
Abstract
The authors describe a rapid implementation of medication treatment for substance use disorders in a value-based organization, delivered in the community-based, interdisciplinary primary care of Medicaid and dual-eligible members. The determinants of increased need are reviewed, as well as the growing opportunity to improve access to treatments, and a template for implementation is shared.
Introduction
Substance use encompasses a spectrum of behavior from lower-risk use to formally diagnosed alcohol and substance use disorders (collectively, SUDs). Mortality related to substance use has been rapidly increasing and has achieved epidemic proportions, with the last known data showing close to 110,000 drug-involved overdose deaths in 2021, 1 a 50% surge over 2019 figures. This substantial increase is often attributed to a combination of an increase in fentanyl and other high-potency opioids in the illicit drug supply, and the combination of stimulants with opioids. 2 –4 This was compounded by the effect of the COVID-19 pandemic, an increase in social isolation, 5 and disruption in access to in-person services for people who use drugs. These services include access to pharmacological treatment for SUDs, including Medications for Opioid Use Disorder (MOUD) and Medications for Alcohol Use Disorder (MAUD), 6 and harm reduction interventions such as Syringe Access Programs, or access to naloxone—an opioid overdose reversal agent, or provision of testing supplies to help assess for the presence of fentanyl before use. 7 The impact of substance use on morbidity is harder to quantify, but SUDs further complicate the course of chronic illnesses (both psychiatric and non-psychiatric 8,9 ) in part due to inherent effects on adherence and engagement (the latter often mediated through stigma and poor experiences with the health care system).
MOUD and MAUD are evidence-based treatments for alcohol and SUDs, 10,11 effective both in specialty care and in primary care, 12 with or without accompanying behavioral intervention. 13 MOUD, in particular, reduces mortality 3-fold and decreases the risk of overdose by up to 80% in opioid users. However, MOUD is utilized less frequently than less effective interventions. 14
The COVID-19 Public Health Emergency declaration in early 2020 resulted in increased flexibility for the prescription of controlled substances, and in particular for the prescription of MOUD using buprenorphine products, allowing for a telehealth visit (using either audio-visual or telephonic communication) to replace the previously required and hitherto mandatory initial in-person visit. In addition, the Consolidated Appropriations Act of 2023 eliminated the need for a special application (a “waiver”) that has been required to prescribe buprenorphine since the passage of the Drug Addiction Treatment Act of 2000 — enabling more primary medical practitioners to provide access to SUD care. Finally, the Medication Access and Training Expansion (MATE) Act of 2023 required Drug Enforcement Administration (DEA)-licensed practitioners to complete 8 hours of continuing medical education related to addiction treatment to renew their DEA license. The combination of these regulatory changes lowered the barriers to access to MOUD services, 15 and provided an opportunity to offer centralized training.
Cityblock is a tech-enabled, value-based healthcare delivery system with medical practices focused on providing high-quality care and whose mission is to radically improve the health of marginalized communities at scale. The population Cityblock serves centers on Medicaid, and Medicaid and Medicare dually eligible members with complex health needs and higher than average utilization of care. Cityblock is structured as an integrated care practice that brings together physical, behavioral, and social care to meet the needs of its members and minimize care fragmentation. Cityblock provides an extra layer of resources to its members rather than attempting to decrease healthcare costs by gatekeeping care. Cityblock’s care model is enabled by prospective value-based payment arrangements with health plans, allowing the flexibility to intervene and invest in dynamic ways that meet members’ complex needs and drive sustainable value. Depending on Cityblock’s contractual arrangement, members are either “attributed” in which case Cityblock practitioners provide longitudinal primary care, or “non-attributed” in which case they provide bridge care. In either case, community health workers facilitate entry into and retention in care and provide care coordination and health system navigation to the members who most benefit from it.
Value-based organizations are uniquely positioned to apply an integrated, harm-reduction-oriented approach to care for members with SUDs and make a sustainable investment in development of adequate programs (Fig. 1). Organizations operating in a value-based payment model ensure that value-creation is tied to improved clinical outcomes rather than to the provision of services, as it is in a traditional fee-for-service (FFS) model. The prospective payment structure is central to enabling Cityblock to tackle problematic alcohol and substance use, as the organization can take a longer view that incorporates both immediate and downstream consequences. Conversely, the results of effective interventions are expected to not only improve the direct consequences of SUDs (eg, overdoses, emergency department [ED] visits, and inpatient hospitalizations [IPs]) but also their further impact on other conditions (eg, HIV, diabetes, hypertension, and prenatal care), leading to an outsized effect on clinical outcomes and total cost of care. Our goal was to provide low-threshold 16 access to MOUD with buprenorphine in primary care (defined as same- or next-day treatment start, harm-reduction orientation, attempting maximum flexibility to accommodate patients) while increasing engagement of potential candidates. This would be accomplished by enlisting outreach staff, community health workers, urgent care practitioners, and all other member-facing staff to meet the members where they are, with respect to their readiness for change. This would achieve the triple aim of improving our member’s experience, improving our population’s clinical outcomes and reducing acute care utilization, 14 the pillars of value-based care.

Integrated services offered to Cityblock members with SUDs. SUDs, substance use disorders.
Methods
Our implementation strategy is rooted in a health equity framework and relies on promoting low-threshold access to substance use care to our members. Historically marginalized communities have less access to substance use treatment 17 due to intersecting realities of race, ethnicity, socioeconomic class, geography, and the structural racism built into the fabric of our healthcare system. 18 This can be seen in the geographic skew of the provider distribution away from communities of color, poor communities, and rural communities. This is compounded by the difficulty of finding convenient treatment while on Medicaid, and the onerous (and frequently, punitive) multi-day intake processes that are often in place for free-standing substance use treatment programs such as Opioid Treatment Programs. 19 These realities are reflected in the lives of our members: 75% are people of color, and 86% are Medicaid or Dual Eligible beneficiaries. The design choices resulting from this strategy will be explored, as well as the ways in which they differentiate this model from that of more traditional provider organizations.
Integrated health approach
Offering a “one-stop-shop” allows for the provision of several important services that are perceived as valuable by the member (including MOUD, MAUD and harm reduction). Integrated care increases the trust that develops between the patient and the care team rather than risk losing a substantial number of members by referring for SUD treatment instead of providing it. 20 This is particularly true in populations that face more structural barriers to accessing care and where follow-up is not assured. Providing access to a medically and socially complex population similar to Cityblock’s is best done in an integrated fashion, along with medical, behavioral, and social care, in an expanded primary care setting.
Initial roll-out in a behavioral health-oriented setting increased visibility and helped solidify the model
Before implementing SUD treatment in primary care, Cityblock started providing it to the members of the Advanced Behavioral Health program. This program serves members who have severe mental illness, SUD, or both, and have high utilization of ED and IP. The program’s interdisciplinary team is weighted toward behavioral health and substance use care and includes behavioral health-trained community health workers, social workers, an addiction specialist, and a psychiatrist. This initial, more targeted setting allowed us to identify needed tools (including Electronic Medical Record, EMR templates and a list of pharmacies that stock MOUD), to evaluate our training needs (both technical and cultural), and to generally optimize our care delivery. It also, crucially, let us increase the visibility of SUD treatment in our organization by highlighting how it helped keep our members engaged in care, and instances where it unlocked the care of our members in a way that would not have been possible otherwise, as the example above demonstrates. Finally, it allowed us to prove its utility where its impact is easiest to measure. By sharing case presentations at monthly all-hands meetings, lessons learned could be reinforced. Grand rounds were also scheduled on harm reduction where a provider in a low-threshold buprenorphine clinic came and shared their philosophy of care.
Internal stakeholders process and buy-in
The first step was identifying all the internal stakeholders who would be affected by the implementation of SUD care, and the role that they would play or the impact the roll-out would have on them (Fig. 2).
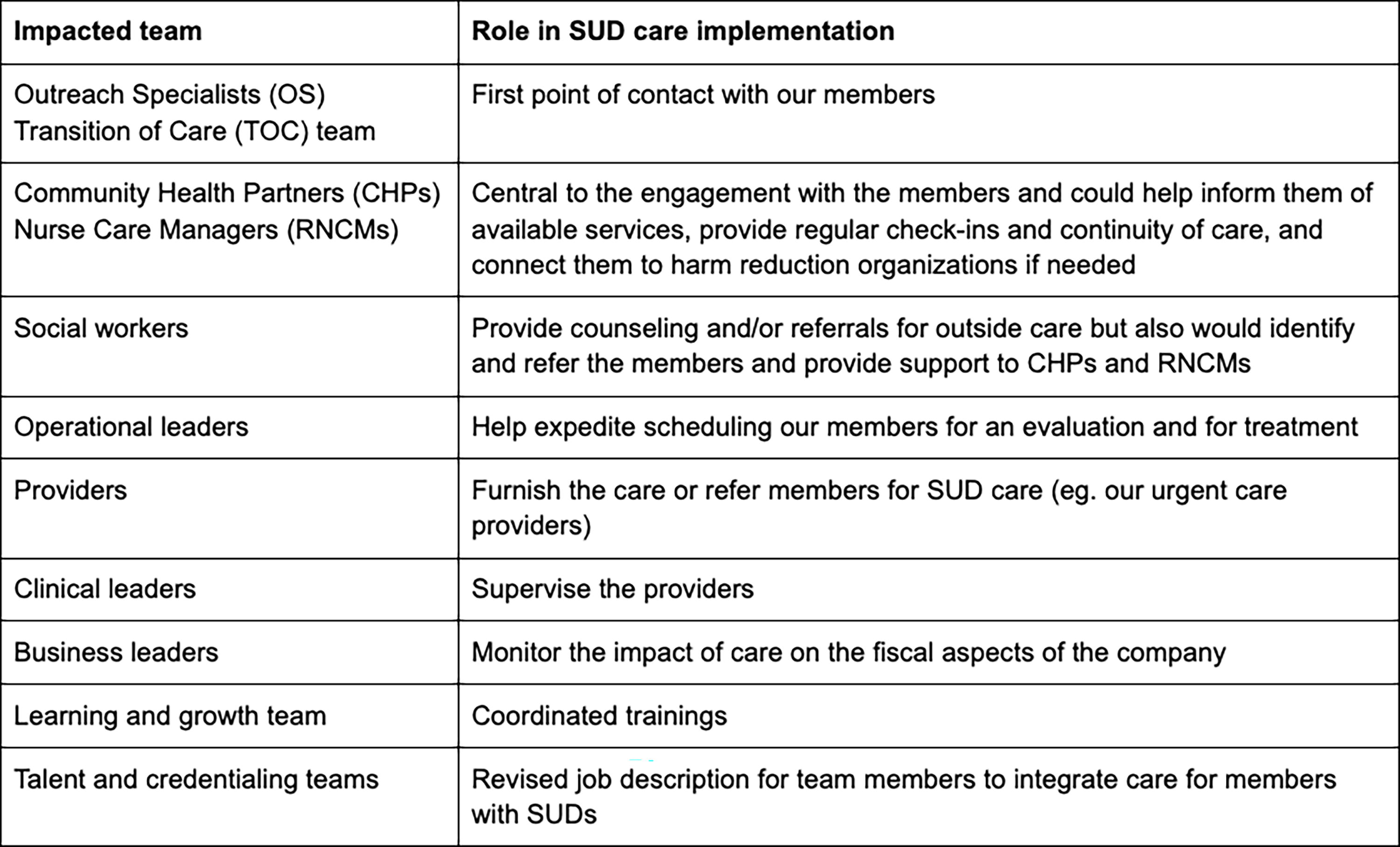
Identified internal stakeholders.
After raising the profile of SUD treatment based on individual examples, buy-in was obtained from the clinical and operational leaders by showing how prevalent SUDs are, and how Medication-Assisted Treatment is effective and underutilized. To prove these points, the expected prevalence of SUDs in our population was highlighted, both by available health insurance claims and by using epidemiological data from the 2022 National Survey on Drug Use and Health. 20 Based on available data, SUDs are more common than diabetes and lead to more annual deaths than car accidents. While there was an obvious clinical quality case for this program, a clear data-driven business case could also be shown by highlighting evidence that suggested that a larger implementation across primary care would enhance our care model. The emphasis was put on the engagement benefits of the intervention (increased adherence and reduced morbidity has been documented in the context of HIV care for patients with SUD 9 ) and on the projected fiscal impact on total cost of care by reduction in ED/IP admissions, in addition to the obvious individual clinical benefit. 21 Cityblock’s Chief Health Officer communicated the importance of SUD treatment and asked Market Medical Directors to prioritize training for our practitioners. The talent team updated job descriptions of primary care practitioners to include provision of MOUD and MAUD, in order to clarify expectations.
Program design decisions
The goal of this ongoing initiative is to integrate safe and effective access to MOUD and MAUD in primary care and within our existing value-based care model without overly increasing complexity of care. Some of the practices that were implemented may not be aligned with the incentives of a FFS model which rewards the delivery of expensive services (such as detox or rehab stays) but they make sense in our value-based model: The downstream improvement in physical and behavioral health outcomes can be weighed against the cost of an intervention, instead of being limited by the arithmetic of margin = cost-reimbursement. To accomplish this, the following decisions were made:
Developing a set of EMR templates and order sets to guide clinical practice and improve efficiency
EMR templates were developed to help with consistent information gathering and for visit documentation in a way that facilitates regulatory compliance and order sets were also developed to nudge practitioners toward evidence-based practices (including screening for other behavioral and medical conditions such as depression, anxiety, trauma, Attention-Deficit/Hyperactivity Disorder, viral hepatitides, HIV, etc.) and to allow them to prescribe efficiently by pre-filling directions and quantities (including on harm reduction supplies). (Both are reproduced in the supplemental data as Supplementary Figure S2 and Supplementary Figure S3.)
Designing and implementing training & clinical support system
Roadshows were conducted in every market to explain the importance of the project, solicit feedback, engage practitioners and care teams in discussion, and surface common negative stereotypes related to the treatment of members with SUDs. During that process, some particular challenges were identified related to culture that were addressed explicitly as the training series was designed: Most practitioners had not received training in MOUD and MAUD and there was a perception that treatment of SUDs was a behavioral health issue rather than a primary care one-even in an integrated care framework. Relatedly, some staff members, including some practitioners and some case managers, while agreeing that treatment was important, expressed discomfort in adopting a harm reduction approach. Some often expressed beliefs, common in 12-step philosophy, that the only acceptable treatment goal is abstinence, or that “people need to hit bottom to change”. This was sometimes the case for staff members with personal or family history of alcohol or substance use. During direct conversations with clinical and nonclinical staff, these cultural and community beliefs were addressed by creating safe spaces for airing dissenting views and validating the beliefs that a particular intervention may have helped someone, while concurrently explaining the treatment choices by tying them to data that support the approach to treatment (such as comparative effectiveness studies).
The new regulation in the MATE Act that requires every provider to complete eight hours of SUD-related training to renew their DEA registration was leveraged by developing a customized curriculum that meets the needs of our practitioners. CME, accredited courses were selected mostly from the Provider Clinical Support System, 28 an organization funded by the Substance Abuse and Mental Health Services Administration to train primary care practitioners in the evidence-based prevention and treatment of SUDs. Selected courses covered the range of outpatient treatment with MOUD and MAUD, but also courses that provide knowledge about the fundamentals of addiction, and of harm reduction. Two one-hour-long courses were commissioned through the Centers for Disease Control and Prevention’s National Harm Reduction Technical Assistance Center and designed in collaboration with a harm reduction psychologist 29 to help inform the internal culture of the organization. The harm-reduction courses were taken by both practitioners, social workers, paramedics, community health workers, and all member-facing staff—representing about 600 individuals. The training was also integrated into the onboarding process for new staff members. Completion of the course was tracked and regular feedback on progress was provided to staff members and supervisors. The completion of the courses correlated with a significant increase in the prescription of MOUD and MAUD as shown in Figure 3.

Training completion of providers and member-facing staff.
In addition to the training, a clinical support system for staff and practitioners was implemented. It combined (1) a bi-monthly forum where members are discussed both from clinical and social standpoints with (2) the accessibility of same-day (and often real-time) consultation from a primary-care trained addiction medicine specialist (the “consultant”). practitioners and care-teams can ask the consultant questions through private messaging, meet to discuss a member (often by inviting the consultant to the team’s case conference), and ask the consultant to participate in the clinical encounter—at first as an active participant, then as an observer.
Mapping out timely access and follow-up
Developing a plan for timely (ideally same-day) access for initial appointment and for follow-up appointments is crucial and needs to account for missed appointments. Our scheduling system was set-up so that MOUD appointments are prioritized and can be made with any available provider rather than the patient-assigned provider. For a same-day appointment, any provider that has a “no-show” is able to see the patient. The initial information gathering can be accomplished by the provider or other staff members (for example a social worker, pharmacist or care navigator) and documented in templated form. The patient can then see a provider for a short initial appointment where they will be prescribed MOUD, if appropriate. A longer appointment can be scheduled for follow-up.
Building tools allowing for visibility of provider prescribing practices
The built-in function of our EMR was used to produce a monthly report of all Food and Drug Administration-approved MOUD and MAUD prescriptions sent by the practitioners. This data was then analyzed and a few metrics were extracted including the number of practitioners having ever written MOUD or MAUD prescriptions, the overall number of prescriptions written for each category, each month, and the monthly number of prescriptions for each individual provider. This data was used to gauge overall progress of the implementation, and to reach out to practitioners who were not prescribing any MOUD or MAUD to provide assistance.
Results
Training and prescribing practices of practitioners
The two waves of training happened gradually, practitioners first followed by member-facing staff (Fig. 3). A similar gradual uptick of the number of prescribers who had ever prescribed MOUD or MAUD was also observed (Fig. 4)—suggesting that the training has made prescribers more willing to discuss and prescribe those medicines.
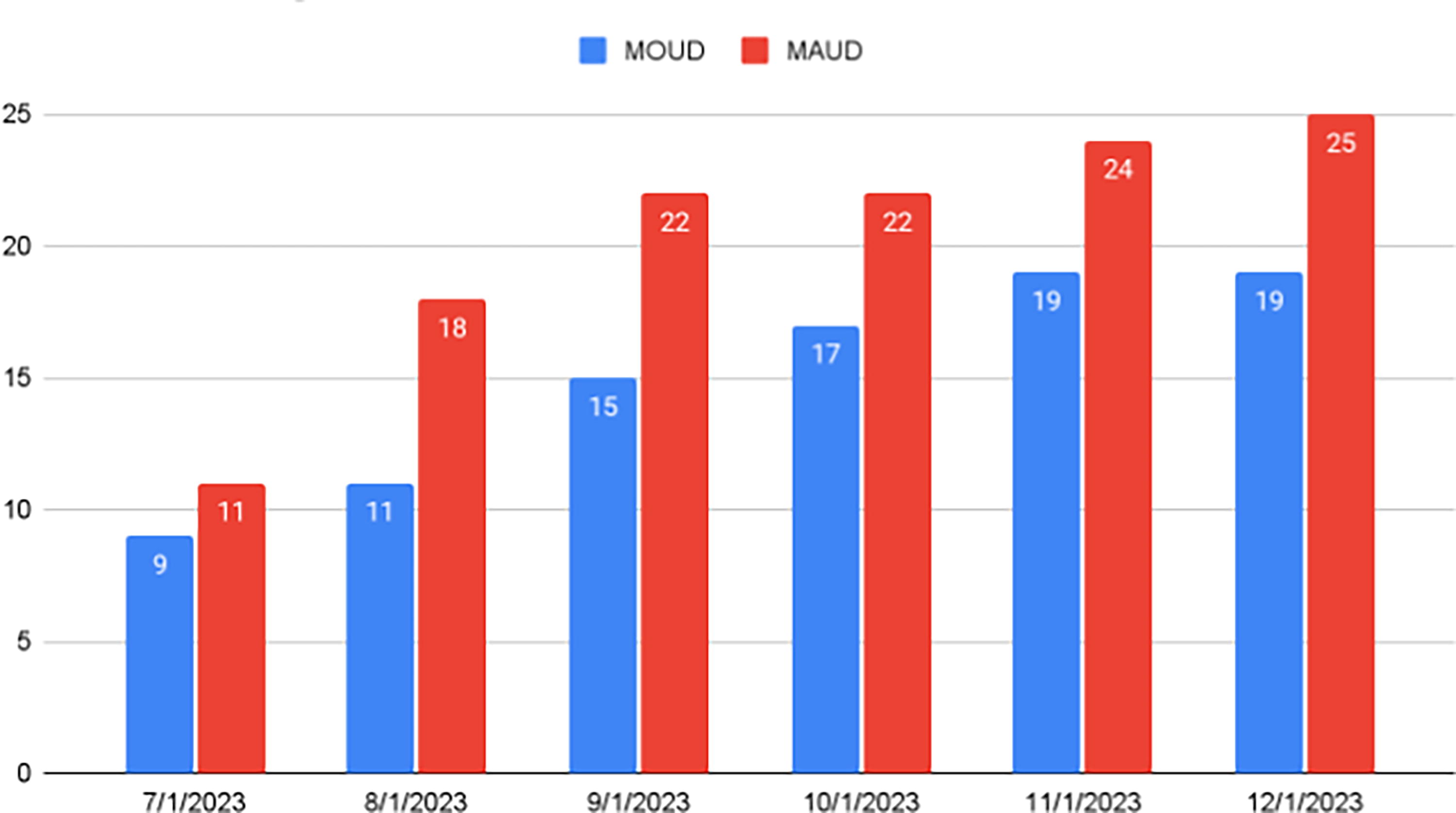
Increase in number of providers ever having written a prescription for MOUD or MAUD. MOUD, medications for opioid use disorder; MAUD, medications for alcohol use disorder.
Number of members receiving MOUD or MAUD
Figure 5 shows a steady increase in the number of unique members being prescribed MOUD or MAUD each month. The monthly number of members being treated is increasing slowly, whereas the total number of members having ever received these medications is increasing quickly. The size of the population ever treated more than tripled from a baseline of 38 members at the start of the implementation of our structured program to 119 members four months later.
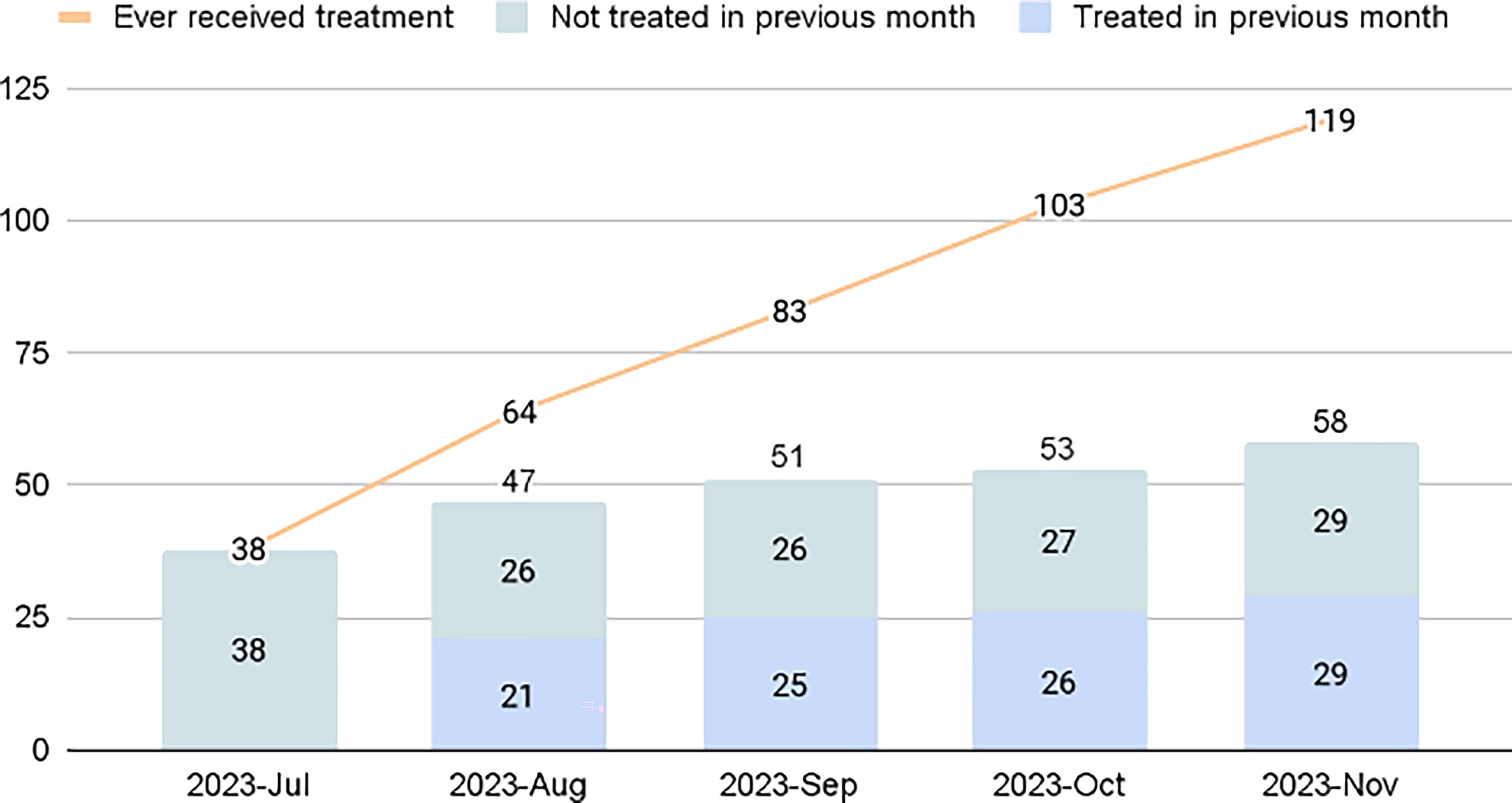
Monthly unique members receiving MOUD, MAUD or naloxone. MOUD, medications for opioid use disorder; MAUD, medications for alcohol use disorder.
Retention in SUD care
Once a patient receives a prescription for MAUD or MOUD, we consider the receipt of a prescription the following month as a measure of retention in SUD care. Figure 5 also illustrates expected challenges in retention in care as 51% to 55% of members are retained in SUD care month-over-month.
Taken together, observations (2) and (3) suggest that while the increase in monthly members receiving SUD treatment seems modest, it belies the underlying dynamics that display a high turnover of the members receiving MOUD or MAUD.
Discussion
A structured training program coupled with systematic reporting and monitoring of ongoing prescribing practices allowed for the quick implementation of SUD care in primary care, using MOUD and MAUD. Although the program’s retention in care is in line with the range of expected retention rates for OUD care nationally 30 —particularly for such a recently implemented program—the results highlight the need for more robust interventions to increase adherence and retention in treatment.
An example of the powerful impact of MOUD can be found in the trajectory of one of the members who was pregnant and using non-prescribed opioids. She had avoided initiation of prenatal care for fear of being reported to the authorities and criminalized, or of losing custody of her soon-to-be baby. The disclosure she made to a provider she already had a trustful relationship with on her primary care team led to discuss treatment with buprenorphine and start her on it that very day. This allowed her to regain agency and start receiving prenatal care. She gave birth to a healthy baby and continues treatment with buprenorphine.
There were several limitations that should be addressed in further evaluations. Although there was an improvement in MOUD and MAUD prescribing, the short duration of follow up limited the ability to obtain longer term data for retention in MOUD and MAUD care and medication adherence. Retention in care and adherence to the prescribed treatment are important quality measure as they correlate to positive outcomes, including decrease in nonfatal overdoses, 31 decrease in relapses, 32 decrease use of acute care services (including inpatient addiction services) and increased engagement in outpatient services (including outpatient addiction services). 33 Obtaining longer term medication adherence data will require an extension of the evaluation and allow testing strategies to increase retention in care. For example, using a registry to track the MOUD and MAUD prescriptions would enable our care team to be alerted when a member runs out or is about to run out of medication, so that they can be outreached proactively. In addition, whether the highest risk groups in the population were engaged is an open question. Is there a difference between the members that were engaged as opposed to those who are more difficult to reach and less likely to accept treatment?
As our cohort is followed for a longer period of time, it will be important to look for the ability of treatment to not only change the direct outcomes in substance use but also the participant’s overall physical and mental health. As the members’ alcohol and SUDs are better controlled, one should witness an improvement in the management of their chronic conditions including ubiquitous conditions such as diabetes, hypertension, congestive heart failure and major depressive disorder. Beyond the clinical outcomes, a value-based SUD initiative must include an evaluation of the financial viability of such an approach. It needs to address whether this approach leads to decreased health care cost and inappropriate utilization in our cohort, consistent with what has been observed in earlier studies which showed that a treatment of opioid use disorders led to a reduction in utilization of high cost medical care. 33 Implementation of Medication Assisted Treatment and harm reduction interventions is cost-effective at the societal level, 34 but the financial implications at the level of care delivery organizations will depend on their care model and should be the subject of further examination. This examination should include both clinical and financial improvements at the level of the organization, as well as improvement in rates of complications from substance use (including death) in the larger community. For instance, could this tactic be deployed in a hot spot such as Kensington in Philadelphia to improve the condition of the individuals and the communities affected by substance use, as it is an approach that is consistent with the Philadelphia Substance Use Treatment Recommendations formulated in 2020. 35 Future evaluations should also consider our approach through a health equity lens. Although this particular intervention was focused on an underserved population that is majority–minority, was our goal of improving equity in the area of substance use treatment achieved?
We recognize that several aspects of the implementation for MOUD and MAUD that we describe are easier to enact in an integrated, interdisciplinary setting, enabled by a prospective value-based payment structure. Many of those lessons, however, are still relevant to community-based and academic-based practice, irrespective of their care model: (1) Concentrating on implementing MOUD and MAUD treatment for SUD in primary care: medical practices are often worried about the investment required to set-up SUD treatment; their leadership often conceptualizes SUD treatment as a behavioral health endeavor that relies on counseling. Where integrated care remains a promise, adopting a medical model rather than a behavioral one can ease many of these concerns, in addition to destigmatizing care for people with SUDs. (2) Stigma and negative biases toward people with SUDs pervade the healthcare system, recognizing and addressing the need for culture change explicitly, through training and open discussion is essential to success. A change-management framework that centers on identifying and consulting all stake-holders through the design and implementation processes can lead to identifying both operational bottlenecks and cultural challenges. (3) Adopting harm reduction philosophy and practices: The culture of SUD treatment is moving away from the punitive and adversarial culture that characterized it in the past. Recognizing that the goals of treatment should be individualized based on patient preference helps provide good care that aligns with the way other conditions are treated; it also improves rapport building and minimizes instances where the care team gets stuck, sometimes resulting in unnecessary discharge from treatment. (4) Providing low threshold access: while all medical practices may not be set-up for same-day or next-day access, choosing simple protocols similar to the ones described here, minimizing the information that is obtained before induction, not requiring lab obtention before the start of treatment, implementing at-home induction and, where available, leveraging telemedicine can all contribute to lowering barriers to access.
Conclusion
As the number of Americans dying of substance-related causes continues to increase it is imperative that our health care system seeks out innovative ways to address this epidemic. 36 A structured training program created within the confines of a value-based health care structure was able to effectively upskill primary care practitioners in treatments for alcohol and opioid use disorders, as well as an entire care team in the tenets of harm reduction. The combination of practitioners’ increasing comfort with SUD treatment combined with activating the non-clinical members of the care team with tools and workflows created an appropriate synergy that translated to vast improvements in prescribing MOUD and MAUD for patients with SUDs. This led to an increase in both the number of practitioners prescribing SUD treatment, and the number of unique patients receiving it every month.
As these types of interventions are scaled, they need to be implemented in an intentional way that addresses health inequities, ensuring the program is not exacerbating already existing disparities.
Footnotes
Acknowledgments
The authors would like to thank Pooja Mehta, MD for helpful feedback on an early version of this article and Jenny Edelston for editing.
Authors’ Contributions
D.D.R. contributed to conceptualization, methodology, writing—original draft, project administration, and supervision. S.S. contributed conceptualization, writing, reviewing, and editing.
Author Disclosure Statement
The authors are employees of Cityblock Medical Practice, P.A. and receive compensation and benefits from Cityblock Health, Inc. All medical services are provided by licensed physicians and health care practitioners employed by Cityblock Medical Practice, P.A. Cityblock Health, Inc. provides management and administrative services to Cityblock Medical Practices.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.