
Abstract
Screening for social determinants of health (SDOH) has been mandated by health systems nationwide. However, a gap exists in closed-loop referral for care coordination between health care and social services. This article presents the framework of a technology-based project to facilitate closed-loop referral between health care and social service agencies in Greater Houston by leveraging and connecting the existing care coordination technology infrastructure. Ten health care and social service organizations in Greater Houston participated in the demonstration project initiated in January 2023. The authors leveraged and linked regional health information exchange (HIE) technology with a master patient index of >18 million, and sector-specific care coordination platforms to build closed-loop referral capacity between HIE-participating health care organizations and social service organizations to meet patient SDOH needs. Evaluation efforts will assess the reach, adoption, implementation, and the effectiveness of the closed-loop framework in improving social and health outcomes. The framework comprised the following 4 components: (1) establishment of collaborative governance for shared decision-making processes, fostering trust, alignment, and transparency among organizations; (2) development of technology linkages between existing platforms to facilitate seamless referrals between organizations and ensure visibility of referral outcomes; (3) integration of regional resource directories into technology infrastructure to ensure resource accessibility/quality; and (4) evaluation of the system’s impact on health equity, efficiency, and cost reduction. This project aimed to close the loop for care coordination between health care and social service agencies, enable data evaluation to determine care coordination effectiveness, and lay the foundation for SDOH-related research/practice equitably.
Introduction
Social determinants of health (SDOH) needs, such as lack of food, housing, transportation, and access to care, are the root causes of poor health outcomes and inequities in the United States. 1 Health care organizations seek to address these factors by referring patients to social/community services. Despite these social/community service programs gaining popularity in the United States, there is currently no standardized national system for health care providers to make or track referrals systematically to “close the loop” (i.e., bidirectional information sharing and communication between practices, including making referral requests to specific agencies, and timely and clear communication response regarding the referral). 2 The lack of systematic referral tracking has resulted in patients not receiving the social services needed to manage health conditions and maintain health. According to the Centers for Disease Control and Prevention (CDC), less than 50% of referrals are being completed (ie, patients receiving the services) and a recent analysis of Houston food prescription programs demonstrates similar rates of incomplete referrals. 3 Rates are even lower for mental health services, with studies reporting that only 10% of referrals from primary care providers to mental health services result in patients accessing psychosocial care. 4,5 Several regional technology efforts are underway to facilitate care coordination for social needs. However, these efforts are largely siloed and often require participating organizations to adopt a new, common technology to engage with these platforms.
This urgent need is further underscored by recent mandates from the Centers for Medicare & Medicaid Services (CMS), which state that hospitals reporting to the Inpatient Quality Reporting program and the Merit-based Incentive Payment System are to submit 2 new SDOH measures, which are associated with payments. These measures were voluntary in 2023 and became required starting 2024. 6,7 In addition, the National Center for Quality Assurance published new Healthcare Effectiveness Data and Information Set quality measures for SDOH screening and response required by health systems and health plans nationwide. The Joint Commission also published its Health Care Equity Certification in July 2023, providing voluntary guidance and new accreditation for screening and referring patients to services for social needs. 8 These changes warrant a strong SDOH referral infrastructure for health care and social service organizations.
The Health Equity Collective (Collective) is a systems coalition in the Greater Houston region consisting of over 200 organizations with a singular purpose of improving care coordination for SDOH across sectors using a collective impact approach. 9,10 The Collective is facilitating the development of the governance, technology, and human capacities needed to build, implement, and scale closed-loop referral infrastructure in Greater Houston that leverages the local health information exchange (HIE), linking it to social services that improve care coordination for SDOH needs. Based on consensus across the Collective’s member organizations, the priority initial system change needed is to establish closed-loop referral capacity between health care and community-based organizations (CBOs).
An effective closed-loop referral infrastructure links health care organizations and social service providers via technology-shared data standards, and complementary human-based workflows to better meet patient needs. While different care coordination technologies that are interoperable with electronic health records (EHRs) already exist, these platforms are largely siloed with one-off care coordination between one health care and one social service organization at a time. This creates inefficiencies and may be burdensome for social service organizations that have to make these individual connections to one health system at a time. Our demonstration project aims to address these inefficiencies by leveraging existing regional care coordination assets and connecting them to create a broader ecosystem of care coordination. This includes the HIE for southeast Texas that links to >90% of the patient records across the region and has a master patient index (MPI) of >18 million, of which 8 million+ lives are in southeast Texas. Over 90% of the southeast Texas region’s health care sector organizations participate in the HIE and patient health information data can flow across the participating health care organizations in real time. Our article presents the design and framework of the demonstration project that leverages the regional HIE and sector-specific care coordination platforms to build closed-loop referral capacity between HIE-participating health care organizations and social service organizations to meet SDOH needs.
Methods
This demonstration project is being implemented by the Collective systems coalition. Ten organizations in the Greater Houston region were recruited to participate in the project initiated in January 2023. These include 2 large hospital systems (Healthcare organization (HCO) 1 and HCO 2), 1 federally qualified health center, 1 community health center, 1 organization providing mental and behavioral health services, 1 statewide nonprofit organization that provides a technology platform to coordinate care across social services (CBO Hub 1), 1 local CBO providing direct services and also facilitates care coordination between social service organizations (CBO Hub 2), 1 local nonprofit providing direct services (CBO), 1 local HIE, 1 nonprofit organization leading the development of collaborative governance, 1 for-profit company that will build the technology solution for closed-loop referral, and an academic institution (UTHealth Houston) that serves as the backbone organization of the Collective and provides project oversight. All participating health systems primarily serve low-income populations in high need of social services, are already screening patient populations for SDOH needs, are members of the Collective, and indicated interest in being early adopters of interoperable care coordination efforts to meet patients’ health-related social needs. This project has been reviewed by the University of Texas Health Science Center at Houston Committee for Protection of Human Subjects and deemed IRB exempt.
Results
There are 4 main pillars of our closed-loop referral demonstration project as follows: (1) building a sustainable collaborative governance (shared decision-making processes), including governance for data sharing; (2) building technology capacity for referrals for social services between organizations, including closing of the loop such that providers across all agencies can see if the referrals have been successfully fulfilled; (3) linking valid resources directory to the referral infrastructure; and (4) evaluation and sustainability—evidence points to the potential impact of this infrastructure in improving health and health equity while reducing costs. Yet, there is no assessment of such type of efforts in reducing social needs and improving outcomes. This evaluation, to be conducted as part of this demonstration project, will inform future sustainability and scalability of this effort beyond the demonstration project.
Building collaborative governance
Collaborative governance is critical to the success of our closed-loop referral project. Leading with technology first does not address the underlying issue of lack of transparency across organizations and sectors. Our approach addresses the general lack of precedence business cultures investing in trusting, collaborative relationships. This is a purposeful and sustainable configuration of people, data, systems, and tools to “collaboratively” achieve a collective goal or address common barriers. Our shared governance process establishes collectively agreed-upon steps and specifications by which members will link together, share and use data, and coordinate care linking existing workflows. This process involved collecting data and data use requirements from each organization and facilitating consensus on the specifics of data sets, data use, and workflows for use in the demonstration project. The consensus-building process was a series of conversations within and across all the participating organizations, culminating with large group convening.
Transparency in governance layers enables organizations interested in participating to understand expectations and requirements for participation, and what data, data uses, and users have already been approved. The steps of the collaborative governance process currently being used in our project are as follows: (1) Design—to build trust, develop a charter by identifying collective goals, pain points, data needs/uses, and key data partners among participating organizations. (2) Develop—work with the organizations to discover existing organizational data, technology, and governance specifications. These specifications were organized into must have, would like to have, and cannot have categories. These data-sharing categories were informed by existing data-use standards, patient/client privacy regulations (eg, Health Insurance Portability and Accountability Act (HIPAA)), patient consent procedures, legal guidance, and organizational practices. Then, a minimum data sharing set was established from these organizational specifications during a half a day collaborative workshop with all participating organizations. Technology design was built upon the data-sharing and existing technology uses for each organization, generating a blueprint for interoperability across organizations and sectors. Current organizational workflows and human capacities were gathered from each participating organization via survey. The survey results were analyzed to inform linkages and workflows. We also obtained input from the community members directly on how they like to receive social services. These results also informed the shared metrics of impact and baseline operations for process evaluation (key performance indicators) as seen in the logic model (Figure 2). The next step is to execute the scope of work and begin implementation, and ongoing evaluation of the shared processes. (3) Implement—we will make changes to the scopes of work and charter from implementation and ongoing evaluation and feedback loops, and the development of a governing body. (4) Iterate—we will seat a governing body to manage and monitor implementation, identify new partnerships, and make expansion decisions. While the collaborative governance framework is critical to identifying the data, technical, and governance specifications needed for organizations to participate, the process by which it is facilitated also helps level the playing field for all organizations to participate and meet them where they are, by linking to existing workflows and accommodating existing systems/structures. In addition, the collaborative governance process builds transparency and communications, which are invaluable for developing trust and understanding among participating organizations, needed to overcome complex issues related to data sharing and use.
Building technology capacity for closed-loop referrals for social services between health care-based organizations and CBOs
Figure 1 outlines the technology framework and architecture of the care coordination ecosystem for closed-loop referral. All participating health care organizations are already part of the local HIE. The technology solution (Channels360® from Ready Computing Inc.) will integrate with the HIE via Application Programming Interfaces (APIs) and allow for HIE-participating health systems to send patient referrals for SDOH to social service organizations. Furthermore, the Channels360® solution links via APIs with the participating CBO hubs to allow for the referral to be made to their network social service agencies who can then accept or reject the referral within the platform. By leveraging the HIE MPI, the technology builds sightlines for HIE-participating health systems on referrals made so that they can see within the technology platform whether their patient has been previously screened, referred, and received the service elsewhere in an HIE-participating health system. This technology solution also facilitates interoperability by which the participating organizations are connected using their existing technology infrastructure to facilitate referral exchange.

Conceptual model of technology-based closed-loop referral between health care and social service agencies in the Greater Houston region.
Linking resources directory to the referral infrastructure
Effective care coordination requires reliable information on resources and services available. In preparation for the closed-loop referral, in 2021–2022, the Collective facilitated the development of a regional resource directory exchange infrastructure. This resource directory exchange linked the 3 local and active resource directories together, with regional 211 resource data. Linkages were developed via APIs and this resource directory exchange is in alignment with the Inform USA 11 and Open Referral data 12 and interoperability standards. The resource directory exchange was designed to link information on resources and improve the quality of the resource information across all sources. This resource directory exchange will support the closed-loop referral demonstration project. It will be linked to the Channels360® technology solution’s existing resource directory, providing access to the expanded network of resource directories.
Evaluation and sustainability
A critical aspect of this project and its sustainability is understanding the process and impact of this closed-loop referral infrastructure on the regional care coordination efforts. In the long term, we will assess the impact of this closed-loop referral capacity on improving health equity, creating efficiencies, or reducing costs. The logic model and theory of change are outlined in Figure 2. We will use a mixed-methods evaluation approach for this effort across stakeholder groups. We will use the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) framework to guide the evaluation. 13 The regional HIE receives Health Level 7 version 2 real-time feeds from their participating health systems to create a unique Consolidated Continuity of Care Documents (C-CDA) for each patient, which is converted to a relational database with individual patient’s longitudinal electronic health data. The C-CDA will also include social service referral and uptake data for each patient. We will create a customized EHR-based cohort of individuals who have received referrals through the platform to assess effectiveness. In addition, we will obtain qualitative and quantitative data using key informant interviews and surveys, respectively, from the staff at participating organizations to inform the implementation and adoption of the closed-loop referral technology solution. We will also conduct interviews and surveys with patients to obtain information regarding satisfaction with the coordination of and access to services. Electronic medical data will be used to assess the impact on social and health outcomes at the individual patient level. 14 We will also leverage various national efforts to inform our evaluation, such as the Gravity Project, 15 Civitas Networks for Health, 16 ONC Social Determinants of Health Information Exchange Learning Forums, 17 and CDC Social Determinants of Health Use Case Workgroup. 18
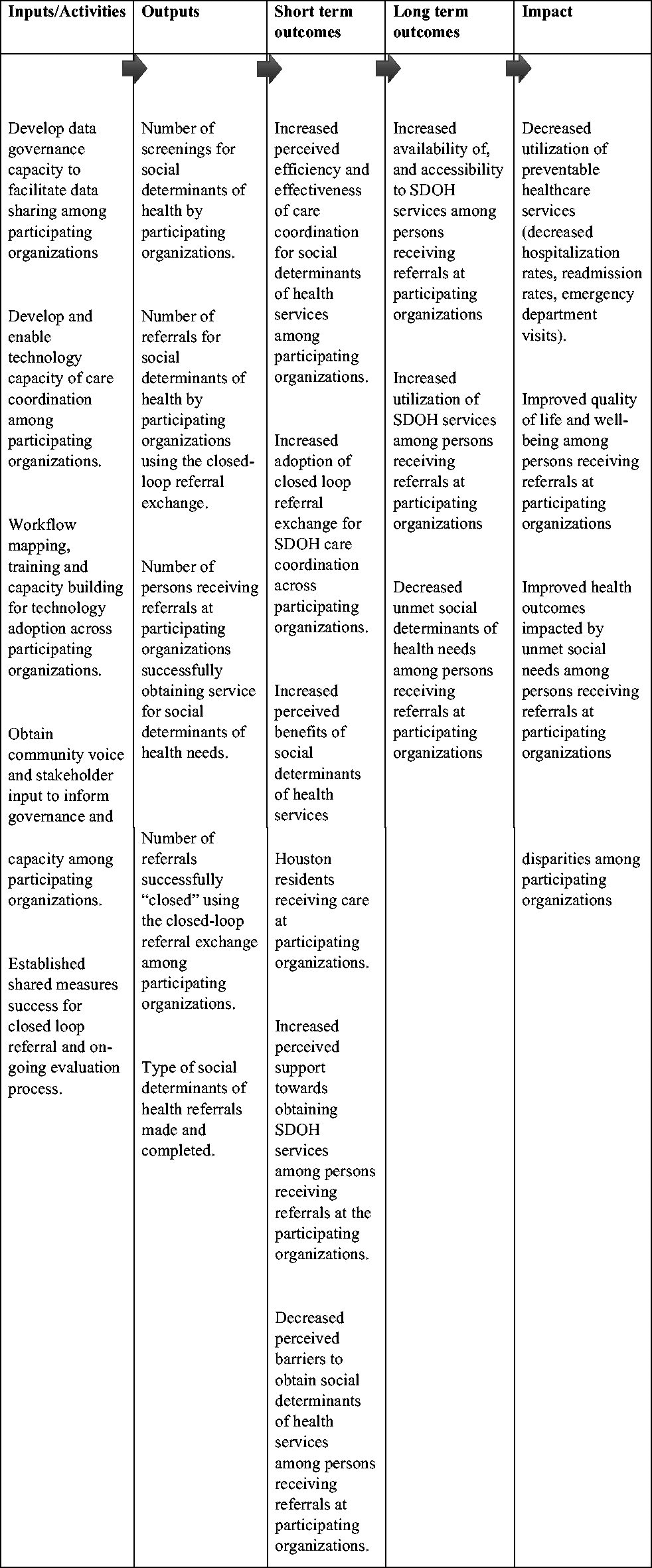
Logic Model and Theory of Change for Closed-Loop Referral Demonstration Project. Closed-loop referrals are defined as bidirectional information sharing and communication between health care and social service agencies, including making referral request to specific agencies, and timely and clear communication response regarding the referral completion, cancellation, or no-shows. SDOH, social determinants of health.
Discussion
The impetus for this project arises from the challenge that despite the increasing popularity nationwide among health systems to screen for SDOH, the uptake of the services falls short due to a lack of care coordination and closed-loop referral between health care and social services. Closed-loop referrals are defined by the CMS as bidirectional information sharing and communication between agencies, in this case—health care and social service agencies, including making referral requests to specific agencies, and a timely and clear communication response regarding the referral completion, cancellation, or no-shows. 2 An ideal care coordination solution should allow for referring agencies to log and track every referral request through completion. Receiving agencies should also log referrals and notify requesting agencies of the referral request disposition, including appointment date and time, and if referral is not appropriate or if unable to schedule. Subsequent cancellations or no-shows should also be communicated. Following a referral visit, the receiving practice should send a timely and clear response note to the referring agency. However, privacy laws such as HIPAA make it challenging for health systems to seamlessly share data with CBOs directly. 19 As a result, there has been a concurrent burgeoning of technologies that offer care coordination services to health systems and social service organizations. However, each technology solution offers varied services, with limited interoperability, and operate in competition with other similar care coordination technologies, or even within themselves when they are implemented across different organizations. This has resulted in numerous siloed care coordination across the region, and sometimes even within the same organization, resulting in care navigation that may too often be redundant, conflicting, expensive, and inefficient. This is especially burdensome for social service organizations that have to make these individual connections with disparate technology platforms adopted by each individual health system partner to provide the social services needed. With a growing number of these technology solutions, the Collective’s shared opportunity is leveraging and link existing disparate regional care coordination technologies and cultivating interoperability across organizations with their existing systems to allow for population-level care coordination and the capacity to measure health impact across the region.
It is important to note that efforts to augment care coordination are underway nationally and in Texas. For example, in Texas, a recently published pilot study demonstrated a digital platform in Central Texas that successfully matches, links, and visualizes patient-level information and community-level deidentified data from across health care and social service sectors. 20 In 2022, a systematic review of 19 programs offering coordination of health care and social services in the United States showed that a majority of these publications facilitated human capacity of care coordination for SDOH services using face-to-face, in-person, or telephone communication to engage patients and coordinate care, none that tested technology to facilitate care coordination. 21 This study adds to the literature in this space to share models, frameworks, and learnings of leveraging and connecting existing technologies and infrastructure to create a broader ecosystem for care coordination.
It is important to recognize the notion of selecting one system or one platform for all data sharing and integrations are obsolete for the Greater Houston region given that most organizations have already invested in disparate care coordination technology platforms. The burden on existing staff to adopt a new system or restructure their existing systems and procedures is too great. Single-system solutions often end up being so complex that they are difficult and expensive to manage over time. Technology can now support broader “interoperability”—the connection of disparate systems through common data standards and APIs, 22 which is central to this study’s efforts. Interoperability also enables collaborating organizations to share responsibilities and risk and leverage each other’s technology, tools, and capacities. Shared technology also allows organizations to take responsibility for a piece of the system, alleviating the financial burden on all by spreading it across many. Shared governance ensures that connected and integrated systems only allow access to and use of data for agreed-upon purposes by approved users. These uses are managed, monitored, and sustained by the participating organizations, collaboratively through the Collective. Our demonstration project will create an ecosystem of interoperability between health care and social service organizations in a region that has already adopted multiple, disparate care coordination technologies to coordinate care for social needs. Given that the participating organizations are members of the Collective with a strong history of building trust and engagement using a collective impact approach with 200+ organizations since 2018, specifically on care coordination for SDOH, makes it the strongest anchor for this effort. 9 The estimated timeline for the demonstration project is January 2023–December 2025. By the time this article was written in spring 2024, the initial legal agreements and contracts between the participating organizations were finalized, the collaborative governance process was completed, and the design for the closed-loop referral technology solution was finalized. Estimated implementation and testing of the closed-loop referral are expected to be initiated starting fall 2024, with evaluation efforts concluding in December 2025.
There are several strengths to our project’s approach. First, the Collective is using a collaborative governance model that establishes collective decision-making and governance to meet goals shared across participating organizations. Governance structure and process are collaborative, eliminating traditional power imbalances (one organization imposing its will on others) and providing all organizations and users with a voice in how their respective data are used and by whom. Governance framework includes safeguards to protect sensitive data, such as limiting the use of combined data to specific approved purposes, and restricting data access to only those who need it to serve patients and clients, or for another approved use. These safeguards and restrictions can be adjusted via the governance processes over time to meet the evolving needs of the collaborations and those they intend to serve. Data-contributing organizations maintain ownership of their data and control its use and by whom. This model eliminates redundancies and reduces administrative burdens related to data sharing, integration, and use, and leverages existing technology, data, knowledge, and relationships. It provides a safety net for organizations to engage in data sharing, especially with new partners. Technology tools are developed after the shared governance processes are developed, that is, technology follows governance. To maintain the shared vision throughout the closed-loop referral development process, the governance process uses shared metrics of impact with clear, shared descriptions for each deliverable item. Another strength of this approach is the utilization of a human-centered design approach where we gathered the voices of the community members to inform the governance and technology. This approach has been demonstrated in other studies involving patient-users in the design and testing ensured functionality and usability, therefore increasing the likelihood of promoting the intended health outcomes. 23 In addition, there is limited evidence on the effectiveness of shared workflows and decision-making across sectors for addressing SDOH. The demonstration project will add to this evidence base. Finally, this demonstration project leverages the HIE with an MPI of >18 million, of which 8 million+ unique patients are across 75 counties in southeast Texas, and if found to be successful, could be scaled rapidly across this region through the HIE.
A limitation of this collaborative ecosystem design is that change happens at the speed of trust established across the participating members. Trust-building takes time, and generally, relationships are built upon histories, both positive and negative engagements across sectors, organizations, and even individuals. Systems change can be complex, nonlinear, and requires operating beyond the typical organization-centric strategies and hierarchies. This type of collaboration requires shared decision-making, while still accommodating participating organizational needs. 24
Conclusion
In summary, this closed-loop demonstration project will enable coordination of care between social service agencies and health care institutions by linking existing care coordination technology infrastructure, developing the ability to evaluate data to determine best practices, referral effectiveness, and creating the foundation for SDOH-related research and practice effectively and equitably.
Footnotes
Authors’ Contributions
S.V.S., H.M.P., M.S., D.G., C.P., K.M., J.H., J.G., and E.B. were involved in the design, protocol development, evaluation measures, writing, and critical review of the article. S.V.S. and H.M.P. conceptualized the article. All authors provided final approval of the article.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work is supported by funding from the Episcopal Health Foundation, Cullen Trust for Healthcare, Rockwell Fund, the Powell Foundation, and UTHealth Houston School of Public Health.