
Abstract

Telehealth (TH) services and the social determinants or drivers of health have both been primary foci of policy development for the Center for Medicare and Medicaid Services (CMS) since the COVID-19 pandemic. Licensure and billing regulations passed for TH have led to a rapid expansion of the digital health technology sector. The social determinants of health (SDOH) have never been more exposed or exacerbated than following the height of the pandemic. The two fields have become increasingly intertwined as TH has been shown to increase access to care. 1 Recently, TH has also been emerging as a tool to identify and address the SDOH. 2 However, the potential for TH to bridge the gap for patients with complex health and social needs has not been fully realized. An analysis of CMS’s billing regulations reveals why there has not been widespread adoption and how this may change in the future.
CMS has repeatedly brought attention to the SDOH since the height of the pandemic. For example, a 2021 “Roadmap for States to Address SDOH” outlined various programs that states could utilize to combat health disparities. While such initiatives raise awareness by highlighting established programs, there are two primary limitations to encouraging future action. Although such proposals may cover the services that would address a patient’s disparity, such as transportation to and from appointments, there is a lack of reimbursement for the necessary upstream actions of identifying and initiating the enrollment of at-risk patients. This limitation highlights an underlying challenge to creating a culture of value-based care in the contemporary health care system; while addressing health disparities may be justified in terms of patient outcomes, how can health systems justify the sustained support of such programs in terms of the bottom-line?
CMS is taking the first step towards addressing this limitation in the 2024 Physician Fee Schedule. Under a newly designated G-code providers can now bill for the collection of a SDOH Risk assessment every 6 months. G-codes can be best thought of as “safety net” codes, or those used for capturing services not covered by Current Procedural Terminology (CPT) codes. 3 There are many types of services covered by G codes. These include preventative services, such as alcohol misuse screening, quality incentive programs, confirming specialist referrals, and even TH services, such as an initial patient visits. 3 They are also used to document patient’s physical impediments to treatment or consultation, such as mobility limitations. (CMS—Functional Reporting) G-0136 is the first G-code that allows physicians to be reimbursed for collecting SDOH data. The details of these assessments per the 2024 Physician Fee Schedule can be seen in Figure 1. (Medicare Learning Network Health Equity Services in the 2024 Physician Fee Schedule Final Rule)
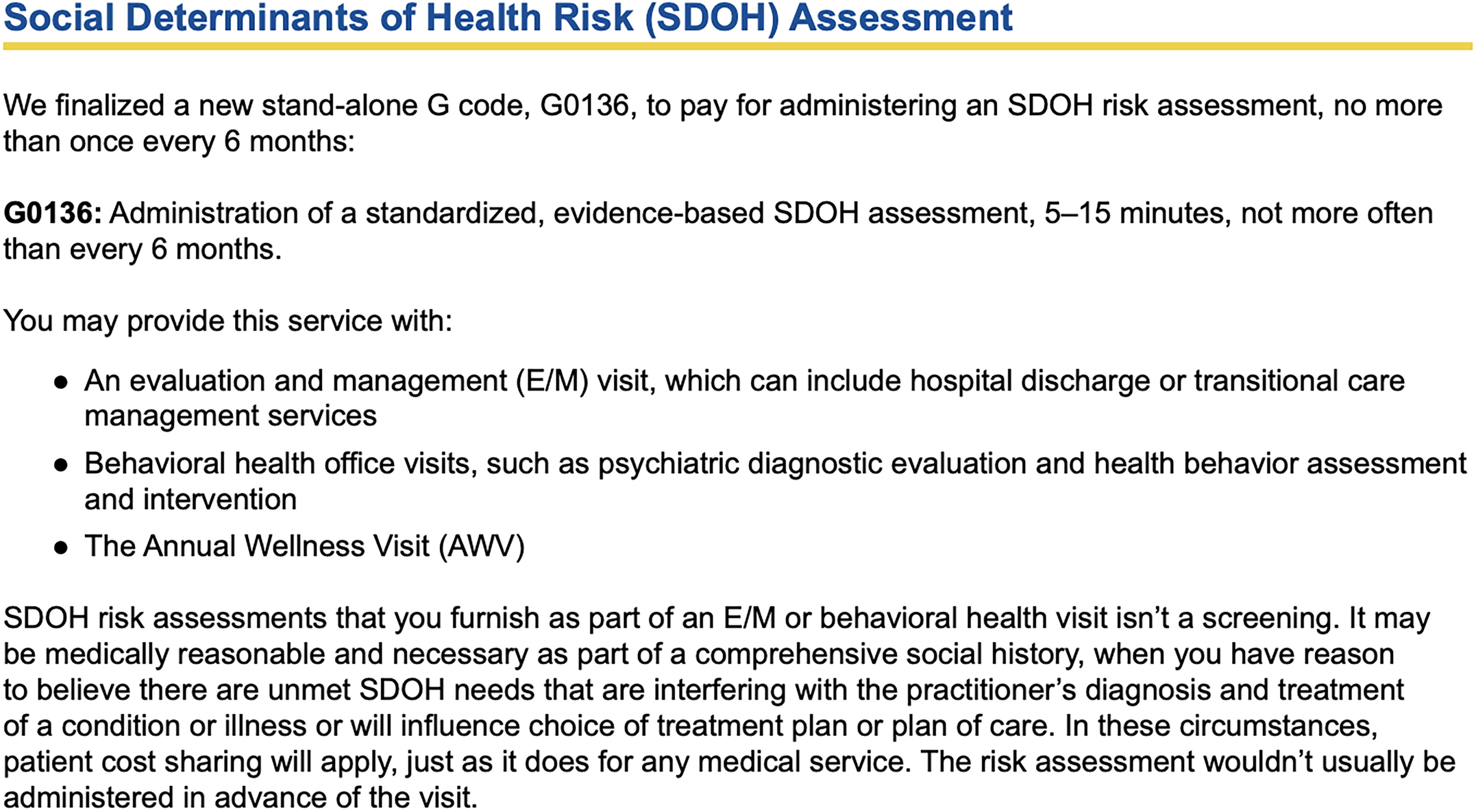
Social Determinants of Health (SDOH) Assessment.
There are several important factors to consider when utilizing this code for health risk assessments. These assessments are not screenings. They can only be completed when providers “have reason to believe there are unmet SDOH needs interfering with…diagnosis and treatment of a condition.” The example CMS provided for utilizing this code details that there must be a clear disruption to care, such as missing appointments due to transportation issues. When this disparity has been identified, an evidenced based tool must be utilized in assessing for the limitations to care due to this disparity. There are already many evidence-backed tools that are available on the CMS website available for use. Further, unlike general screenings that can be administered at every visit, these assessments can only be billed at 6-month intervals.
These services can be conducted during a variety of encounters and over multiple platforms. They can be administered during an evaluation and management visit, as part of a hospital discharge, during behavioral health office visits, or at an annual wellness visit. Most significantly, these assessments can be conducted over a TH platform.
From a health-system and provider standpoint, identifying and tracking the individuals that have clear disruptions to care would require a significant effort for the administrative, personnel, and facility needed to integrate into a present workflow. These patients would need to be flagged and assessed within an acceptable time-frame. A proficient TH infrastructure provides a low overhead pathway to increase the number of patient services provided. TH-based care delivery has been shown to decrease the “unit-cost” of care relating to personnel and equipment costs. 4 These assessments could be conducted apart from a traditional care visit or following a hospital discharge and have their own schedule distinct from the daily patient schedule. These could be completed by a staff member other than the primary provider, such as a dedicated social worker, digital-health/TH specific employee or APP.
From a patient point-of-view, TH services obviate the need to be physically present in a care facility. A TH infrastructure offers several advantages for patients in both rural and urban underserved communities. Patients benefit from reduced costs associated with travel time and time-off from work. 1 A distinct TH-associated schedule would also increase availability. TH services have already been proven to increase health education and promotion among disparate populations. 5,6
A code for the reimbursement for health determinant collection fits within a larger movement focused on the importance of health disparity and care navigation services. Within the “Health Equity Services” portion of the 2024 Physician Fee Schedule are other G-codes associated with Community Health Integration and Principal Illness Navigation. Both of these services provide person-centered planning, health care navigation, and community resource allocation, among others. While some of these services were available to Medicare or Medicaid beneficiaries previously, these designations were state-dependent. Further, including the risk assessment reimbursement provides an incentive to begin the process of addressing complex social needs and is a vital step for progress in this space. Consistent application of this risk assessment and code allows for data to conduct studies on its effectiveness and patient satisfaction to advocate for further compensation and support in this arena.
It is important to note several potential barriers to the success of this initiative. In regard to TH utilization, it is estimated that 50 percent of all visits were performed over Th in April of 2020. This rate quickly dropped to 39 percent by 2021. 7 While current utilization is still higher than the pre-pandemic period, disparate access to TH services limits further utilization. Broadband internet access and devices that can connect to network are not as readily accessible in low-income communities. Promising initiatives such as the Federally funded Broadband Equity, Access, and Deployment program present an opportunity for expanding access to TH services. 8 Other factors include a limited access to suitable spaces necessary for meaningful conversations about sensitive topics. 9 Patient uncertainty for the utility of social needs discussions is a primary limitation to engaging in these conversations during a care-related appointment. 10 Refining the established structure to utilize this new G-code within a TH framework presents an opportunity to create a culture centered on addressing social needs that is distinct from health-care related visits. This represents a promising foundation for increasing patient engagement and further disparity assessment changes in the future.
Footnotes
Author Disclosure Statement
All authors have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received for this article.