
Abstract
Despite focusing on drivers of health, or social determinants of health, for more than a decade, health care organizations have made minimal progress in improving these factors and associated health outcomes. This data- and theory-driven analysis looks at (1) why that is the case and (2) how organizational leaders and operators can go about correcting it. The authors’ research finds that lack of progress is often due to ill-fit, entrenched business models that were optimized for a fee-for-service environment and cannot easily pivot to focus on drivers of health. Additionally, leaders are often unclear about what to change and overwhelmed by how to do it. The authors propose a 5-step strategy and execution process to address these challenges, laying out an end-to-end road map that enables health care leaders to meaningfully improve drivers of health and associated health outcomes for their patients and communities.
Introduction
In this article, the authors outline a guide to success for health care leaders whose organizations have made a commitment to population health, community health, drivers of health (DOH), or social determinants of health (SDOH). The authors appreciate the challenges of addressing social DOH in the current policy and financing environment. However, the Centers for Medicare and Medicaid Services and other payers are increasingly incentivizing DOH-related interventions. As a result, since the passing of the Affordable Care Act, more and more organizations have invested in various strategies and programs to improve health.
Herein, the authors outline evidence-based, practical strategies for leaders who have committed to the cause for improved health, so they can make the required changes for their DOH commitments to succeed.
For more than a decade, health systems, hospitals, community-based organizations, payers, community clinics, and the government have been attempting to improve DOH (a.k.a. SDOH). But overall, little progress has been made in improving these factors that contribute to up to 80% of our health outcomes. 1
What are these DOH? The authors define them as all the circumstances in a person’s life that affect their health and quality of life status. 2 These include access to quality health care, plus nonmedical factors, such as education access and quality, access to and affordability of healthy foods, social connections and support, stable employment and housing, safe neighborhoods, clean air and water, and more.
So, why, if we know these factors contribute so significantly to health outcomes, has the health care system not made more progress? There are two root causes.
First, the prevailing fee-for-service business models in health care delivery are optimized to treat sickness, not promote health or prevention. 3 Because business models are ingrained and resistant to change once established to serve a specific value proposition (ie, treating sickness), today’s organizations lack the foundation to support prevention services and address DOH.
Second, even if they had the right business model, organizational and government leaders may lack a clear pathway for how to change, or a picture of what effective change looks like. The problem is a lack of clarity and direction around what success looks like and how to achieve it.
In this brief, the authors offer a five-step guide to help health care leaders solve the problems of ill-fit business models and an unclear “what” combined with a foggy or overwhelming “how.” To address DOH effectively, health care leaders must (1) articulate their beliefs and vision, (2) understand their business models, (3) improve or transform their models to support DOH interventions, (4) specify their strategies overall and specifically for DOH, and (5) implement effective interventions. To guide them through this process, the authors have developed a road map highlighted in this piece.
Before discussing the solution, a brief overview of Business Model Theory is below, which is critical to understanding the process.
Brief Business Model Theory Overview
What are health care organizations capable of? How much change can they bear? What types of innovations can they successfully deploy? Which ones require a fundamental restructuring of how organizations operate?
The Christensen Institute has a unique theoretical framework that answers these questions and clarifies the often nebulous concept of a “business model.” (See Fig. 1.) The framework defines a business model as four interlocking elements that, when taken together, create and deliver value: value proposition, resources, processes, and profit formula/priorities.

The 4 components of a health care business model. This graphic was originally published in Clayton M. Christensen and Mark W. Johnson, “What Are Business Models, and How Are They Built?” Harvard Business School Module Note, August 2009 (revised November 2021). It has been modified to focus on health care business models.
Business models determine an organization’s or company’s capabilities (what it can and cannot do) and its priorities (what it must accomplish). This, in turn, defines which innovations it can and will pursue. The framework is powerful because it enables the prediction of which initiatives will succeed and which ones will fail. It is critical for leaders to understand these four components of their business model so they know what to leverage from their core business when they need to employ a new business model approach.
In an organization’s early days, when it is operating as a startup, all business model components are flexible. To survive infancy, organizations pivot their value propositions and adjust their resources and processes until they identify how to bring in the revenue they need to survive. Once this is determined, business model components become increasingly interdependent and resistant to change, especially in successful organizations.
This happens because when resources and processes meet a need or solve a problem, they get replicated, repeated, improved, and standardized. Even though specific value propositions were an organization’s starting point, a mature organization can only successfully deliver value propositions that fit its existing resources, processes, and profit formula. As a result, all four components become interdependent, creating a durable set of capabilities and priorities.
Therefore, if leaders of established organizations want to pursue an innovation that conflicts with their existing capabilities and priorities, they must create a new business unit with a new business model approach. This was the approach taken by Intermountain with the creation of CivicaRx, by Providence with the creation of Ayin, and by Advocate Aurora Health with Advocate Aurora Enterprises. In-depth case studies on these examples can be found in Hogg’s study. 4 This was also the approach taken by Dayton department stores when they created an autonomous business unit known as Target, which grew over time and ultimately became the dominant business model. This evolution occurred over decades. 5
A 5-Step Guide to Help Health Care Leaders Make Progress on DOH
Step 1: Setting the stage: Articulate beliefs about the future, mission, and vision
Despite the stubborn challenges facing those who attempt to change entrenched business models, with the right tools and approach, it is still possible to succeed. To do so, leaders must first understand the specific context in which their model exists both today and in the future. This process starts with setting the stage to articulate beliefs about the future, mission, and vision.
Outlining beliefs about the future, as well as the company’s purpose (mission) and where it sees itself going (vision), is a foundational aspect of a strategy. To formulate beliefs, leaders should perform a thorough scan of current and emerging market trends, consumer behaviors, competitor dynamics, and futurist predictions. Armed with these inputs, leaders can then articulate three to five beliefs about the future that will inform what they need to do now in order to succeed in the future they see on the horizon. An example of a belief about the future could be that health care payers and providers, motivated in part by growing regulatory and accreditation pressures, will need to address DOH beyond medical care.
Leaders should also affirm that the existing mission and vision are still the company’s purpose and desired destination. If this is not the case, leaders must revise these grounding principles. Given leaders’ awareness of the evolving landscape and the desire to enable their organizations to effectively address DOH, one or both of these foundational components may well need to change.
Because strategy operationalizes a vision and articulates how to arrive at the desired destination, leaders cannot establish a clear and compelling strategy without first solidifying the vision. In other words, strategy without vision is much like a set of directions without a specified destination. A variety of resources exist to help leaders in the process of defining their vision. Two compelling ones are Innosight’s “future-back” process 6 and A.G. Lafley and Roger Martin’s “playing to win” framework. 7
Step 2: Understanding the current and future state: Map the business model and determine its viability
Armed with beliefs about the future and a clarified mission and vision, leaders should map their current business model. There are many methodologies available to do this, but the most straightforward is the four-box framework shared earlier. Mapping includes articulating today’s model: the value proposition(s) the organization offers customers, the resources and processes required to deliver those promises, and the revenue and cost structures that allow the entity to do so sustainably.
It also includes stating what the future business model needs to entail. In this step, leaders will want to articulate their future value proposition that takes DOH into account; they will also need to state what business model components are required to deliver this new value proposition and how revenues and/or expenses will need to change in order to do so sustainably. Lastly, they will need to determine how they will adjust priorities to align with their new approach.
Outputs from this step include answers to the following questions: What existing capabilities can we leverage? Which additional/different ones are required for the future, and how do we support DOH work? How and to what extent will our revenue streams be impacted in the future? How and to what extent will costs be influenced?
Understanding the vision for DOH impact, the scope of services that will be provided, and what existing business model components can support change will be key considerations as leaders move to step 3.
Step 3: Determining the strategy for change while accounting for risk
When leaders need a strategy to operationalize a required business model change, they have a choice of two approaches: They can improve their existing model or transform their business by creating a new business model within a separate business unit. The challenge is in choosing the appropriate approach and accepting the risks associated with each option.
In short, when today’s value proposition is similar to the proposed future value proposition, an improvement strategy is usually appropriate. However, leaders should remember that an improvement approach will not work if the new value proposition is too different from the current one or if the profit formula has to change.
In cases where the value proposition of the core business is different from that of a potential new opportunity (ie, serving DOH needs when one has not previously done so), the current business model’s viability is limited or already in decline, and/or a new profit formula is required, leaders must pursue a transformation strategy. This is typically done through either a buy, build, or partner approach.
Determining the value proposition for a DOH program is similar to any other: How can an organization effectively meet an unmet need by drawing on existing and potentially new capabilities? 8 For DOH programs, an additional consideration is the availability and interest of social service organizations that could help meet those needs through contractual or referral arrangements.
The authors created a decision tool to help leaders determine which business model strategy is right for their future. This guide takes into account the context considerations detailed above and the risk considerations outlined in more detail in the study by Hogg. 4 It is based on the tenets of Business Model Theory and what has—and has not—worked for leading innovators in the field. See Figure 2 for the tool.
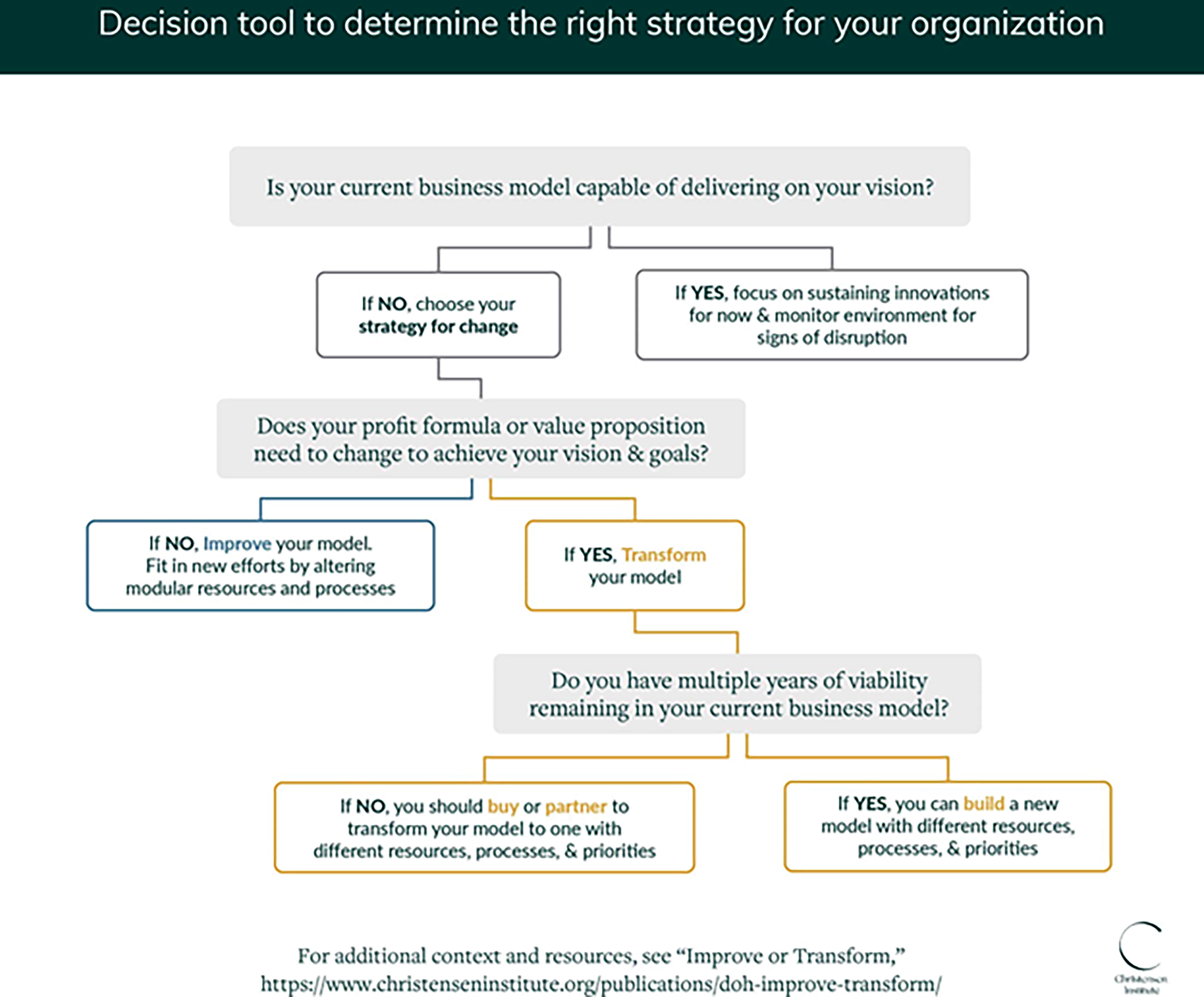
Decision tool to determine the right strategy for your organization.
One output of this step is a clear plan to improve the existing business model or transform it by creating a new business model in a separate unit.
With an updated vision, mission, and value proposition that includes addressing DOH and a strategy to improve or transform the business model to deliver DOH programs effectively, the next step is to design and build the DOH programs.
Step 4: Designing and delivering DOH programs
Once organizational leaders have articulated the high-level direction for the organization, including mission, vision, and beliefs about the future; determined the business model requirements to deliver on the mission and achieve the vision; and assessed the appropriate organizational strategy to pursue, they can tackle the operational details of DOH strategy and program development.
Effective DOH initiatives operate in the zone of convergence (see arrow in Fig. 3), where they can meet the needs of the organization’s targeted populations by drawing on a realistic set of internal capabilities as well as external community and government resources.

Zone of convergence for DOH initiatives. DOH, drivers of health.
For example, an initiative could aim to help patients living in a “food desert” with uncontrolled diabetes and food insecurity improve their HbA1c or reduce food insecurity by developing partnerships with local Meals on Wheels programs and food pantries or by introducing a new grocery delivery service.
Critical strategy and design questions to tackle operational details of DOH strategy and program development include: What are our DOH-specific goals? How do these align with the organization’s overall priorities, and how do they support the profit formula? What programs will help us achieve those goals? What are the DOH programs’ goals? How will success be measured? Based on the organizational strategy of “Improve or Transform,” where will these initiatives live in the organization, and who is responsible for the outcomes? Based on the value proposition, what services or goods must we deliver and to whom? How can we test and refine the value to stakeholders, including all the intended participants? What internal capabilities (resources/processes) do we leverage or augment, and what external capabilities do we need? How do we include them in our business model? Do we create contractual agreements, referral arrangements, or other relationships? What will the intervention cost, how will we fund it (profit formula), and how do we align the intervention’s success with the organization’s broader goals (priorities)? How can we build a strong pathway (process) to results?
Step 5: Building the pathway to results
A key value of DOH programs is to help people with social risks obtain and use resources that meet their health-related social needs. For example, people who struggle with food insecurity need to get food they and their families will eat when they need it. Unfortunately, in many cases, most of the participants in DOH programs do not get the resources they need. 9 Not only does this reduce the program’s effectiveness, but it is also frustrating for patients, clinicians, and others who are trying to resolve social risks.
By definition, DOH programs cross medical and social care sectors and organizations. Health care organizations typically refer patients to social resources, such as community-based organizations and government programs. To “close the loop” or get resources to patients, the activities of health care and social service organizations must be aligned with each other—and they must also be aligned with patients’ journeys.
While this sounds self-evident, some programs simply provide information about social resources and hope for the best. There is, however, a useful 4-step model to understand and address the gaps and opportunities along these pathways. The 4 steps are as follows, and they are explained in detail below: Understand the ecosystem and involve stakeholders in design Map the pathways to results and connection points Identify connection drivers and mitigate risks Measure and improve
To most effectively understand where gaps may arise, leaders should develop their pathways model through the lens of their future business model. This will highlight potential pitfalls or areas where organizational capabilities (ie, resources and processes) and priorities are mismatched to achieve desired outcomes in advance of program roll-out.
The ideal way to identify the key stakeholders, draw the pathways map, assess the risk of weak connection points, and proactively mitigate those risks is to involve the stakeholders at every step. While potentially time-consuming, it is essential. Unfortunately, many programs only ask stakeholders to share their perspectives after the fact, when most of the people for whom the program was designed fail to get any benefit from it. 10
The process in detail
Understand the ecosystem; identify and involve stakeholders in design
A DOH program ecosystem encompasses the sponsoring health care organization and one or more community-based organizations that provide health-related social resources like food or housing assistance. Stakeholders include multiple people within those organizations. For example, stakeholders in a DOH program to address food insecurity are likely to include: Primary care clinicians and medical assistants—to identify people who might benefit from the program and refer them to social resources; DOH program staff (eg, community health workers to help people find and access food or food assistance, nutritionists, diabetes educators); Managers, frontline staff, and others in community-based organizations that provide food and assistance in accessing food assistance programs such as the Supplemental Nutrition Assistance Program (SNAP) and the Women, Infants, and Childrens Nutrition Program (WIC); The patients themselves.
Map the pathway to results and connection points
Once the stakeholders are identified, a “pathways” map should be developed. This map, which is like an expanded journey map, identifies the steps along the pathway, within and across organizations, that patients must traverse to get resources. But listing the steps is only the beginning. The critical exercise to ensure that the pathway is strong involves two additional analyses: identifying the connection points from each step to the next and assessing where barriers may arise to prevent those connections.
It is also critical to understand where the DOH strategy and associated programs fit within the organizational strategy and priorities, as well as the organizational resources that will be available for the work, the processes that may support or hinder its roll-out, and alignment with overall organizational priorities.
Identify connection drivers and mitigate risks
Barriers, or missed connections along the pathway, can occur anywhere. Drawing on other programs’ lessons learned reveals a range of barriers and root causes, some of which may not be obvious at first glance. Some examples are as follows: Health care organizations hesitate to screen people for problems they cannot solve, such as access to affordable housing. Patients who do not trust the people who are screening them may fear that disclosing problems like food insecurity will expose them to consequences like losing custody of their children. Not all patients with social risks want help or the help offered by a health care organization. Social resource organizations with limited capacity or cultural fit may be unable to serve patients referred to them. Social resource organizations may be inaccessible to people who do not have cars, cannot come when they are open, or have limited English language or digital access.
Barriers may also occur at particularly stressful or critical connection points, like handoffs from one organization to another or areas in which people are being asked to make significant behavior changes.
Once critical risks are identified, some can be mitigated. For example, the hours or food selection at a food bank could be changed to better meet participants’ needs, but SNAP eligibility and application processes cannot. This process will create a stronger pathway by which more patients get social resources to improve their health.
Pulling it all together, an output of this pathways process is a visual map of the major stakeholders and steps along the pathways to get resources (see Fig. 4). It highlights the connection points and risks of barriers that leaders should pay attention to as the program is implemented and succinctly communicates the complex interactions of people, organizations, and resources required for the DOH program to be successful.

DOH pathways map. Health care organization step/connection driver.  Social resource step/connection driver.
Social resource step/connection driver.  Participant resource step/connection driver.
Participant resource step/connection driver.
Measure and improve
Like any new program, DOH programs—particularly those that involve new business models, new intervention strategies, and new partners—will not get everything right from the beginning. Successful DOH programs routinely test and learn or use the principles of continuous quality improvement to assess what is working well and what needs improvement. Two elements of the pathways framework are critical to optimizing improvement: understanding breakdowns at the key connection points along the pathway and getting (and using) input from stakeholders. While it is more work to collect data, examine processes, workflows, and relationships step by step, and to build relationships with stakeholders to get meaningful insights about barriers and facilitators, the results are worth it.
Conclusion
The DOH are responsible for the vast majority of our health outcomes. But today’s health care business models are not set up to address or positively influence them. One root cause of this issue is the traditional fee-for-service business model. Additionally, leaders operating in that business model do not have clarity on what needs to change, or how to do it, in order to effectively impact DOH and improve overall health.
However, by following a clear, five-step process with associated frameworks and strategy and program development tools, leaders can not only determine what to change but also how to do it.
The work is not easy, but these tools will help leaders traverse the foggy unknown of business model change and systematic program design to amplify their DOH impact. May this guide empower you to get started, or correct course, on your DOH journey.
Footnotes
Authors’ Contributions
A.S.H.: Conceptualization (lead), writing—original draft (equal), writing—review and editing (lead), visualization (equal), and formal analysis (equal). A.S.: Conceptualization (supporting), writing—original draft (equal), writing—review and editing (supporting), visualization (equal), and formal analysis (equal).
Author Disclosure Statement
The authors declare that they have no relevant or material financial interests that relate to the research described in this article.
Funding Information
No funding was received for this article.