
Abstract
In response to rising costs associated with providing health care services to Americans over 65 years old, policymakers have called for the expansion of care coordination programs to reduce total spending while improving patient outcomes and provider efficiency. This study uses a Markov Chain model to estimate financial impacts associated with the implementation of a care coordination program across the state of Iowa. Estimates revealed an association between the implementation of the Iowa Return to Community (IRTC) and a reduction in health care service use, which yielded per capita cost savings of $7,920.24 over a 5-year span. Subgroup analysis showed that inclusion of informal care partners enhances these savings, as they contributed to reduced inpatient hospital use and deferred nursing home admissions. The continued expansion of the IRTC appears as a viable strategy to curtail aggregate health care spending while supporting older adults stay at home.
Introduction
U.S. Census projects the total number of Americans over the age of 65 to soon outnumber those under the age of 18 for the first time in history, and the costs associated with providing health care services to older Americans are substantial. 1,2 In 2021 alone, 1 out of every 5 older Medicare patients experienced an inpatient admission with an average stay of 5.6 days, constituting 26% of total national health spending on medical care. 3 While some researchers indicate that hospitalization rates for older adults continue to trend upward, 4 others have suggested that 12.9% of all hospital admissions can be attributed to health conditions that can be managed and treated in ambulatory care settings. 5 Charges for these types of inpatient visits were nearly 4 times higher than a standard inpatient admission ($11,414 vs. $2,563). 6
Furthermore, some older adults, especially those who lack access to home and community-based services (HCBS) and long-term support services (LTSS), show an increased likelihood of placement in nursing homes despite needing little medical or physical assistance. 7,8 The annual costs associated with these low-acuity nursing home placements amount to nearly $10.6 billion. 9 This potentially avoidable financing of LTSS for older Americans is particularly an issue for state Medicaid programs, as older adults who are near-poor and medically at-risk are more inclined to become qualified beneficiaries. 10,11
To reduce overall health care spending, policymakers advocate for the expansion of patient-centered care coordination programs, in which interprofessional teams, including clinicians, rehabilitation specialists, and administrative professionals, provide information and education to older adults and connect them with supportive services that enable independent living in community settings. 12,13 Previous studies have demonstrated how implementation of such programs was linked to a decrease in hospital admissions and nursing home stays among older adults. 13,14 In addition to engaging interprofessional teams, some programs emphasize the importance of involving home-based informal care partners (ICPs) in discharge planning and care coordination processes. 15 Research has shown that older adults with ICPs are less likely to require nursing home stays. 16,17
While offering supportive services to older adults and their ICPs has been associated with reductions in health care use and improved patient outcomes, 13,18 these studies have yet to estimate how such programs impact aggregate spending over time. The goal of this study is to address this gap by estimating financial benefits associated with the implementation of the Iowa Return to Community (IRTC) program over a 5-year time span. This evidence-informed care coordination initiative relies on interprofessional teams and ICPs to assist older adults at-risk for hospital use and nursing home admission in Iowa to live independently in community settings.
Iowa return to community program
The IRTC was introduced in 2019 by the Iowa Department on Aging (IDA—which recently merged into the Iowa Department of Health and Human Services (HHS), becoming the Iowa HHS Division of Aging and Disability Services), in 4 of the 6 Areas Agencies on Aging (AAA). This program leverages partnerships between hospitals, community-based medical clinics, nursing homes, and AAAs to identify at-risk older adults and support their transitions from nursing homes and hospital settings to community living. Individuals were considered at-risk based on the following criteria: being near-poor (measured by annual income between 138.0% and 300.0% of the Federal Poverty Line—FPL), non-Medicaid, aged 60 or older, and at-risk for functional decline due to demographic, socioeconomic, or medical/health-related reasons. 19 Once identified by local hospital discharge planners, medical clinic case workers, and nursing home staff, these at-risk individuals would then be referred to AAA-based care coordinators who would conduct a comprehensive assessment of individual needs and preferences as well as develop and implement customized care plans. These plans included the provision of social support services, such as home-delivered meals, transportation, and home modifications, for up to 90 days, regardless of the older adults’ ability to pay, as supported by the federal Older Americans Act and state appropriations. 20 Beyond its primary focus on aiding at-risk older adults, the program recognizes and responds to the interconnected nature of caregiving by extending similar supportive services to ICPs. 17
Reductions in nursing home placement and hospital use were repeatedly observed among IRTC enrollees since the program’s initial implementation. 19 The Iowa HHS Division on Aging and Disability Services reported that nearly 90% of program participants transitioned back to the community from a hospital stay or nursing home placement within 90 days, 19 and previous studies attribute this success primarily to the consistent use of support services over the enrollment period. 20 Given the high rates of community transitions associated with the implementation of IRTC, the goal is to explore whether these results would remain consistent over a 5-year period and if such transitions lead to cost savings.
New contribution
In addition to expanding the understanding of how care coordination helps older adults remain at home, economic modeling is used to forecast aggregate spending associated with the implementation of such programs. Existing literature examines transitions of older adults primarily between 2 settings (e.g., hospital to community, hospital to nursing homes and vice versa). 21 –23 This approach, while beneficial for understanding specific aspects of transitions and evaluating the effects of care coordination under controlled conditions, might not fully capture the complex nature of real-world settings, where older adults could experience multiple transitions over time across more than 2 settings. Therefore, this study includes the estimation of probabilities for individuals moving between hospitals, nursing homes, and community settings, and then, the incorporation of these parameters into a Markov Chain model to provide a more comprehensive picture of older adult transition dynamics. This study also contributes to the literature on ICPs by examining the potential impact of supporting their involvement in care coordination processes for at-risk older adults on hospital utilization outcomes, nursing home admission rates, and aggregate expenditures over time.
Methodology
Data sources
Data were obtained from Iowa HHS and consisted of a de-identified sample of 523 enrolled individuals who were referred to IRTC between July 1st, 2020 and June 30th, 2022 by hospital and nursing home staff or persons who independently reached out to IRTC program coordinators. The dataset included individual information on demographics, referral source, social support services received, as well as program discharge outcomes. To compare IRTC projections with what would happen without IRTC in place, data from a statistically matched control group derived from the National Health and Aging Study (NHATS) for the years 2020–2021 was used. The NHATS population is a nationally representative sample of Medicare recipients providing detailed information on participants demographics, activities of daily living, functional limitations, as well as other social and physical characteristics. 24
The statistical matching was based on several basic demographic characteristics, including race, ethnicity, gender, living alone, and income level. In addition, 2 additive indices for instrumental activities of daily living (IADL) and activities of daily living (ADL) were used. Both indices were constructed by summing daily activity variables, which were categorical with values ranging from 0 to 3: 0 indicating the activity did not occur, 1 indicating no help was needed, 2 indicating help was sometimes needed, and 3 indicating help was always needed. The sum was then divided by the total number of variables. The IADL index included 6 activity variables: shopping, taking medications, cooking meals, using transportation, managing money, and doing light chores. The ADL index also included 6 activity variables: walking, bathing, dressing, transferring, toileting, and eating.
Data analysis
To estimate spending associated with the IRTC program, a Markov Chain model was conducted, which simulated transitions of participants between hospitals, nursing homes, and community-based settings as well as the associated costs over a 5-year period. Markov Chains belong to a group of economic models capable of simulating events with recursive components over time. 25,26 Their basic property is that there is a finite number of states of health referred to as “health states” at any given time, and all events of interest are modeled as transitions from one state to another. 26 Time is divided into a sequence of discrete periods (e.g., 1 day, 1 month, 1 year), and the model simulates the number of observations that have transitioned between states and their associated costs or utilities at the end of each period. 27 In this study, each discrete period represented 1 year, with simulations conducted over a total of 5 years. The 5-year period was chosen to align with the typical timeframe used in economic models for strategic planning. 28
All models were run for cohorts of 10,000 individuals using Monte Carlo simulations, where multiple sampling with replacement was done from both the IRTC group and the matched control to account for possible uncertainties in the transition probabilities. Costs were discounted to their present value using an annual discounting rate of 3.5% in line with standard guidelines and practices for economic evaluations. 29 Furthermore, deterministic sensitivity analyses were conducted by adjusting individual parameters upwards and downwards by 20%, 30%, and 40% to construct best- and worst-case scenarios, assessing the models’ sensitivity. Best-case scenarios assumed increased rates of transitions back to community and lower rates of hospitalization, nursing home admissions, and death, whereas the worst-case scenarios assumed lower community transitions and higher rates of adverse health outcomes.
In addition, an a priori power calculation (α = 0.05, β = 0.80) indicated that a minimum sample size of 200 was required to detect a 30% difference in community transition proportions between IRTC enrollees and the control group, as reported in prior studies. 21 –23 A post hoc power analysis was deemed unnecessary, as the population projections for transitions between health states and their associated costs were based on simulated samples of 10,000 individuals per group and subgroup, 50 times larger than the minimum sample size needed to detect the anticipated effect size. The Markov Chain analysis with Monte Carlo simulations was performed using SpiceLogic Markov Decision Process 4.1.3, a statistical software package designed for health economic modeling. Statistical matching, calculation of transition probabilities, average costs, and statistical power were conducted in STATA 18.0.
The constructed Markov Chain tracked IRTC enrollees under 2 scenarios: first, by comparing IRTC transitions with those from a statistically matched control group from NHATS data, and second, by separating IRTC participants with ICPs and comparing their transitions to those without ICPs. In this study, ICP support was determined based on IRTC enrollee assessment responses on whether they were receiving help from their spouse, a family member, a friend, or another caregiver. 19 All ICPs supporting IRTC enrollees received assistance from the IRTC program, whether through counseling or direct supportive services like home-delivered meals and transportation assistance.
Health states
A total of 4 health states were identified in which individuals are referred from and discharged to: (a) living in the community, (b) experiencing a hospitalization, (c) getting admitted to a nursing home, and (d) deceased. As with other studies that use Markov Chains to explore state progression, deceased signifies an absorbing state, meaning that individuals are only transitioning to and not from. 27 Based on annual probabilities of transition from one health state to another, the model forecasted and monitored from 2023 to 2027 the number of enrollees who remained in the community and their related costs of care, the number who experienced a hospitalization or residential placement accruing facility charges, and those who passed away.
Transition probabilities
The annual likelihood of transitioning between defined health states was estimated based on observed transitions in the IRTC data and the statistically matched group from NHATS data. These transitions represented the possible pathways of older adults moving between hospitals, nursing homes, and community-based settings and passing away. For the IRTC group, individuals were first categorized based on their referral sources: hospital discharge planners, health professionals in nursing homes, and clinics or other community-based settings. Then, the likelihood of transitioning to community-based settings, hospitals, nursing homes, or passing away was estimated separately for each category. This was done by dividing the number of individuals transitioning from one initial state to another by the total number of individuals in the initial state. For instance, the transition probability for individuals moving from a hospital setting to community living was calculated by dividing the number of those discharged from the IRTC program to the community by the total number referred to the program from hospitals. The same approach was used to estimate transition probabilities for IRTC participants with and without ICPs.
For the statistically matched group from NHATS data, individuals were separated based on their 2020 setting: living in the community, admitted to a nursing home, or those who experienced hospitalization. Then, the number of individuals from each category who, by the end of 2021, were residing in community settings, nursing homes, hospitals, or were deceased was tracked. Transition probabilities were estimated using the same approach as for the IRTC cohort and its subgroups. All estimated probabilities were normalized to sum to one for each initial health state by calculating the total of the original percentages and then dividing each original percentage by this total. Table 1 Figure1.
Transition Probabilities of the Markov Chain Model
ICP—Informal Care Partners. IRTC, Iowa Return to Community.

Markov Chain diagram showing transition pathways between community, hospital, and deceased.
Costs
The cost for IRTC participants living in community-based settings was estimated by analyzing their use of services such as options counseling, direct support services, home visits, and case management, as well as the associated administrative overhead costs during program enrollment. To determine the average cost per person, the total cost was then divided by the total number of IRTC participants. This average cost was assigned to the “living in community” health state exclusively for the IRTC group, as the matched control group would not have received supportive services from the IRTC program. In the subgroup analysis, it was observed that individuals with ICPs incurred slightly higher costs, as their ICPs also received supportive services from IRTC. This difference was accounted for in the Markov Chains for this subgroup.
For the “hospital” health state, data from the health care cost and utilization project (HCUP) was used, which provided a range of costs for various types of hospitalizations. 4,30 The cost reflected in the model was estimated by multiplying the cost of one stay by the average number of days a Medicare patient spends in the hospital annually. For the “nursing home” health state, data from the Brown University Center for Gerontology and Health Care Research LTCfocus dataset was used, which provided information for nursing homes, including spending. 9 The average cost assigned to the “nursing home” health state was derived by multiplying the daily cost by 90, corresponding to a conservative estimate of the median number of days an older adult typically spends in a nursing home annually for short-term stays. 31 To maintain consistency in comparisons, the average cost of experiencing a hospitalization and that of nursing home placement were assumed to be the same for both the IRTC group and the matched control, as well as for both subgroups (those with ICP and those without). Lastly, the costs of being deceased were not considered in this analysis. Table 2.
Cost Parameters of the Markov Model
The percentages represent the proportion of the total direct cost allocated to IRTC enrollees for options counseling, direct support services, home visits and case management, as well as overhead administrative expenses.
ICP—informal care partners.
Results
Descriptive statistics for the statistically matched control group, the IRTC group, and the IRTC enrollees with and without ICPs are presented in Table 3. The matching process resulted in a total of 974 individuals from the NHATS data with characteristics similar to those of the IRTC group. Overall, the majority of the matched control group and the IRTC enrollees were white, non-Hispanic females, living above 100% of the FPL and living alone. The IRTC enrollees had slightly higher needs for ADLs and IADLs, as indicated by the average values of both indices. When comparing the two subgroups, differences in living arrangements were observed: 70% of those without ICPs lived alone, compared with only 48% of those with ICPs. Both ADL and IADL needs were higher for the group of IRTC enrollees with ICPs. Table 3
Descriptive Statistics
ICP—informal care partners. ADL, activities of daily living; IADL, instrumental activities of daily living; IRTC, Iowa Return to Community.
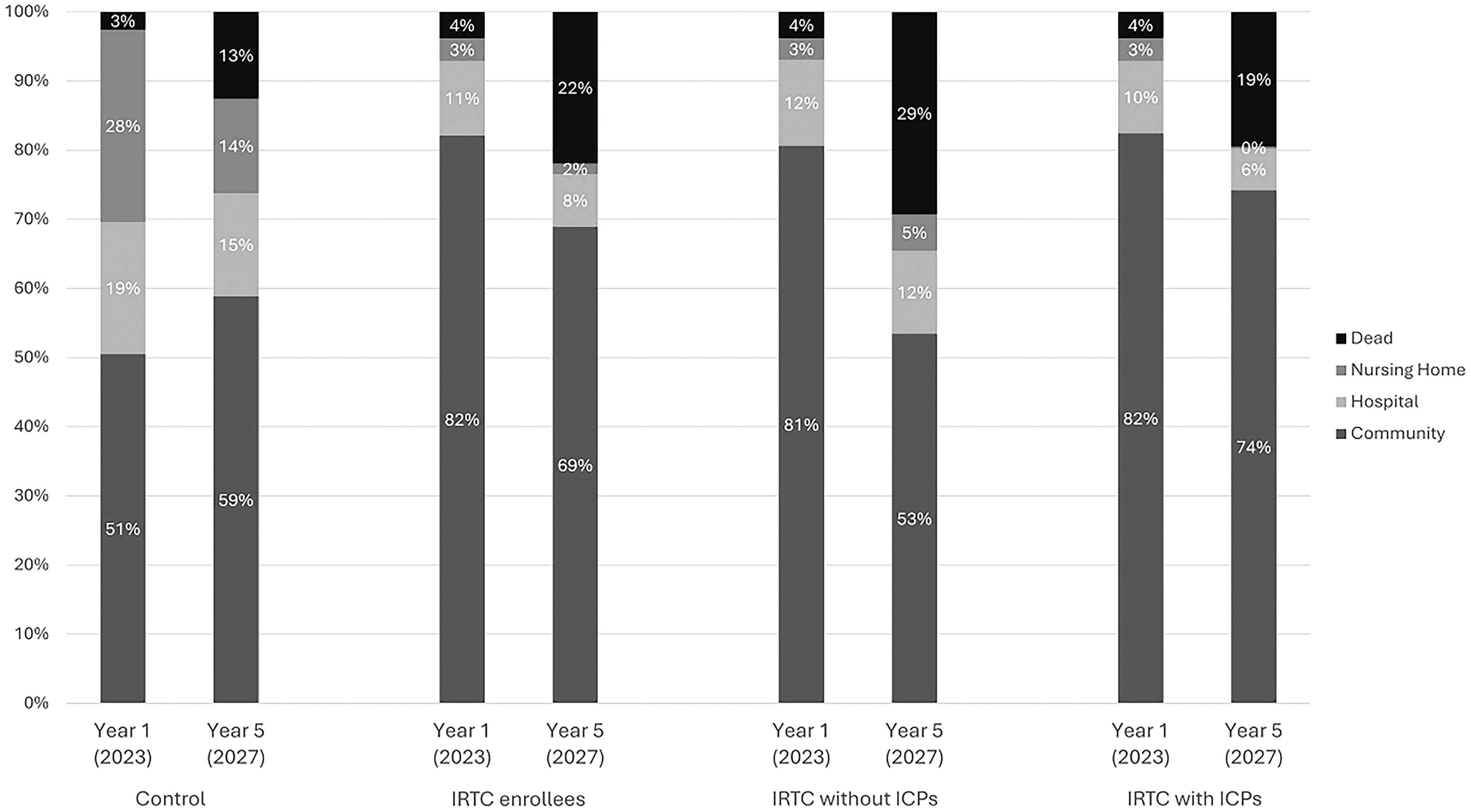
Upon executing the Markov Chain model, unique patterns emerged across the 4 defined health states ([a] living in the community, [b] experiencing a hospitalization, [c] getting admitted to a nursing home, and [d] deceased). Figure 2 shows the proportion of the population across the 4 defined health states for the simulated cohorts for selected years of projection. In the first analysis, comparing IRTC enrollee transitions with those of the statistically matched control, the model predicted that 69% of IRTC enrollees would be living in the community at year 5, as opposed to only 59% without IRTC in place. Regarding hospitalizations, the models suggested that at year 5, the proportion of older adults expected to be hospitalized is slightly lower for the scenario with IRTC, 8% compared with 15% without the program in place.
Population projections for simulated cohorts at select years.
When estimating transition probabilities for IRTC enrollees, the findings indicated a minimal likelihood for IRTC participants to be admitted to a nursing home subsequent to their enrollment in the program. Therefore, over the course of 5 years, with the IRTC in place, a lower proportion of older adults (2%) would be admitted to a nursing home compared to a scenario without the IRTC (nearing 14% by the fifth year). In regard to mortality rates, IRTC enrollees are projected to experience a 22% mortality rate by year 5, while projections exhibit a smaller mortality rate for those without IRTC. Figure 2
Moreover, this analysis forecasted differences in subgroups by contrasting IRTC participants with ICPs against those without. Over the course of 5 years, the group without ICPs is projected to see a 28% decline in the number of individuals residing in the community, from 81% to 53%, while the group with ICPs sees a relatively smaller decline of only 8%. Another difference is shown in hospitalization projections, where, by the fifth year, the cohort with ICPs is anticipated to experience a 4% reduction in hospitalizations while that without ICPs is anticipated to remain constant, at 12%. Mortality rates are projected to increase for both groups over the course of 5 years, reaching 19% for those with ICPs and 29% for IRTC enrollees without ICPs.
The data also reveal that the implementation of this program is associated with reduced financial burdens when contrasted with scenarios where the program is absent. Even after separating the data into subgroups, with one having ICPs and the other not, it is evident that both subgroups within IRTC maintain a cost advantage over the non-IRTC alternative. However, the subgroup without ICP incurs higher costs over time compared with its counterpart that benefits from ICP involvement. Although the cost per enrollee with an ICP is slightly higher than for those without an ICP (refer to Table 2), due to the support services provided to ICPs through the program, these results suggest that their involvement in care coordination for older adults could be beneficial in reducing long-term costs.
Cumulative cost savings associated with the IRTC program are presented in Table 4. Over the course of 5 years, cost savings of $7,920.24 per person would be achieved with the IRTC in place. As depicted in Figure 2, most of these cost savings are achieved through delaying nursing home admission and preventing hospitalizations. The subgroup analysis indicated that savings would be the highest among the individuals with ICPs, achieving cumulative cost savings of $8,330.28 over the course of 5 years as opposed to cumulative cost savings of $6,945.14 among those without ICPs. Initially, in year 1, the savings are modest across all scenarios. By year 5, there is an increase in savings across all scenarios, with IRTC individuals with ICPs achieving higher savings than those without. Best- and worst-case columns provide a risk assessment and offer a spectrum of potential financial outcomes. Best-case scenarios, which assume higher rates of transitions back to community and lower rates of hospitalizations and nursing home admissions, are consistently showing an optimistic upward trend in cost savings. In contrary, the worst-case scenarios present more conservative figures, where higher rates of hospitalizations and nursing home admissions coupled with lower rates of transitions back to the community are leading to diminished cost saving. Table 4.
Cumulative Cost Savings per Capita Achieved by Year and Best-Case Worst-Case Scenarios
Cost savings are presented in discounted 2020 dollars and reflect the difference between the costs incurred by the control group and those incurred by IRTC enrollees, broken down by subgroups.
ICP—informal care partners. IRTC, Iowa Return to Community.
Discussion
This study suggested that the implementation of a patient-centered care coordination program linking older adults to essential community-based social support services is associated with cumulative cost savings. More specifically, over a 5-year span, a potential average savings of $7,920.24 per individual was observed, most of which stems from the decreased cumulative costs associated with extended nursing home care. These estimates also follow on other research suggesting that the financial benefits of care coordination programs can be substantial, yielding high savings per participant. 32 Indeed, expanding implementation of patient-centered care coordination programs may play an important role in reducing aggregate expenditures while also helping older adults remain at home in community settings.
Estimations of the IRTC program costs related to offering support services to an at-risk older adult individual were lower compared with an average hospital or nursing home stay. This finding is consistent with other research that compared costs between support services and institutional care. For instance, one such study highlighted that older adults residing in nursing facilities incurred, on average, $2,919 more in total health expenditures than those with similar acuities and needs who received supportive services in their homes. 33 Upon considering how an estimated 69% of older individuals would still be residing in community settings by the fifth year, as opposed to residing in a nursing home, the merits of such a care coordination model are promising.
Findings also indicated that supporting the involvement of ICPs in assisting older adults can lead to cumulative cost savings over time, and it could be an important element in enhancing older adults’ overall health and well-being. Projections indicated that these cost savings were tied to reductions in hospitalization rates for at-risk older adults with ICPs. This is also consistent with other studies that emphasize the role of ICPs in the lives of older adults, with an effect on minimizing the chances of hospitalizations through the effective management of chronic conditions, 34 the proactive identification and management of potential health issues, 35 and the prevention of accidents or injuries within the home setting. 36 Other studies have found that initiatives designed to support ICPs not only enhance their well-being but also positively affect the care recipients. 17 It stands to reason, then, fostering a supportive environment that caters to the needs of both caregivers and older adults could be instrumental in reducing hospitalizations among older adults.
Given the continued increase in the number of older Americans and the associated costs of providing health care services to this population, it seems prudent to expand care coordination efforts by offering community-based support services to at-risk older persons and then extending similar supports to ICPs who can help reduce hospital and nursing home admissions for at-risk older adults. This expanded approach can offer multiple benefits, where on one hand, ICPs assist older adults in residing in their preferred environment, 15 and on the other hand, this arrangement translates to economic benefits as suggested by these findings. Although the findings from this study may apply to other care coordination programs designed to help older adults live independently in community settings, such initiatives are particularly well-suited for population-based health systems and health care networks capable of engaging and implementing value-based care models. 37
Limitations
Despite the consistency of these findings with previous studies, the results should be interpreted within certain limitations. First, the IRTC data lacked a control group, so this study relied on a statistically matched group drawn from an external dataset that represented a population similar to the IRTC enrollees. While the matching process accounted for various demographic characteristics and up to 12 ADLs and IADLs, unaccounted differences between the IRTC enrollees and the matched control group may have influenced the outcomes. For instance, the matching process could not account for common comorbidities, as AAAs do not receive detailed health information from hospitals and nursing homes at the point of referral but rely on surveys that focus on assessing functional status and identifying support service needs. Moreover, it is likely that the experiences of health care professionals in identifying individuals at risk for hospitalizations or nursing home admissions might have also contributed to these results. Qualitative research, such as interviews with care coordinators and health care professionals involved in discharge planning and referral processes, could offer deeper insights into the underlying factors contributing to these outcomes.
While not presented in this article, a control group was first constructed using transition probabilities derived from a review of literature and previous studies that had explored transitions of older adults between hospitals, nursing homes, and community-based settings at a regional and national scale. The population studied in these investigations consisted of Medicare fee-for-service recipients, predominantly non-Hispanic White females, which is reflective of the IRTC demographic composition. 21 –23 Aggregate cost savings by year 5 were very similar to the current results at $9,587 per person. Although further research may be needed to provide stronger causal inferences, these projections offer an initial indication that the IRTC program can result in increased benefits that need to be taken into consideration.
Secondly, the cost projections focus only on direct costs associated with the provision of social support services and health care, excluding indirect costs such as caregiver burden, loss of productivity, and other societal costs that might be important from a policy perspective. Despite this limitation, projections in this study indicate that providing social support services to older adults and their families can help them remain independent in community settings while also resulting in cumulative cost savings for agencies implementing such programs.
Lastly, there are some limitations related to the use of Markov Chains for economic modeling. A primary assumption of these models is that future states depend only on the current state, not on the sequence of preceding events. 26 However, since historical health event data, such as prior hospitalizations or nursing home admissions before enrolling in the IRTC program, were not available, a Markov Chain was deemed appropriate for this setting. Moreover, within the data employed to compute transition probabilities, a limited number of transitions from community to nursing homes was noticed. It remains uncertain whether this reflects selection bias or, alternatively, indicates the efficacy of the IRTC program in delaying and preventing nursing home stays. To address the uncertainty, sensitivity analyses were conducted where transition probabilities were conservatively estimated by adjusting upwards the frequency of transitions from community to nursing homes by 20%, 30%, and 40%, which resulted in diminished cost savings. Nevertheless, further investigations may be needed to fully understand and quantify care coordination’s potential in reducing adverse health events and associated costs.
Conclusion
The IRTC program presents a promising approach to supporting older adults, not just from a moral and legal perspective, but also from a financial standpoint. The long-term cost savings, encompassing direct aggregate spending as well as reduced hospitalizations and nursing home admissions, make a compelling case for broader adoption and continuous investment in such care coordination community-based programs. The involvement of ICPs in care coordination processes for older adults should also be considered as a strategy that can enhance these savings. With an aging population and escalating health care costs, these models could very well serve as a cost-saving approach to assisting older adults in Iowa and beyond.
Footnotes
Authors’ Contributions
All authors made substantial contributions to this research. E.S. contributed to the acquisition, analysis, and interpretation of data; drafted the article and agreed to be held accountable for the work. All authors contributed to the conception and design of the work, provided critical revisions to the article and approved the version to be published.
Author Disclosure Statement
K.O. is the OAA Fiscal Coordinator at the Iowa Health and Human Services Division on Aging and Disability Services and oversees the Iowa Return to Community Initiative. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Iowa Health and Human Services Division on Aging and Disability Services.
Funding Information
This work was supported by the Iowa Health and Human Services Division on Aging and Disability Services under contract #2127 with the University of Iowa.