
Abstract
Lung cancer screening (LCS) rates are low, and lung cancer mortality is high in the United States. This report describes a strategy that health systems can use to identify LCS areas of need and engage associated primary care providers and patients in screening. A research team from Jefferson Health (JH), a large, urban health system, used geocoded standardized lung cancer mortality rates (SMRs) to identify zip codes in Philadelphia where lung cancer mortality is high. In addition, health system electronic medical record data were used to identify primary care practices serving these areas. The study also developed an online program to train providers in shared decision making (SDM) about LCS. Finally, primary care leaders were interviewed to learn about training obstacles and opportunities. The JH research team identified 8 high-SMR zip codes and 8 practices with patients from those areas. Working with the American College of Chest Physicians and the National Lung Cancer Round Table, the authors developed a free, online, accredited course to train providers in patient education, values elicitation, and decision support for LCS. Interview analyses with practice leaders encouraged the health system to incentivize provider training and use of SDM tools in practice. Health systems can implement a systematic approach to identify LCS areas of need and train primary care providers to engage patients in SDM about LCS. Research is needed to implement such an approach and evaluate the program’s impact on patient engagement, screening, and related outcomes among patients’ diverse populations.
Introduction
It is well known that lung cancer is the leading cause of cancer-related death among US adults. 1 Over a decade ago, the National Lung Screening Trial showed that for persons at increased risk, lung cancer screening (LCS) with annual low-dose computed tomography (LDCT) had a significant impact on reducing lung cancer mortality. 2 The United States Preventive Service Task Force (USPSTF) and the Centers for Medicare and Medicaid Services (CMS) both recommend annual LCS for older adults (USPSTF: 50–80 years of age; CMS: 50–77 years of age) with ≥20 pack/years of cigarette smoking exposure and currently smoke or who quit smoking within the past 15 years. 3,4 USPSTF guidelines recommend shared decision making (SDM), and the CMS requires SDM prior to screening for coverage of this preventive health service. According to CMS guidelines, SDM includes counseling about the risks and benefits of LCS, the use of a decision aid to assess patient values and preferences, and counseling about tobacco treatment for individuals who smoke. 4
Despite these recommendations, SDM is utilized infrequently in primary care, and the quality of SDM, when offered, is suboptimal. 5,6 Prior studies have demonstrated that the utilization of SDM is limited by low provider knowledge about current guidelines and familiarity with SDM as a patient engagement approach. 7 This state of affairs may also be attributed to a lack of SDM training for health care providers, limited time providers have to discuss LCS with patients, and the lack of health system support for SDM performance. 6,8 –10 Furthermore, as LCS rates are low nationally, 8,11 there is a need for a broader, collaborative health-systems approach.
Given their role in supporting the delivery of preventive health care services to those in need, health systems are in a unique position to facilitate provider training in SDM about LCS and, thereby, increase the number of screening-eligible patients who are given access to LCS rates, and, ultimately, raise LCS rates in diverse at-risk populations. Unfortunately, most health systems have not embraced these challenges. 12,13 The current study describes a project that one large, urban health system undertook to develop a strategy to increase SDM and improve rates of LCS utilization in primary care practices that serve patients from geographic areas in which the burden of lung cancer is high.
Methods
Determining areas of need and identifying primary care practices
Geographic identifiers are commonly used to describe population-level sociodemographic background characteristics, identify specific health risk factors, and present information on the burden of disease. 14 Recently, zip code and census tract data have been used to bring together data on population background characteristics in areas experiencing an excess burden of lung cancer. 15,16 Building on methods used in those studies, the research team initiated an effort to identify Jefferson Health (JH) primary care practices that serve patients in Philadelphia zip codes experiencing excess lung cancer burden (see Fig. 1).
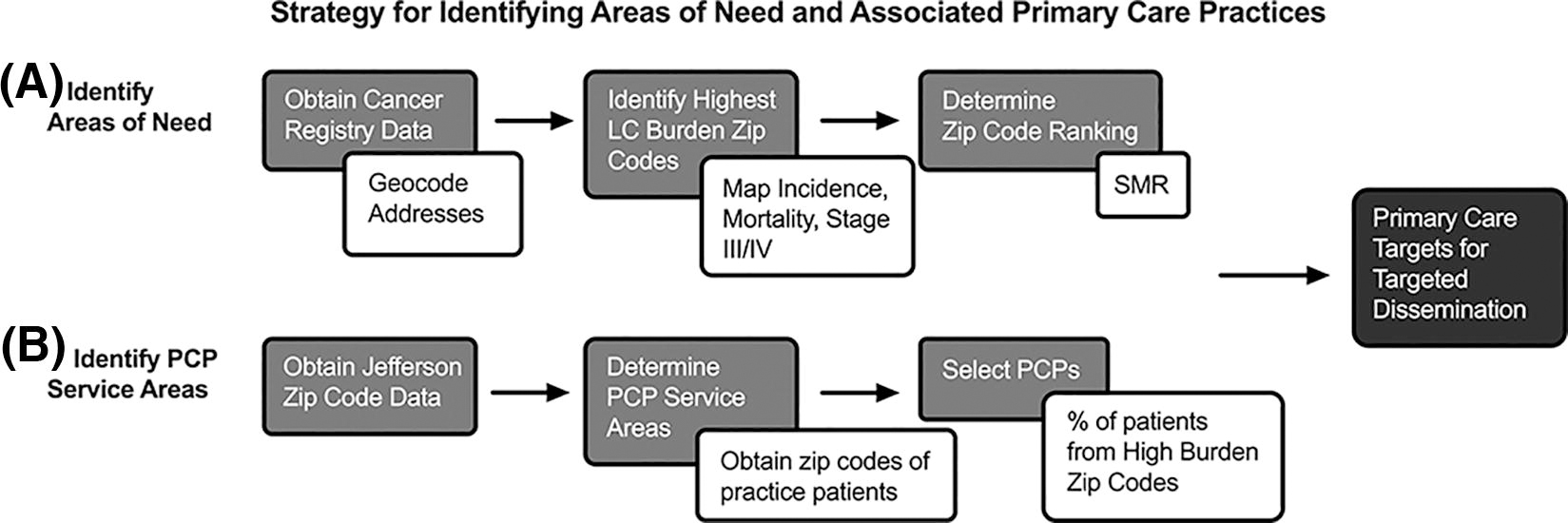
Strategy for identifying areas of need and associated primary care practices. Identification of sites for LCS intervention followed a 2-step approach.
Initially, the study obtained geocoded data from the PA Cancer Registry (2008–2017) and the US Census Bureau (2020). These data were used to determine lung cancer incidence, mortality, and mean stage at diagnosis for Philadelphia County, as well as sociodemographic trends within areas of interest. After review and discussion of these data, the authors found that age-standardized mortality rates (SMRs) were representative of overall disease burden and thus could be used as a metric for health systems to assess the current burden of disease and future impacts of interventions. SMRs were calculated in part using data from the Centers for Disease Control Surveillance, Epidemiology, and End Results program. 17
Initially, the study focused attention on examining census tract data but ultimately decided to use zip code as a geographic identifier to define areas of need. This decision was influenced by the plan to use patient addresses and their associated zip code in the health system electronic medical record (EMR) to identify primary care practices and patients who would benefit most from an effort to increase SDM and LCS. In accordance with this plan and methods used by McIntire et al., 15 Zeigler-Johnson et al., 16 and Walters et al., 18 the study used Zip Code Tabulation Area (ZCTA) crosswalk to align tabulation areas for Philadelphia County and identified 8 zip codes experiencing the highest SMR. 19 Once high-burden zip codes had been identified, the study focused attention on identifying primary care practices affiliated with JH that served patients in these areas.
To identify JH practices serving patients in high-SMR zip codes, the study used health system EMR data to assess the number and percentage of patients who were of screening eligible age under CMS guidelines (50–77 years) and had an address located in one of the high burden zip codes. 4 The criterion for practice selection was that the patient population of the practice comprised >10% of persons from high-burden zip codes. In one identified zip code, the aforementioned methodology determined that there were no JH primary care practices that satisfied this threshold. To ensure that the needs of patients from that zip code were addressed, the authors identified the next most representative under the 10% threshold.
Assessing LCS rates among patients in selected primary care practices
Baseline LCS data were obtained from the health system EMR for selected primary care practices using Qlik®, a software platform that can be used for data visualization, custom analytics, and reporting. This study used compiled EMR data for the practices from January 1, 2021, to December 31, 2021, quantifying the number of patients referred to the health system’s centralized screening program for a LCS LDCT scan, the number of patients for whom an LCS scan was ordered outside the centralized program, and the final number of patients with LCS referred/ordered who completed screening. These data provided baseline LCS measures for practices and patients in the identified high-risk zip codes.
Designing an SDM training program
An initial step toward supporting providers in identified practices involved the identification of a suitable SDM training program. A review of current CMS guidelines revealed that CMS specifies that SDM should involve the identification of patients who are eligible for LCS, the use of a decision aid to educate patients about screening risks and benefits, informing patients about initial and repeat LCS (along with diagnostic follow-up), and helping patients clarify their personal preference related to screening. 4 Thus, it is important for health care providers to learn how to assess patient eligibility for screening, educate patients about screening, and engage patients in SDM about LCS. 7,10,20
Beginning in 2018, Thomas Jefferson University, the American College of Chest Physicians (CHEST), and the National Lung Cancer Round Table (NLCRT) initiated the process of bringing together physicians, researchers, instructional designers, and public health professionals from around the nation to begin developing a short training course for providers on SDM about LCS. Initial discussions led to the development of a unique online training program designed to prepare primary care providers, nurses, and others to engage patients in all aspects of SDM about LCS as defined by CMS coverage guidelines. 4,21
Developing an approach for dissemination
To learn how to disseminate the training program to providers in selected primary care practices, the current study contacted health system leaders to identify practice leaders with whom to conduct key-informant interviews that could guide the dissemination strategy by identifying barriers and facilitators to dissemination. 22 Following Roghanizad et al., 23 the study also developed an educational presentation on SDM and LCS and an interview guide intended to identify important barriers to and facilitators of SDM training about LCS for practice providers. The authors conducted interviews with the on-site representatives for the identified JH primary care practices and used the results to inform the dissemination strategy. 22 While conducting the interviews, research team members kept detailed notes on informant responses and produced transcripts of each interview. Responses were coded and analyzed to identify salient themes.
Results
Identified areas of need
Through an analysis of geo-coded markers of disease severity (SMR), the study was able to identify the 8 Philadelphia zip codes served by JH Enterprise practices with the highest SMR for Philadelphia County: 19142, 19123, 19133, 19147, 19130, 19144, 19139, and 19146 (see Table 1). Zip code 19127 was initially included based on an SMR of 14.9 but was subsequently removed as it was deemed nonresidential with a population of <5000 residents. Demographic data for the identified zip codes showed populations within selected zip codes were 66.0% non-White, 14.9% over 25 years without a high school (or equivalent) degree, and 26.7% at less than 125% of the poverty line.
Identified Areas of Need
Identified primary care practices
Using the aforementioned criteria, the authors selected 7 primary care practices with greater than 10% of their patient population residing in the 8 highest SMR zip codes in Philadelphia County. An additional practice (Practice H) was included that did not meet the 10% threshold as it provided further coverage to zip code 19130, which otherwise had less than 50% of Jefferson patients covered by the practice selection criteria. In total 8 primary care practices were selected, covering 91% of Jefferson patients in high-SMR zip codes, with all nonselected practices combined serving 9% of patients from selected zip codes (see Fig. 2). As all nonselected practices represented <10% of patients, the authors found further inclusion would result in diminishing returns and increased resource strain. Selected practices saw a wide range of total number of patients as there was no set threshold for the number of patients served, only the percentage of patients from high-burden zip codes. The 8 selected practices served between 112 and 2080 patients from high-burden zip codes, with a mean of 837 and a median of 407.
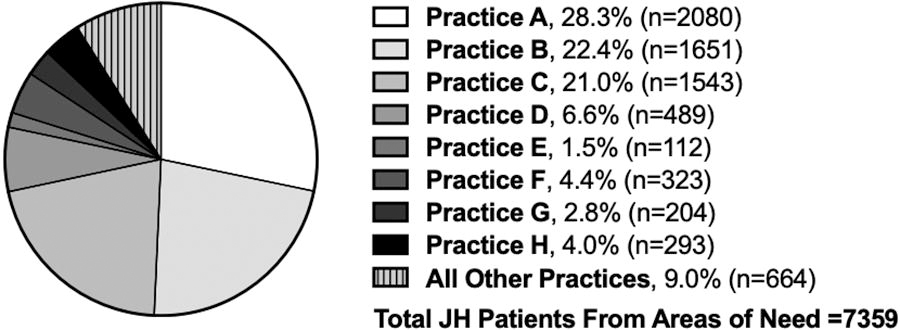
Patients and practices in areas of need. In 2021, Jefferson primary care practices served 7359 Jefferson patients from areas of need (see Table 1). Practices A–H cared for 6695 (91%) patients, and all other practices cared for 9% of patients. In Practices A–G, patients from areas of need accounted for at least 10% of the practice–patient populations. Practice H did not meet this threshold but was included to provide greater than 50% coverage to Jefferson patients in zip code 19130.
Baseline LCS rates in practices
Analysis of 2021 LCS data across the 8 selected primary care practices yielded a total of 826 LDCT screenings ordered with only 251 being completed (30.4%). Orders and completion percentages varied across practices (see Table 2) and depending on whether they were outside of, or within, the centralized Jefferson Lung Cancer Screening Program (JLCSP). Individual practice screening completion percentages ranged from 0% to 42.1% with total screening referrals ranging from 3 to 321 and completions ranging from 0 to 72. The 278 screenings ordered outside of JLCSP resulted in a completion percentage of 26.6% and the 548 orders to the JLCSP carried a completion percentage of 32.3%. Overall, 826 LCS orders were placed in 2021 and 30.4% were completed.
2021 Baseline Low-Dose Computed Tomography Screening Data for Practices Serving High-Risk Areas
JLCSP, Jefferson Lung Cancer Screening Program.
The SDM training program
The collaboration involving Thomas Jefferson University, the American College of Chest Physicians, and the NLCRT resulted in the development of a brief, self-directed, accredited, online training course that includes 3 modules, which prepares the learner to (1) assess patient eligibility for LCS, (2) educate patients about lung cancer and LCS, and (3) help patients make a shared decision about screening. 21 Learners can access this course, Shared Decision Making in Lung Cancer Screening, online at: https://www.chestnet.org/store/products/standard-products/elearning/updated-shared-decision-making-in-lung-cancer-screening.
In the initial launch of the course in 2021, providers who registered for and completed the modules (N = 91) showed a 59% increase in SDM and LCS knowledge (unpublished data). More specifically, only 14% of learners were able to answer all questions on the course pretest about LCS and SDM correctly; while after completing the course, 73% answered all post-test questions correctly. Furthermore, of those who completed all 3-course modules and the course evaluation, 99% agreed that the course met its stated objectives, and 90% reported that they intended to change their approach to SDM and LCS. These preliminary data suggest that encouraging course completion among primary care providers could help to increase SDM and LCS rates in practice. 12
Planning to disseminate the SDM training program
On-site interviews with practice leaders revealed crucial information for the development of an effective dissemination strategy. These interviews revealed the importance of utilizing existing education-dedicated time at the practices to outline the project’s purpose and goals and provide time for the completion of modules. The use of this preallotted time was a focus of many of the practice–leader interviews as this could minimize the provider fatigue from additional time obligations associated with the training. The authors aim to use this education-dedicated time to emphasize the importance of SDM and LCS, and interviews with practice representatives suggested that highlighting the importance of SDM and LCS as potential future quality-performance metrics could further incentivize engagement. The interviews indicated a desire for practice-specific guidance on the LCS referral process and instruction on when an individual order should be placed or a referral to a centralized program. Furthermore, the interviews identified potential noncash incentives such as accreditation, certification, and awards that were deemed desirable and could be used to promote engagement and completion of the training modules. Interviewees suggested the utilization of practice-specific digital communication channels to reinforce engagement with the training materials both before and after the dissemination meetings to create a multifaceted dissemination approach that employs top–down dissemination from central leadership, as well as peer–peer dissemination through these specified channels that could be facilitated by on-site leadership. Finally, the no-cost, self-directed, and remote-optional aspects of the modules were identified as factors supporting engagement as they supported participant autonomy and flexibility.
Discussion
The methodology described in this study establishes a framework for health systems to address the need to increase SDM and LCS practices that serve patients in areas of need. The identification of high-burden areas highlights the potential value of using geospatial analysis to target at-risk populations for intervention. 14 –16,18 While previous studies have used a similar methodology to identify practices serving high-burden areas, 15,16 those studies did not provide guidance on how the health systems could embrace the challenges of training to the practices and providers that serve patients from areas of need in SDM about LCS. The current study addresses this need.
By selecting areas of need by greatest SMR (while excluding nonresidential areas such as 19127) as a method of quantifying disease burden, the research team was able to target high-impact geographic areas for the allocation of resources in a strategic manner. 15,16 During the project, the authors considered an alternative methodology that would utilize SMR data directly from census tracts, rather than first using zip codes to establish areas of need and subsequently identify practices for intervention. However, the catchment area for some practices encompassed the whole of Philadelphia County, making it difficult to target specific census tracts for intervention. The methodology used to select practices serving high-burden zip codes allowed for the identification of primary care practices with a substantial number of patients who resided in identified zip codes. Further research is needed to identify the optimal approach for identifying geographic areas of increased burden of disease to ensure equitable coverage for patients from diverse populations served by the health system.
The SDM training program was tailored to the goals of this project. The multidisciplinary team cultivated through collaboration between representatives from Thomas Jefferson University, CHEST, and NLCRT created a resource that improved providers’ understanding of LCS with a focus on the patient-centered approach that is the core of SDM. 21 The focused nature of the 3 modules on the key aspects of patient eligibility, patient education, and SDM allowed for an efficient yet effective manner of material delivery that worked within the time constraints of providers while still creating a benefit to provider knowledge and implementation. The early data from pre- versus post-module knowledge checks and provider indications to change practices on LCS are an indicator of the success of this training program, making it an appropriate candidate for this dissemination project. 7,10
Finally, the identification and engagement of practice leadership in completing key-informant interviews was crucial to the training program planning process, as these conversations and predissemination interviews identified barriers and facilitators to uptake of educational resources in a timely manner, allowing for the optimization of the dissemination process. 22 These interviews affirmed the existing time constraints that providers face, emphasizing the importance of using preallotted education-based time, such as grand rounds, for delivery of the study’s message. Furthermore, the utilization of traditional motivation tactics, such as the inclusion of noncash incentives or education accreditation were highlighted as key adjunctive strategies to enhance provider engagement.
Limitations
The baseline data for this study were limited by the fact that the patients comprising the 2021 LCS data do not necessarily map to a 1:1 LCS order to LCS completion relationship. Some patients had LDCTs ordered in 2021 but underwent screening in 2022, and some were undergoing interval follow-up from prior LCS counseling with orders falling outside of 2021.
In addition, the underutilization of LCS and the focused scope of this study to 8 practices created an inherently small sample size. However, this can be remedied by expanding the initiative to the whole JH enterprise to involve a greater number of zip codes and practices. Despite the small sample size, the LCS trends were consistent with previous studies, 8,11 with the utilization being low overall, and with higher completion rates in the centralized program. 24 These trends are expected to remain consistent in future initiatives.
While the current study used zip codes to estimate geographic trends in lung cancer mortality and collect associated sociodemographic data, the use of zip codes is not necessarily an optimal approach for evaluating population-based health data. The primary issue in using zip codes for this type of project is that census tract level data does not always align with zip codes, making the evaluation of data across resources and organizations more difficult and necessitating the use of the ZCTA crosswalk. 19 That said, the authors found it necessary to use zip codes in this project as the JH system organizes patient data at the zip code level and hence, it was necessary to determine the catchment area of each practice as this project was facility focused. However, the authors do not recommend or endorse the use of zip codes as opposed to census tract data for similar future projects.
Future directions
Further work is needed to disseminate the learning modules of this project and analyze the realized uptake and in-practice impact to fully inform the success of this dissemination project for application to future works. After analyzing and refining this smaller-scale dissemination a similar strategy can be used for a health system-wide dissemination of SDM/LCS training, followed by implementation of similar programs across the state and country. Nationwide dissemination of the LCS and SDM modules can improve primary care LCS practices and lessen the burden of lung cancer among US adults. 12,13
Currently, the disparities in lung cancer extend from the screening-eligible period through mortality, with individuals of color less likely than their white counterparts to receive early diagnosis, and more likely to suffer poor outcomes. 25 As screening interventions fail to equitably reach these groups, further work is needed to create interventions to increase LCS uptake within these communities. 11 Through equitable distribution of LCS education resources to the highest-burden areas, health care systems can lessen the disparities that exist in lung cancer and improve patient outcomes. 12 The current study confirms that LCS fails to reach lower socioeconomic status population groups through the demographic trends in identified high-burden zip codes (see Table 1), 11 with a disproportionate number of patients from the identified areas of need coming from minority-race, under-educated, or low-income backgrounds. These trends confirm the need for targeted LCS intervention with a focus on underserved and highly impacted areas as outlined in this study to reduce the inequitable burden of disease and improve health outcomes. 11,12
Future work can examine exactly how patient populations reflect area demographics and assess how demographics differ between the target population, patient populations, patients referred for LCS, and patients who undergo LCS. Such work can highlight potential areas for intervention to alleviate barriers to patients accessing care with an ultimate goal of improving health equity in lung cancer from the identified trends in LCS (see Table 1). 11
Conclusion
Action is required to improve the low utilization of LCS in primary care to improve lung cancer outcomes among US adults. A systems-based dissemination strategy that targets SDM and LCS training resources to primary care providers serving areas of high lung cancer burden can improve provider knowledge and patient uptake of LCS. By implementing such a need-based intervention, health care systems can alleviate existing disparities in LCS and lung cancer outcomes. Further work is needed to analyze this strategy’s future impact on LCS and confirm the demographics of patients receiving benefits of improved LCS match those of the targeted geographies.
Footnotes
Acknowledgments
The authors would like to thank the Bureau of Health Statistics and Registries, Pennsylvania Department of Health, Harrisburg, Pennsylvania, for providing access to Pennsylvania cancer registry data. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations, or conclusions. In addition, the authors would like to express appreciation toward those JH primary care providers who participated in key informant interviews.
Authors’ Contribution
G.M.: Writing—original draft preparation, writing—reviewing and editing, and visualization. C.Z.-J.: Conceptualization, methodology, investigation, formal analysis, and writing—reviewing and editing. M.D.: Conceptualization, methodology, investigation, formal analysis, and writing—reviewing and editing. C.S.S.: Data curation, investigation, and formal analysis. K.P.: Methodology and investigation. R.M.: Conceptualization, project administration, funding acquisition, methodology, supervision, validation, and writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part by funding provided by