
Abstract
In recent decades, the integration of artificial intelligence (AI) into health care has revolutionized diagnostics, treatment customization, and delivery. In low-resource settings, AI offers significant potential to address health care disparities exacerbated by shortages of medical professionals and other resources. However, implementing AI effectively and responsibly in these settings requires careful consideration of context-specific needs and barriers to equitable care. This article explores the practical deployment of AI in low-resource environments through a review of existing literature and interviews with experts, ranging from health care providers and administrators to AI tool developers and government consultants. The authors highlight 4 critical areas for effective AI deployment: infrastructure requirements, deployment and data management, education and training, and responsible AI practices. By addressing these aspects, the proposed framework aims to guide sustainable AI integration, minimizing risk, and enhancing health care access in underserved regions.
Introduction
Since the 1970s, artificial intelligence (AI) tools have ushered in a transformative era in health care, permeating multiple aspects of health care delivery. From diagnostic imaging 1,2 and predictive analytics 3,4 to personalized treatment recommendations, 5 –7 AI-powered technologies hold immense potential to revolutionize medical practices in high-income countries (HICs) and broaden access to health care in low-resource communities. With a projected global shortage of 10 million health care workers by 2030, 8 AI innovations in telemedicine and remote monitoring may address persistent health inequities in areas facing physician and specialist shortages. 9,10
As digital health tools have rapidly evolved, integrating knowledge from various medical disciplines, regulatory mechanisms must keep pace with their advancements while also protecting user health and safety. While much of the discourse has centered around HICs, the challenges and opportunities of implementing AI in low- and middle-income countries (LMICs) demand attention. Limited digital infrastructure, privacy concerns, and algorithmic bias must be addressed to effectively and responsibly integrate AI-based tools within existing health care systems. Furthermore, for AI technologies to reach their full potential, current health care systems must adapt through personnel training, economic strategies, and improved communication frameworks.
In this article, the authors conduct a literature search and expert interviews to examine how AI-powered health technologies can be responsibly deployed in low-resource environments. The article focuses on 4 critical areas: (1) infrastructure requirements, (2) deployment and data management, (3) education and training, and (4) responsible AI practices. Here, AI is defined as any technology enabling machines to perform tasks that would otherwise require human intelligence or intervention. 11 The focus on “low-resource” settings refers to geographic areas and populations (in both HICs and LMICs), which lack access to health care services.
Methodology
The study was conducted in 2 phases. First, a literature search was conducted to identify and analyze the challenges and opportunities of AI-based medical tools in low-cost settings, particularly in LMICs. Next, the authors conducted semi-structured qualitative interviews with experts to validate this framework and identify potential gaps. The pooled findings from the literature search and interviews were synthesized and integrated into a refined framework for responsible deployment of AI-powered health technologies in low-resource settings.
Literature search
To capture relevant studies, PubMed (n = 8), IEEE Xplore (n = 11), Scopus (n = 68), and Google Scholar (n = 17) were searched for original research studies (ie, randomized controlled trials), review articles, government reports, meta-analyses and systematic reviews, case studies, perspective articles, correspondences, book chapters, or technical reports. The search was limited to articles published in English from January 1, 2010 to July 20, 2024. The authors specifically sought studies addressing the application of AI in health care within low-resource environments. Details regarding search terms and keywords are provided in Supplementary Appendix SA1.
Retrieved search results were imported to Zotero and duplicates were removed. Inclusion criteria were as follows: (1) focused on the application of AI-based tools in medicine, (2) describes technology in low-resource settings, specifically LMICs, (3) original or reviewed, written in English, and published in a peer-reviewed journal. All identified articles were imported into a reference management software (Zotero), reviewed, and screened to assess their eligibility based on the inclusion criteria. Full-text articles were retrieved from studies deemed potentially relevant. Key findings were extracted, focusing on AI technologies used, their medical applications, and unique challenges and benefits observed in LMIC settings. Noteworthy studies and themes were highlighted and summarized to provide a comprehensive overview of the current landscape.
Stakeholder interviews
Given the paucity of literature on AI-powered technologies specifically tailored toward addressing health disparities, the authors conducted virtual interviews (Zoom) with expert stakeholders in the field of medical AI for health equity. Through these interviews, they sought tangible insights into the practical challenges and opportunities of implementing AI-based tools in low-resource settings.
The authors identified and mapped potentially relevant stakeholders through official university websites, search engines, and global health conference speakers. Interviewees were purposively selected to include a diverse range of perspectives, from health care providers (n = 2), AI tool developers (n = 3), health care administrators (n = 2), academic professors (n = 2), and government consultants (n = 2), and representatives from nongovernmental organizations (NGOs) working in LMICs (n = 4), with strong representation from sub-Saharan Africa and Southeast Asia. Invitations were sent via email, and interviews were scheduled based on participant availability.
Semi-structured interviews were conducted between February 7, 2024 and July 1, 2024, using a predefined interview guide (see Supplementary Appendix SA1: Interviews). Topics covered included: Experiences with AI-based tools in health care Perceived benefits and challenges Implementation strategies Recommendations for future research and practice
Eight interviews were conducted via video call and lasted approximately 60–90 minutes each. Each interview contained 1 primary interviewer and 2 note-takers? This mixed-methods approach allowed for a comprehensive understanding of the use of AI-based tools in medicine in low-resource areas, combining empirical evidence from the literature with practical insights from field experts. The authors manually performed a thematic analysis, extracting recurring concepts from interview notes and drawing connections between interviews and the literature search. Key considerations were identified for implementing medical AI in low-resource settings, which were then categorized into 4 pillars: (1) infrastructure requirements, (2) deployment and data management, (3) education and training, and (4) responsible AI practices.
Current Applications of AI in Health Care
AI has become a valuable asset in clinical decision-making, helping health care professionals diagnose and treat conditions earlier and more accurately. 1,2 Tools like OpenAI’s ChatGPT, which passed the U.S. Medical Licensing Exam, 12,13 use patient histories and peer-reviewed literature to provide evidence-based recommendations and insights on therapeutic strategies. 5 –7
AI-powered technologies applied to health care administration enhance health care systems by streamlining screening, triage, 14 –16 and remote support, 17 and optimizing administrative processes like appointment scheduling, billing, and electronic health record management. These technologies also simplify medical documentation and bridge language gaps where interpreters are unavailable, improving efficiency and enabling providers in low-resource settings to dedicate more time to patient care.
Generative AI tools in medical education enhance the accessibility of medical knowledge by simplifying technical terms for patients. These tools provide personalized health information, treatment options, and medication reminders, promoting proactive health decisions. 18 –20 AI-powered chatbots and virtual assistants facilitate interactive communication, addressing patient queries and concerns. 17 These technologies also support the training of medical professionals and community health workers, introducing new procedures and medical concepts. 21,22
AI-powered tools may also leverage predictive analytics to assess and mitigate patient risks effectively. 23,24 By analyzing demographic, medical history, and lifestyle data, AI algorithms can identify individuals at higher risk for conditions like hospital readmissions or psychiatric emergencies. 25,26 This allows health care providers to implement personalized interventions and targeted monitoring, 27 –29 enhancing preventive care for high-risk patients, with applications including cardiovascular risk assessment and chronic disease predictions. 30
Infrastructure and Capacity Requirements
Physical requirements
According to the World Bank Group, low-income countries have an average rural population of 65%, with only 20% using the internet, compared with 19% rural populations and 90% internet usage in HICs. 31 This digital divide, driven by disparities in income, power access, urbanization, and connectivity, underscores the need for tailored infrastructure solutions in LMICs (Fig. 1). Baseline physical and safety requirements must be considered when deploying, implementing, and operating AI systems:
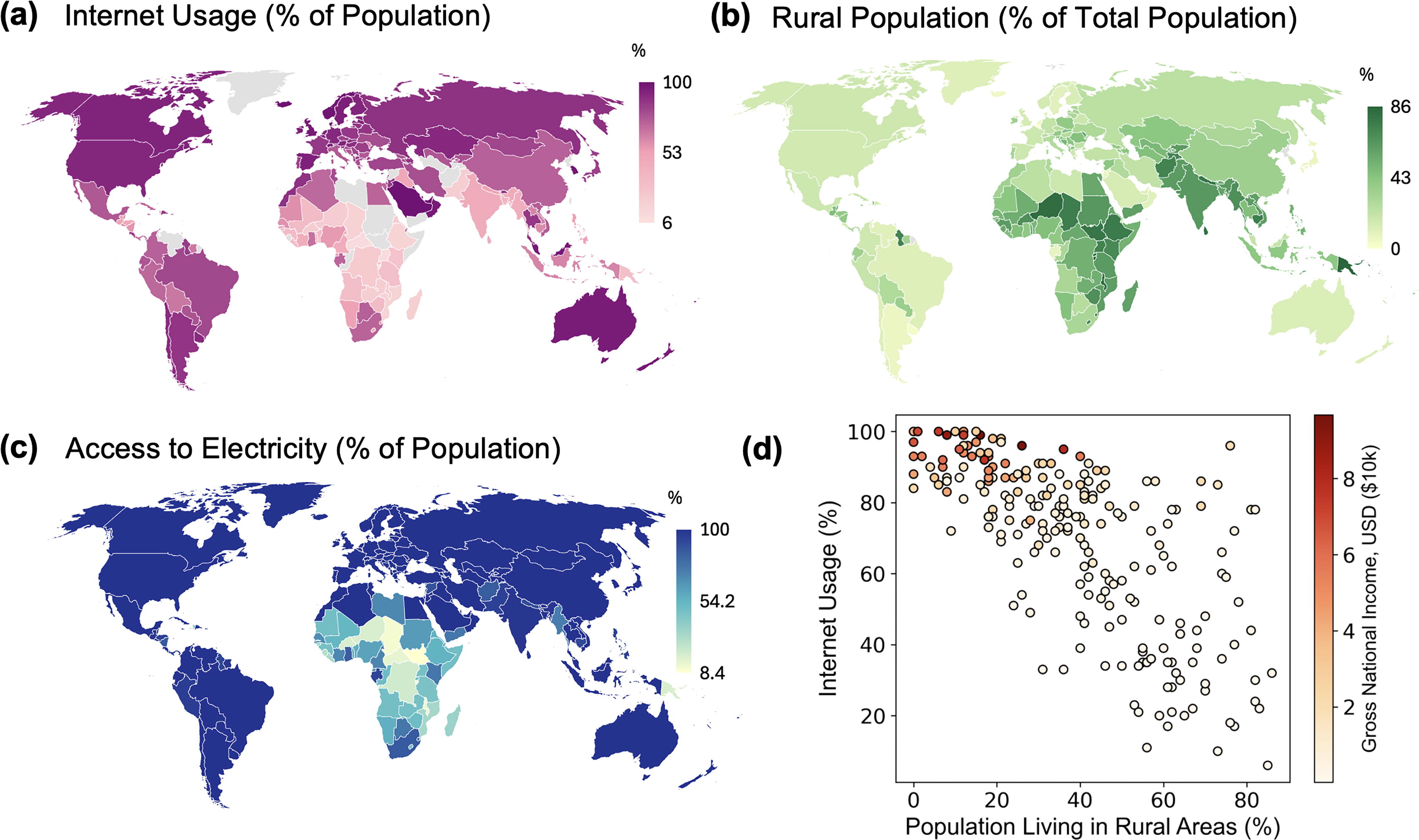
Visual representation of
Functional requirements Electrical grid Computer servers Trained operators/users Internet connection Physical medical record storage Secure facilities
Responsible implementation Standardized AI/software operating procedures Information technology (IT) staff for training and maintenance Local enterprise systems or offline backup for power loss “Human-in-the-loop” (ie, for clinical decision support tools)
Meeting these physical requirements often involves significant investment and coordination with regulatory agencies, which may be readily available in HICs but require careful planning in under-resourced settings. While a single smartphone with internet access can support AI for health care use, 32 –34 such systems may lack robust safety mechanisms and quality assurance. Before deploying AI-powered technologies, local stakeholders should conduct risk assessments for AI use in optimizing patient health outcomes. Community input is crucial in defining “acceptable” risk, as having transparent discussions about potential AI risks and benefits builds trust and empowers local stakeholders in their own health care decisions. Furthermore, local risk-benefit analyses provide an opportunity to tailor AI deployment to the specific needs of each community. For instance, in remote settings, where access to physicians is extremely limited, 8 the benefits of using smartphone-powered AI medical tools may vastly outweigh potential risks of implementation—and the consequences of nonimplementation may be even greater. In contrast, in high-income settings with greater densities of physicians, the risk-benefit assessment would shift. While there are few universal measures of health care access, indirect indicators like physician density and life expectancy may help assess needs. For instance, HICs have an average life expectancy of 69 years and 36 physicians per 10,000 people, while low-income countries average 47 years and just 3 physicians per 10,000 people. 8 Thus, local risk assessments—particularly those guided by community-centered decision-making—provide valuable opportunities to address health care disparities in low-resource settings.
The existing challenges in AI infrastructure in LMICs present tangible opportunities for innovation and development. For example, partnerships like Zambia’s Medland Hospital with private telecommunications providers help address connectivity issues, allowing patients in remote regions to access physicians via telemedicine. 35 Beyond improving health care access, AI can automate or streamline administrative hospital operations such as patient triaging, 14 –16 scheduling, 36 inventory management, 37 and diagnostic imaging in areas with provider shortages. 1,2 Lastly, in addition to optimizing hospital heating, ventilation, and air conditioning systems and reducing strain on local electrical grids, AI-directed streamlining improves the environmental sustainability of the health care system and reduces the number of health care personnel needed without sacrificing high standards of care.
Digital requirements
Creation of robust data infrastructure
Delivering health care in any setting necessitates the exchange of substantial personal health information, which can be stored physically or electronically. Both formats require privacy measures: physical records need locks and custody logs, while electronic records demand various cybersecurity protocols. Health data protection encompasses 2 main areas: security (preventing unauthorized access) and privacy (preventing unauthorized data release). Ensuring robust data security and privacy for electronic health records can be resource-intensive, requiring trained IT personnel and continuous monitoring. Nevertheless, achieving optimal data security and privacy while delivering health care benefits is an ethical imperative, as it safeguards patient trust, ensures regulatory compliance, and enhances the overall effectiveness of health care delivery. 38
Data privacy and selection
Creating a robust data system poses specific challenges. Different hospitals and clinics may lack or use different data management systems, leading to inefficiencies and data duplication that hinder AI integration. While open-source databases can enhance communication, they also expose patient data to security risks. Establishing a standardized hospital management system and a comprehensive electronic medical record database is a crucial first step for responsible AI deployment. Ongoing maintenance and improvement of these databases are essential to ensure compatibility with evolving AI systems. There is a concerted effort across the industry to develop local datasets for large language models (LLMs), with universities in Kenya, Rwanda, and Nigeria working on clinical decision support tools through a Gates Foundation challenge, for example. Clinical trials will assess the efficacy of these tools using locally curated datasets, ultimately aiming to centralize patient data and health care delivery in these communities.
Personnel and communication
Deploying AI in health care requires specialized roles, including health IT specialists to manage digital infrastructure, troubleshoot technical issues, and ensure system functionality; AI trainers to educate health care providers integrating workflows; and clinicians with AI expertise to oversee responsible use of AI in clinical decision making. While these pose considerable initial costs, building local capacity through tailored training programs is vital for sustainable AI deployment, particularly in low-resource settings where external support may be limited.
Furthermore, effective communication systems are required for the integration and operation of AI-based tools. Specific needs include interoperable systems for seamless data sharing between medical facilities; stakeholder channels to establish clear communication pathways between providers, patients, and policymakers; and standardized reporting for consistent feedback and accountability, ensuring alignment of AI tools with local needs. These elements ensure AI tools enhance—rather than disrupt—existing workflows.
Deployment and Data Management
Data management
The quality of data used to train AI models plays a pivotal role in their effectiveness: just as impurities in fuel can clog an engine, poor-quality data can impair the performance of AI health tools. 39 Many medical applications of AI require third-party models to be trained on or adapted to local data to improve accuracy and minimize bias. However, many LMICs struggle to meet the data maturity benchmarks outlined by the Health Care Information and Management Systems Society (HIMSS), 40 which require health care organizations to have advanced electronic health record systems with comprehensive data capture, interoperability, and analytics capabilities. This lack of mature data—characterized by duplicates, missing entries, and outliers—often renders third-party algorithms unusable, and physical medical records can also be lost or illegible.
Cleaning data involves detecting duplicates with techniques such as N-grams or clustering, addressing missing data through imputation, and managing outliers with cluster-based or statistical methods. 41 These steps serve to fill gaps in the data without sacrificing valuable information, as well as minimize distortion of data analysis. Nevertheless, the process of cleaning data comes at a high cost, alluding to capacity limitations specifically in low-resource settings. 39 The lack of infrastructure and resources to process large volumes of incoming data poses a major barrier to AI deployment in LMICs.
When comprehensive data cleaning is not feasible, local data collection using ethical and appropriate practices becomes essential. This approach ensures context-sensitive data gathering, which is critical when leveraging Retrieval-Augmented Generation (RAG) architecture to build health care models tailored to specific regional needs. 42 –44 RAG combines traditional information retrieval methods with generative models, allowing AI systems to access relevant data from extensive datasets while generating contextually appropriate responses. 45 This approach can be particularly helpful in low-resource settings by providing health care professionals with timely, evidence-based information that is tailored to local conditions, thereby enhancing decision-making and improving patient outcomes despite limited access to comprehensive medical resources. However, the need to curate local datasets places a considerable burden on local health care workers, 39 who are often overworked and underpaid. Therefore, equitable AI implementation must address these challenges to ensure fair and sustainable adoption.
Research and development
In addition to creating and deploying AI-powered health technologies, continuous evaluation of their performance in both pre- and post-deployment settings is imperative. Pre-deployment testing rigorously assesses AI algorithms for effectiveness, reliability, and biases, while post-deployment monitoring allows for ongoing adaptation to evolving health care environments, both in HICs and LMICs. 46,47 Leveraging open-source AI tools can lower costs and facilitate knowledge sharing within the global community.
Private companies can support this ecosystem by thoroughly evaluating AI technologies and sharing best practices with local health care providers. Hospitals intending to adopt AI technologies should first conduct capability and capacity assessments. Recognizing limitations in capacity can help define a “minimum technology threshold” for effective AI engagement. This could involve requirements such as registering algorithms, maintaining a status dashboard, and conducting basic predeployment tests to ensure system readiness.
Implementation, testing, and maintenance
While advancements in AI-based health care have focused on research and development, responsible implementation strategies are equally vital for successful deployment. 46,47 How AI algorithms are integrated into existing systems can directly influence health outcomes, independent of their predeployment performance. Implementing AI in health care requires a thorough maintenance and assessment plan, which can be managed internally, by the AI vendor, or through third-party organizations like the HIMSS. 48
Three primary implementation strategies include: (1) repurposing existing, publicly available models; (2) developing customized AI systems based on preexisting models; and (3) creating entirely new AI foundations. Each approach presents unique advantages and challenges based on context and objectives. For example, repurposing publicly available AI systems can speed up deployment and reduce resource needs, especially when donor and recipient communities share similar health care data infrastructures. In contrast, developing customized models may require more resources and expertise but can yield better performance and address disparities associated with technology translation to unique settings.
With AI technologies such as LLMs roughly doubling in power annually, deployment requires scalable infrastructure and adaptive governance to accommodate future advancements. As AI capability increases and costs drop over the next decade, health systems must prioritize iterative training and deployment to balance immediate needs with long-term scalability. This forward-facing approach ensures that AI systems remain relevant and impactful as capabilities evolve.
Education and Training: Digital Health Literacy
Digital literacy is defined as the ability to use technology to find, evaluate, and communicate information. 49 In the context of AI in health care, digital literacy reflects users’ ability to operate AI systems with minimal training. This includes patients, providers, administrators, and IT professionals. Significant disparities exist in digital literacy between users in LMICs and HICs, stemming from limited access, distrust of government and technology, and a lack of resources. 50 As shown in Figure 1, there is a 50% gap in electrical power and a 70% gap in internet usage between these groups.
Digital health literacy (DHL)—which combines digital and health literacy—poses a substantial hurdle to AI implementation in health care. Over 70% of adults in LMICs have inadequate health literacy, 51 necessitating increased training and resource allocation prior to AI deployment, more rigorous monitoring during operation, and frequent feedback to ensure effectiveness. Even when infrastructure conditions are met, implementing AI in LMIC health care systems will be more costly and time-consuming than in HICs due to these literacy gaps. Neglecting to address inequities in DHL will lead to the failure of AI applications, as intended users may avoid using systems that detract from health care operations and provide no additional value.
Increasing both digital and health literacy requires enhanced training and education. Building trust in institutions providing digital services will take time and effective leadership. Although studies on educational techniques for improving digital literacy are limited, those conducted show promising results. For instance, Perestelo-Perez et al. found that 70%–80% of participants in several European countries demonstrated excellent integration of DHL competencies after completing massive open online courses (MOOCs), with higher eHeaLS Scale scores observed across all cohorts following the MOOCs. 52 Further research on digital literacy is warranted in LMICs to develop effective strategies for education and training. Additionally, adaptive licensing frameworks can ensure providers are equipped to use AI tools responsibly, offering tailored certification processes for low-resource settings.
Building Trust: Ensuring Responsible AI in LMICs
While addressing infrastructure is critical, building trust in health care AI technologies is equally important. The World Health Organization outlines 6 principles for the ethical use of AI in health care to promote trust: accountability, fairness, data privacy and selection, transparency, explainability, and value and purpose alignment. 53,54 This section discusses these criteria within the context of LMICs, where resource scarcity can pose significant challenges to meeting them effectively.
Accountability involves establishing regulatory frameworks to hold stakeholders responsible for AI system failures, while fairness aims to minimize biases and ensure equitable outcomes. In LMICs, limited infrastructure, expertise, and governance pose challenges to effective monitoring. Implementing “human-in-the-loop” systems and prompt engineering can enhance accountability and monitoring. Regulatory bodies, such as the FDA, 55 recommend that training data be representative of the local patient population, which can be difficult to achieve in LMICs, where data may not be as widely or readily available. Although AI Assurance labs conduct rigorous predeployment bias testing, their focus on elite institutions limits scalability. 56 Instead, LMICs could adopt Reinforcement Learning from Human Feedback (RLHF) 57 and RAG 42 –44 methods to refine AI training and mitigate bias effectively.
These architectural approaches can enhance transparency, which ensures that the use and limitations of AI tools are clear. RAG ensures models are trained on the specific data provided, while RLHF can be tailored to fit specific applications and contexts. Clear disclaimers about technological limitations are also crucial, especially for medical advice. Data privacy and selection protect electronic health records and sensitive information. As discussed in Section “Digital requirements,” achieving data privacy requires robust cybersecurity frameworks. Regulatory guidelines like the General Data Protection Regulation 58 and the Health Insurance Portability and Accountability Act of 1996 59 provide guidelines on processing personal data in medical AI, emphasizing de-identification. Enterprise AI systems help minimize data leakage risks by ensuring that input prompts and underlying data are not externally exposed. Techniques like differential privacy and federated learning can further mitigate privacy risks during AI training. 60 –63 However, cybersecurity remains a challenge in LMICs, 64 and recent efforts by the White House highlight appropriate measures to enhance cybersecurity for rural hospitals. 65
Explainability ensures that AI operations are understandable to developers, health care workers, and patients, and can be attained through user-friendly interfaces and digital literacy programs. Additionally, local health care workers who collect data need effective feedback mechanisms that demonstrate how their data is used and its impact on health care outcomes. This transparency can help build trust and improve their understanding of the data’s importance. Finally, value and purpose alignment with local health care goals must incorporate cultural nuances and unique community needs. AI models should adapt to these differences, grounding their implementation in local contexts and capabilities.
Proactive measures are required to ensure AI accessibility across all settings, including LMICs and underserved communities. High implementation costs risk widening disparities; as a result, current reimbursement mechanisms must evolve to maximize gain from AI-powered technologies. Subsidies, public-private partnerships, and open-access tools may offset initial costs and facilitate adoption in resource-limited areas. Equitable pricing models and fair distribution of technologies—supported by community involvement and transparent policies—are essential for aligning AI with health equity goals.
Market Considerations
The rapid expansion of digital health technologies, including electronic health records, multi-omics data, and wearable devices, has largely accelerated the adoption of AI in health care. Given the anticipated global health worker deficit, 8 AI-powered tools provide ample opportunities to reduce medical expenditures and improve access to health care in low-income regions. Globally, an estimated 13.5% of households face catastrophic health expenditures (over 10% of household income) annually, pushing low-income families further into poverty due to illness. 66 These households often must choose between essentials such as food and accessing health care services, especially accounting for the cost of transportation to medical facilities. In countries such as Kenya, Zambia, and Nigeria, medical tourism to India has emerged as a viable option for patients unable to afford local health care services. Such trade-offs can lead to late-stage or severe diseases, increasing care costs, and diminished economic productivity. 53 Thus, AI’s economic benefits lie in its ability to enhance efficiency and productivity, from supporting understaffed health care systems to enabling early disease detection and management.
Despite the global AI health care market being valued at $19.27 billion, 67 several factors influence the adoption of medical AI within LMICs. One critical barrier to advancing health equity is the fragmentation of the health care sector, 68 where individual providers and organizations implement new technologies in isolation. Many health care institutions in low-resource areas lack standardized clinical protocols, leading to fragmented responsibilities among physicians. This disjointed approach reduces accountability among providers and impacts holistic patient care. To address this, organizations like the International Hospital Federation facilitate knowledge exchange among health care leaders to promote transformative health care delivery. 64 For instance, Baines Intercare Medical Centre in Zimbabwe is pioneering a “group practice” model, involving multiple specialists per patient visit for more cohesive care.
The scarcity of inter-entity collaboration is further compounded by short-term and fragmented funding for digital health solutions, which are often disease-specific and unsustainable. Such funding lacks the longevity required for effective data collection, maintenance, and training—all of which are essential for effective AI implementation. Political dynamics can also affect the sustainability of digital health initiatives. To this end, public-private partnerships between local hospitals and industry allow for marketing and implementation independent of government constraints. For example, Medland Hospital, a health care facility in Zambia, receives private funding from shareholders to expand affordable primary and specialty care to remote areas. Collaborations with private telecommunications entities have enabled Medland to improve high-speed broadband access for data collection and telehealth communications with remote regions—ultimately reducing health care costs while also improving quality and efficiency of care. 35 Additionally, international nonprofits such as the Program for Appropriate Technology in Health (PATH) function as government consulting agencies to facilitate the development, evaluation, and adoption of digital health tools to address persistent global health issues. 69
Another major consideration for LMICs is developing sustainable, climate-resilient health care infrastructure. Reliable electricity access is paramount for emergency care, vaccine storage, sterilization of surgical tools, and medical device operation. Hospitals such as Medland are powered by hydroelectricity, which has become a scarce and expensive energy source. This underscores the need for health care solutions that are resource-effective and sustainable. AI-driven technologies, such as remote data analytics and rapid diagnostics, can streamline operations and reduce energy costs, ensuring sustainable health care delivery in the long term.
AI has the potential to improve efficiency and outcomes at modest costs, but health care systems must carefully consider how to budget for its implementation. Costs may be incorporated into capital expenses, resembling current IT budgeting methods. Alternatively, AI may be accounted for in operating costs, as is done for software as a service (SaaS) platforms. In private hospitals, costs are covered by a mix of public and private payers, while government-funded hospitals rely on public or mixed payer (public and self-pay) systems. 70,71 The revenue structure determines how costs are distributed, whether through taxes, insurance premiums, or patient payments. Budgeting for uncompensated care is essential for equitable access, requiring government regulation to ensure fair pricing and prevent unethical billing or denial of services. This may be funded either as charity care from hospital revenue, donations, and grants or accounted for by assuming bad debt. 72
Sustainable financial models are critical to AI adoption in health care, especially in LMICs. Bundled payments for AI-enabled diagnostics can reduce costs and complexity by packaging multiple services into a single payment structure; public-private partnerships can subsidize implementation costs, leveraging industry investment to promote public health goals. Tailored reimbursement strategies are needed to balance cost recovery with equitable access, thereby accommodating diverse economic and regulatory landscapes within LMICs.
Conclusion
The implementation of AI in low-resource settings hinges on 4 key pillars: (1) infrastructure requirements, (2) deployment and data management, (3) education and training, and (4) responsible AI practices (summarized in Fig. 2). The process begins by leveraging existing AI systems and adapting their algorithms and models to account for factors such as limited resources, diverse populations, and infrastructure constraints. Establishing guardrails throughout technological development is crucial for ensuring data privacy, bias mitigation, and transparency. Furthermore, developing consistent performance monitoring frameworks will help assess the impact of AI tools on health outcomes, enabling timely adjustments to promote equity. Achieving these goals demands collaborative efforts from international organizations, policymakers, and local stakeholders in aligning technological advances with greater health care access for all.

Roadmap for deployment of AI-powered tools in low- and middle-income countries (LMICs) and medically underserved areas. This roadmap outlines a phased approach for the sustainable implementation of AI-based tools in resource-limited settings. The process is divided into 4 primary pillars: infrastructure, deployment and evaluation, education and training, and responsible AI practices. The roadmap emphasizes community involvement, localized data collection, and ongoing monitoring to ensure that AI-powered tools are implemented effectively and ethically in LMICs and underserved regions. Figure created in BioRender.com.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of Michele Barry, Anurag Mairal, and Krista Donaldson from the Stanford Byers Center for Biodesign and Yosefa Gilon from the Stanford Center for Innovation in Global Health in the production of this article. The authors would also like to thank Terry Mwesigwa from Stanford School of Business for early research efforts. Lastly, they would like to thank the following interviewees who contributed their time and expertise to the content of the article: Searchmore Chaparadza (IHF), Miyele Kaliwanda (IHF), Laurie Werner and Olivia Velez (PATH), James Weinstein (Microsoft), Tirzah VanDamme (Microsoft), Este Geraghty (Esri), Ajay Gupta (Health Solutions Research), Karen Eggleston (Stanford Asia Policy Health Program), Dan Desmond and Shanaya Satterfield (Health Equity Consortium), and Kevin Schulman (Stanford University).
Authors’ Contributions
E.W.: Conceptualization (equal), methodology (lead), writing—original draft (equal), writing—review and editing (lead), visualization (equal). A.B.-C.: Conceptualization (equal), methodology (supporting), writing—original draft (equal), writing—review and editing (equal), visualization (equal). M.-J.C.: Conceptualization (equal), methodology (supporting), writing—original draft (equal), writing—review and editing (equal), visualization (equal). D.-R.C.: Supervision (lead), conceptualization (equal), review, and editing (equal).
Author Disclosure Statement
Dr. Rhew is employed by the Microsoft Corporation. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1