
Abstract
Hypertension control remains challenging for many primary care patients. The goal of this study was to implement an evidence-based team approach to improve hypertension control, self-reported health distress, and self-efficacy in adult patients with hypertension at a large academic family medicine practice. The 5-year intervention included team-based medication therapy management, patient-centered behavioral counseling, and home blood pressure monitoring. Pre- and post-intervention blood pressure and patient surveys were analyzed using paired t-tests. The authors observed significant decreases in systolic blood pressure (148.4 vs. 135.6, P = 0.001) and self-reported health distress over the enrollment period in participants who completed the study. The multidisciplinary intervention was associated with reduced systolic blood pressure and health distress in patients who enrolled and completed the program. A multidisciplinary blood pressure monitoring program can be implemented by providers referring patients with uncontrolled hypertension after pharmacologic interventions.
Introduction
Jefferson Family Medicine Associates (JFMA) is a large primary care practice located in downtown Philadelphia whose patient population experiences high rates of hypertension (54.9% at the start of the study) and low rates of blood pressure control. JFMA has a high prevalence of complex health-related social needs that may contribute to these patients’ vulnerability to uncontrolled hypertension. 1 Studies show that pharmacologic treatments alone fail to lower blood pressure in patients from socially and economically disadvantaged backgrounds. 2 Fortunately, evidence points to the success of multi-pronged approaches involving self-monitored blood pressure (SMBP), behavioral counseling, and multidisciplinary collaboration in improving BP control and reducing cardiovascular disease risk. 3 –5 Unfortunately, uptake of SMBP remains low, and more evidence is needed for SMBP interventions that are feasible to implement in routine primary care practice, particularly for diverse patient populations. 6,7 Based on these factors, we identified an opportunity to incorporate SMBP at JFMA to improve hypertension control.
SMBP implies a patient would, on a day-to-day basis, measure and work to improve blood pressure control with lifestyle changes. Necessarily, this would depend on patient self-efficacy and may be modified by any distress related to living with hypertension. 8 Research on hypertension control emphasizes that successful health outcomes hinge on patients’ confidence in their ability to manage their health conditions. 9 Furthermore, the ability to cope with distress brought on by a chronic disease such as hypertension may impact a patient’s engagement in self-management. 10 Therefore, the researchers assessed how involvement in a multidisciplinary hypertension control program affected patients’ self-efficacy and health distress.
The primary aim of the study is to assess whether hypertension control at JFMA can be improved through the implementation of an integrated, multidisciplinary approach that includes team-based medication therapy management, patient-centered behavioral counseling, and home blood pressure monitoring (HBPM). In addition, the researchers assessed patient self-efficacy and health distress related to hypertension before and after receiving education, training, and monitoring blood pressure at home.
Methods
This study was implemented at JFMA, a family medicine clinic in Center City, Philadelphia, over a 5-year period (2019–2023) in the form of a prospective non-randomized intervention with a pre–post evaluation design. Funding was provided by the Centers for Disease Control and Prevention (CDC) 1817 grant administered by the Philadelphia Department of Public Health. The study protocol, consent forms, and all other study materials were approved by the Thomas Jefferson University institutional review board and the Philadelphia Department of Public Health’s institutional review board.
Screening and recruitment
Eligible study participants were identified via direct provider referral and an electronic health record outreach report. Eligible patients included English-speaking adults aged 18 or greater who had Medicaid as their primary insurance and had a new or existing diagnosis of hypertension (systolic blood pressure [SBP] ≥140 mmHg or diastolic blood pressure [DBP] ≥90 mmHg). Project staff contacted potential participants via phone outreach and MyChart messaging. Patients who were pregnant or incarcerated were excluded. All participants provided their verbal informed consent prior to inclusion in the study.
Intervention
The authors developed an intervention that consisted of an initial enrollment appointment and subsequent follow-up appointments. During the initial appointment, participants met with a clinical pharmacist to review their hypertension history, screen for hypertension comorbidities (obstructive sleep apnea, alcohol, and smoking), identify blood pressure targets and address any potential barriers to hypertension control. The pharmacist identified lifestyle modification opportunities with the patient. These screenings were supported using a visit template in the electronic health record that included validated screening tools: (( S: Snoring, T: Tiredness during the day, O: Observed apnea (witnessing breathing pauses during sleep) P: Pressure (high blood pressure or on blood pressure medication), B: Body mass index (BMI) greater than 35, A: Age over 50, N: Neck circumference greater than 16 inches (40 cm), G: Gender (male) (STOP-BANG)), 11 Alcohol Use Disorders Identification Test, 12 and a one-question medication adherence screen, as well as prompts for key history elements. A research coordinator assisted with ordering and obtaining a home blood pressure monitor, provided instructions on proper HBPM technique, and then administered the pre-intervention survey. Participants were instructed to monitor and log their blood pressure at home daily and were scheduled for follow-up appointments within 2–4 weeks.
At subsequent follow-up visits, home blood pressure data was reviewed, ongoing education was provided, and treatment changes were initiated with the primary care provider's direction. A research coordinator administered the post-survey once patients graduated from the program. Patients graduate when they meet blood pressure goals or by patient choice.
Measures
Demographic data was collected from electronic health record review, including sex, race/ethnicity, and age. Clinical data, such as body mass index, tobacco/alcohol use, lipid numbers, and glomerular filtration rate, in addition to each patient’s current medication list (not reported here), were documented. The dates of initial and follow-up appointments were recorded.
The research team collected patients’ ambulatory blood pressures in both pre- and post-enrollment in the study. They also collected data on patient self-efficacy and health distress using the Self-Efficacy for Managing Chronic Disease 6-item Scale, 8 and an adapted version of the Health Distress Scale from the Self-Management Resource Center, 13 (see Table 2). In the final 2 years of the study, process measures regarding recruitment approaches were collected to determine which approach was most effective.
Analysis
Data was stratified into two categorical groups based on whether the patient completed the study. Descriptive statistics were used to describe the baseline demographic characteristics of each group. A pre-post design was used to assess changes in SBP, DBP, self-efficacy, and health distress (initial visit vs. follow-up visit) for each group using paired t-tests. The researchers defined pre-intervention blood pressure as the average of the first three blood pressures recorded at the initial visit to the hypertension team. Post-intervention blood pressure measurement was defined as the average of three blood pressures recorded at the last visit to the hypertension team, or the last recorded blood pressure at a primary care visit at the end of the study period if a patient was lost to follow-up. Changes in SBP and DBP were evaluated for the entire study sample (initial visit vs. most recent department encounter) using paired t-tests. All analyses were conducted in IBM Statistical Product and Service Solutions (SPSS) Statistics Version 27, with P < 0.05 indicating statistical significance.
Results
Out of 619 patients contacted during the study period, 111 were reached and 90 scheduled an initial appointment. Patients were successfully reached via MyChart messaging 16% of the time compared to 21% of the time via phone calls. Fifty-three patients attended an intake appointment and completed the pre-survey (Table 1).
Demographics
BMI, body mass index; Std, standard.
Twenty-eight participants completed post-surveys and therefore completed the study. Twenty-five participants did not complete the post-survey and were lost to follow-up or chose not to complete the study. Of the 53 participants who completed the pre-survey, most were women (n = 45, 84.9%), and most identified their race as Black (n = 50, 94%). There was a significant reduction from pre-survey to post-survey in mean health distress scale score (1.02 to 0.63), P = 0.001*. There was a significant reduction in the systolic pressure for those who completed the program (148.4 mmHg to 135.6 mmHg, P = 0.001). (Table 2 and Figs. 1 and 2).
Pre and Post-Intervention Survey Results for Study Completers (n = 28)
Overall health distress was calculated by combining these variables and averaging the score.

Systolic blood pressure (mmHg) before and after intervention (n = 23**).
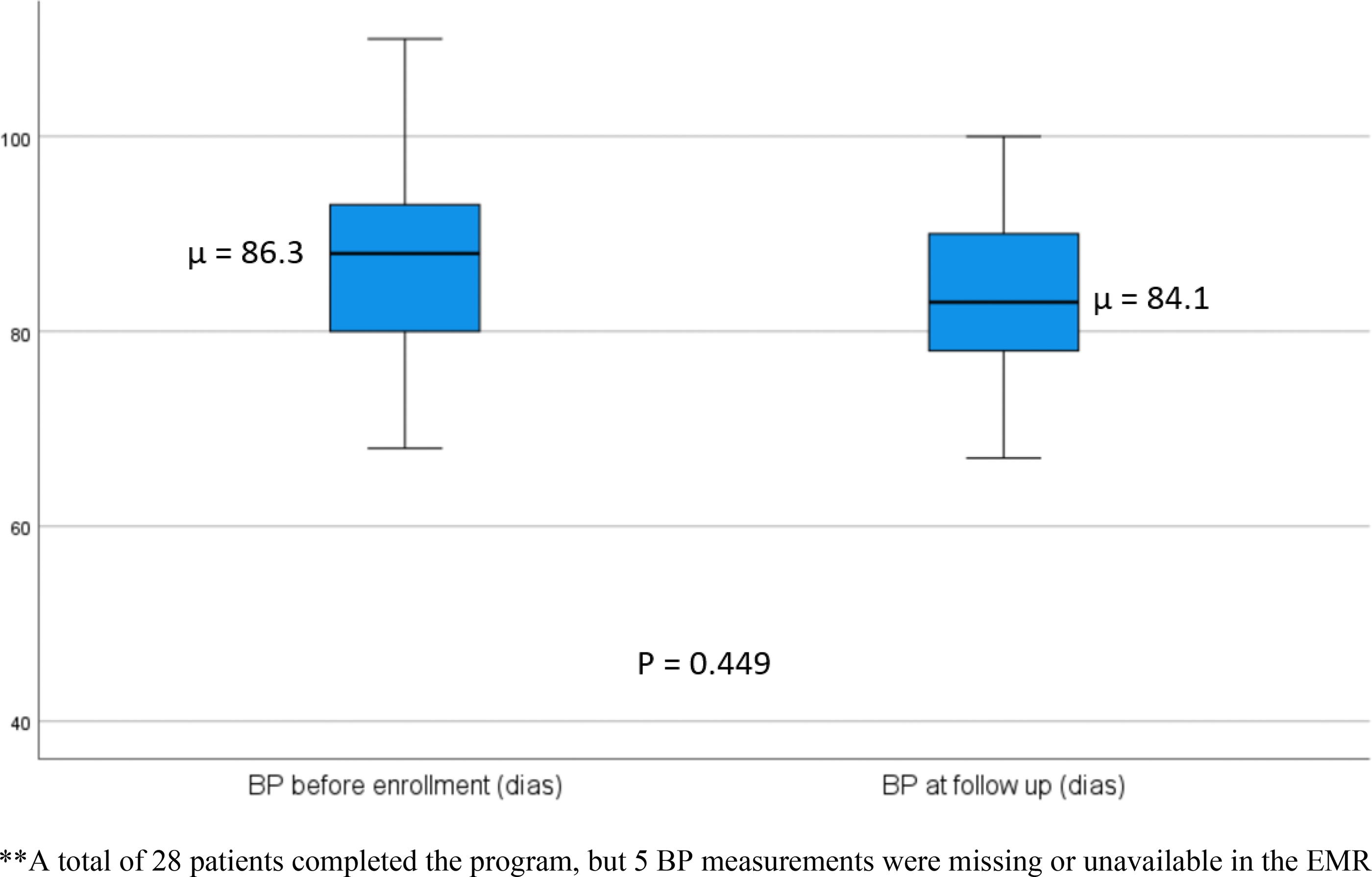
Diastolic Blood Pressure (mmHg) before and after intervention (n = 23**).
Discussion
Participants who completed the SMBP program had reduced systolic blood pressure and self-reported health distress. The statistically significant change in systolic, but not diastolic pressure is consistent with prior literature showing larger changes in systolic blood pressure than diastolic blood pressure in SMBP programs. 14 Participants who enrolled in the study but failed to complete the program did not show any change in systolic or diastolic blood pressure over a similar time period. These results are promising, particularly given the need for evidence-based interventions that are effective with Black patients, 6 and other underrepresented populations. 15,16 The authors’ findings suggest that a standardized interdisciplinary approach to hypertension management in primary care may improve clinical and patient-oriented outcomes in this patient population and emphasize the potential of multidisciplinary team-based approaches to support chronic disease management.
The study’s process measures also demonstrate the challenges of implementing an SMBP program in primary care. A large amount of effort was put into recruitment for the study, and other clinics may not have the capacity to do the same. The team struggled to recruit patients to participate in this clinical program and study. This project spanned 2019 to 2023, so it was impacted by the global COVID-19 pandemic, and the project had significant issues with staff turnover. Study personnel improved recruitment by sending MyChart messages and reaching out to patients with direct physician referrals. Based on the authors’ evaluation of patient recruitment approaches, electronic outreach was minimally effective but required little staff time. Direct referrals from primary care providers had the best results in terms of patient engagement and enrollment. Many participants were lost to follow-up, and there was a high rate of missed initial and follow-up appointments. The authors’ note that some of the patients who did not attend their initial appointment or who were unable to be reached after their initial appointment saw their primary care physician for their hypertension instead. This experience highlights the challenges associated with team-based care of chronic diseases in primary care: many patients have a challenging time establishing trusted relationships with other providers and many providers have a difficult time delegating work that traditionally is managed by physicians and advanced practice clinicians. The shifting of blood pressure management tasks from physicians to other team members remains a critical gap in the implementation of SMBP programs. 16
This study has several additional limitations. There are likely unmeasured confounders in our study; without a control group, individuals who completed the study may have differed in motivation or other characteristics than those who enrolled but did not complete, or who chose not to enroll. Furthermore, the authors note that the findings are based on small sample size, and thus, the generalizability of these results is limited. Because the authors could not collect responses to the health distress and self-efficacy measures from patients lost to follow-up, it is difficult to determine if secular trends in these responses may have impacted the change over time in participants. Finally, this project took place in a large, urban family medicine practice that included on-site pharmacists; findings may not be applicable to other practice settings.
The JFMA practice where this program was implemented may differ from most primary care settings due to its inclusion of learners, part-time faculty clinicians, and access to care team members who are not typically available in smaller practice locations. Although the practice had an interdisciplinary team, direct referrals from primary care clinicians were infrequent, and only a limited number of patients expressed interest in engaging with non-physician team members during separate visits. Barriers to realizing true team-based care may include a lack of clear roles, inadequate training in interprofessional collaboration, resistance among physicians to changing practice patterns, poor communication, and lack of shared incentives or goals. 17 Practice leaders must create structures that reward collaboration, minimize friction for patients, and harness the electronic health record and population health tools to facilitate SMBP and access to specialized team members to achieve the potential of true team-based primary care.
Implementation and next steps
Despite the limitations and challenges encountered, clinical protocols were adapted to improve blood pressure control, and we aim to standardize this method of hypertension management at JFMA. The authors are exploring an automatic referral process for hypertension management within the electronic health record that may lead to better control rates in the practice. Interdisciplinary teams, including pharmacists, are needed to successfully manage patients with chronic illnesses. Understanding how to integrate this work into primary care from both the provider's perspective and the patient's perspective is critical to increase efficiency and improve clinical outcomes. Understanding and sharing the impact of team-based care on patients’ perceptions of health and health distress may be one way to promote a team approach and increase participation.
Footnotes
Authors’ Contributions
The authors confirm their contribution to the article as follows: G.M. and A.C. conceived and designed the study. M.C. collected the data, analyzed and interpreted the results, contributed to writing the manuscript, and guided the students. S.O. and S.Q. aided with data collection and contributed to writing the manuscript. A.C. assisted with data analysis and interpretation. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
The Authors declare that there is no conflict of interest.
Funding Information
Funding for this evaluation was made possible in part by Cooperative Agreement # NU58DP006628 from the Centers for Disease Control and Prevention, U.S. Department of Health and Human Services (DHHS); and the Division of Chronic Disease and Injury Prevention at the Philadelphia Department of Public Health (PDPH). The views expressed in this article do not necessarily reflect the official policies of the DHHS or PDPH nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government or the City of Philadelphia.