
Abstract
High-need, high-cost (HNHC) adults require comprehensive strategies that address both clinical and social determinants of health (SDOH). This retrospective, propensity score—matched study (n = 526) evaluated a care model integrating monthly SDOH screenings, medication oversight, and real-time admission-discharge-transfer alerts in four urban primary care clinics. Compared to usual care, the intervention significantly reduced acute utilization within 60 days: emergency department (ED) visits decreased by 0.17 (P < 0.001) and hospital admissions declined by 0.12 (P < 0.001). Gross per-participant costs fell from $6,019 to $2,422 (a $3,597 reduction); after accounting for intervention expenses, net savings reached $3,222 (P < 0.001), yielding an estimated 6.9:1 return on investment. Patient-reported outcomes also demonstrated significant gains: EQ-5D-5L scores increased by 0.082 (P < 0.001) in the intervention cohort, exceeding the threshold for clinically meaningful change, while Net Promoter Scores rose by 8.8 points (P < 0.001). Subgroup analyses revealed slightly smaller quality-of-life gains among non-White cohorts, highlighting the need for culturally tailored approaches to advance equity. These findings align with prior Population Health Management research showing that integrated care models can reduce costs and enhance patient satisfaction. Overall, this multifaceted model effectively curbs avoidable ED visits and admissions, generates short-term cost savings, and boosts patient satisfaction—key outcomes under value-based care contracts. Future research should investigate longer-term outcomes and refine equity-focused strategies to ensure sustained and inclusive benefits.
Introduction
The social determinants of health imperative for High-Need, High-Cost populations
High-need, high-cost (HNHC) patients—those with multiple chronic conditions, unstable social settings, and psychosocial barriers—are among the most expensive yet underserved populations in healthcare. Their outcomes often remain suboptimal, demanding innovative, value-based care (VBC) strategies. Various models address social determinants of health (SDOH), but few generate both rapid cost savings and durable improvements in patient well-being. 4,5
Although prior interventions (e.g., community health worker programs, brief SDOH screenings) show modest success in reducing acute-care utilization, many rely on single-focus or short-term solutions that fail to capture patients’ full social, behavioral, and clinical needs. Fragmented efforts often overlook housing insecurity, limited health literacy, or other instabilities that trigger avoidable emergency department (ED) visits and admissions. This gap underscores the need for an integrated, multifaceted approach, rather than siloed solutions. 7,8
Population health management and value-based care: achieving near-term return on investment
Building on evidence that real-time data sharing, cross-sector partnerships, and team-based care can improve outcomes in HNHC populations, the authors developed an intervention combining monthly SDOH reassessments, active medication management, and real-time admission-discharge-transfer (ADT) alerts. 9 –11 By continuously monitoring social barriers and addressing medication-related risks, this model seeks to avert acute events and achieve near-term cost offsets—critical under risk-based contracts. The present study investigates whether a proactive, data-driven, patient-centered framework can reduce ED use and hospital admissions within 60 days while enhancing patient-reported outcomes. This dual focus on financial and experiential metrics addresses the “so what?” factor in population health: demonstrating a viable, scalable model advancing equity, patient satisfaction, and cost-effectiveness. 12
Integrating social, behavioral, and medication management
In parallel, prior research confirms HNHC patients—those with multiple chronic conditions, unstable social settings, and psychosocial barriers—disproportionately drive healthcare spending yet often face poorer outcomes. 1 –3 Fragmented care that overlooks key SDOH (transportation barriers, food insecurity) fuels reliance on EDs and avoidable admissions. 3 –5 These patterns inflate costs and undermine well-being, prompting preventive solutions. 5 –7
Although interventions (e.g., community health worker programs, integrated disease management) show promise, most hinge on short-term impacts—especially under value-based contracts seeking rapid cost offsets. 5,8 Although HNHC populations contend with entrenched social and economic risks that cannot be solved through singular or episodic clinical interventions. 3,9 Brief educational handouts or one-time referrals often prove insufficient when underlying instabilities—such as lack of reliable transportation or secure housing—remain unaddressed. 5,7 This perpetuates a costly cycle of ED utilization without true improvements in outcomes. 4,5 Recent policy discussions emphasize integrating SDOH screening with ongoing, tailored follow-up to reduce repeat ED visits and achieve measurable cost savings. 5,7 These efforts lay the groundwork for comprehensive interventions spanning social, behavioral, and clinical domains to yield near-term financial returns and longer-term patient benefits. 7 –9
Objectives, hypothesis, and the 60-day focus
Population health management (PHM), underpinned by the Chronic Care Model and social-ecological theories, identifies at-risk groups and coordinates multidisciplinary teams to avert costly acute events. 8 –10 Over the past decade, PHM approaches have evolved to incorporate real-time data sharing, cross-sector collaboration, and recognition of social as well as clinical drivers of health—transformations that parallel the rise of value-based care (VBC). 7,11 Under VBC, payers increasingly tie reimbursements to cost-effectiveness, patient experience, and equity, prompting demands for short-term return on investment (ROI)—often within 6 to 12 months—to validate SDOH interventions. 5,12 –14 Despite promising results from some SDOH-focused programs, few studies confirm immediate cost offsets among high-need, high-cost (HNHC) populations. 2,3 Gaps in follow-up and insufficient medication oversight can diminish impact, while equity concerns underscore the need for culturally responsive strategies. 13,15 Multi-component approaches integrating real-time admission-discharge-transfer alerts, medication checks, and ongoing SDOH assessments appear effective, but a uniform (“one-size-fits-all”) tactic may falter in diverse communities. 9,10,15 –17
Integrating social, behavioral, and medication management approaches
Many interventions prioritize SDOH-focused outreach (screenings, referrals) or medication adherence alone, 13,15,18 but a model combining monthly SDOH checks, medication management, and rapid post-encounter follow-up may better curb avoidable ED visits and admissions. 7, 12 Overlapping social and behavioral barriers—such as underdiagnosed depression or limited health literacy—can disrupt chronic disease control and trigger frequent ED use. 5,15,18 By integrating pharmacy data (e.g., refill records), real-time ADT alerts, and monthly SDOH assessments, care managers can address emergent issues before they escalate. 7,16,19 Early demonstrations suggest this integrated approach fosters trust, reduces fragmentation, and produces short-term cost benefits. 11,19,20
Still, siloed workflows remain common, dividing social workers, pharmacists, primary care teams, and community entities with minimal coordination. 15,16,20 This fragmentation delays help until crises arise, undermining proactive care. 5,15,17 For HNHC patients frequently returning to EDs, structured monthly outreach, medication pickup verification, and real-time ADT alerts can address social risks earlier. 7 Preliminary evidence shows cost benefits, though rigorous links to short-term ROI and patient-reported outcomes remain limited. 2,8
Study objectives, hypothesis, and 60-day focus
Building on these insights, a proactive, SDOH-focused care management model was deployed in four community-integrated primary care clinics serving HNHC populations. 15 –17 Unlike narrower interventions, it merges monthly SDOH reassessments, real-time ADT alerts, and consistent medication oversight to ensure secure prescriptions, adherence to treatment, and timely social support. A retrospective, propensity score—matched cohort study examined whether this multifaceted method can (1) reduce ED visits, hospital admissions, and costs; (2) improve patient-reported outcomes (health-related quality of life, satisfaction); and (3) identify subgroup variations pertinent to equity. 18
In line with policy imperatives 5,11,16,21 and frameworks highlighting synergy among social, behavioral, and clinical supports, the authors hypothesized this integrated intervention would significantly cut acute utilization, yield a robust ROI, and boost patient satisfaction and quality of life within 60 days. A 60-day window aligns with short-term contract benchmarks in risk-based agreements, emphasizing immediate cost offsets essential for budget planning. 9,14,22 Demonstrating near-term financial and patient-centered outcomes is increasingly critical to sustain SDOH-based models under value-based care. 11,12,16,17,27 By uniting social and clinical interventions in a single, data-driven system, this approach aims to deliver tangible economic returns and improved experiences for HNHC adults.
Literature Review
Population health management frameworks and the social-ecological perspective
Population health management (PHM) aims to move beyond episodic care by identifying high-need, high-cost (HNHC) individuals and tackling the complex interplay of medical, behavioral, and social factors. 1 –3 Grounded in the Chronic Care Model and social-ecological theories, PHM spans multiple levels—from individual and community to broader policy. 4 –6 In recent years, efforts to integrate upstream interventions targeting SDOH have helped avert expensive acute episodes. 7 –9 Tools like real-time data and predictive analytics can further reduce reliance on emergency departments and hospital admissions. 10,11 However, standardization and financing remain challenging, especially when seeking a demonstrable return on investment (ROI). 12,13
SDOH integration and team-based care in PHM interventions
Embedding SDOH screening into routine workflows is increasingly seen as key to advanced PHM. 14,15 Rather than focusing solely on clinical markers, many studies now endorse comprehensive screening for social risks such as food insecurity or housing instability. 3,16 This approach empowers multidisciplinary teams—from primary care providers to social workers—to implement more effective interventions. 17,18 Team-based models distribute tasks, improve medication adherence, and sustain care continuity, often reducing ED utilization. 17 –20 Research also highlights medication management (e.g., refills, patient education) as crucial for SDOH-focused initiatives. 13,16,20 Monthly medication checks have reduced readmissions and boosted satisfaction, aligning with the Quintuple Aim. 21,22
Health policy initiatives, value-based payment models, and equity alignment
Policymakers and payers, confronted by rising healthcare costs and persistent equity gaps, have embraced value-based care (VBC) models that reward improved outcomes and lower spending. 6,14,23 Programs such as the Accountable Health Communities (AHC) initiative, Medicaid Section 1115 waivers, and new Medicare Advantage benefits encourage social care integration through updated payment structures and performance benchmarks. 6,24,25 These reforms support SDOH-based approaches as both cost-effective and equitable. 11,19 –25 Yet converting policy ambitions into effective interventions remains difficult. 10,15,24 Even with new funding streams, demonstrating robust cost savings and equitable outcomes across race, ethnicity, and insurance tiers is still a challenge. 13,16 –26 Researchers warn that failing to account for cultural nuances can deepen disparities. 16,20 –27 Consequently, policymakers increasingly seek programs that curb costs, enhance patient experience, and proactively address inequity. 10,18 –27
Economic considerations, sustainability, and scaling in PHM
A pivotal barrier in PHM is demonstrating timely ROI to preserve and grow SDOH-based models. 4,12,15 Although certain large-scale demonstrations show ED and inpatient reductions leading to net savings. 1 –22,28 Direct comparisons are often hampered by varied designs, participant attributes, and outcome definitions. 11,14,17,22 Emerging consensus indicates that advanced analytics (machine learning, social risk stratification) and cross-sector data (housing agencies, food banks, pharmacy records) can help optimize resource allocation while quantifying cost returns more accurately. 19,22,29 Yet, technology alone does not guarantee sustainability—multidisciplinary engagement, dedicated funding, and tailored incentives are all crucial to align provider goals with patient-centered PHM. 6,14,17,19
Gaps in the literature and the present study
Although numerous SDOH-focused interventions reduce utilization and enhance satisfaction, 5,8 –11 challenges remain. First, much of the literature highlights single components—like food insecurity screening or medication therapy management—rather than cohesive monthly outreach that also uses real-time ADT alerts and extensive pharmacy coordination. 13,16,20 Second, while ED visit declines are commonly reported, few studies tie these outcomes explicitly to meaningful cost savings and robust ROI within a short timeframe—an increasingly urgent requirement in risk-based contracts. 10,15,18 Third, despite efforts to improve equity, certain racial or insurance-based subgroups still experience fewer benefits. 26,27,29
Methods
Study design and setting
A retrospective, propensity score —matched cohort study was conducted to assess whether a proactive, SDOH–oriented care management model could reduce utilization, lower costs, and improve patient-reported outcomes (PROs) among high-need, high-cost (HNHC) adults. The intervention was implemented in four community-integrated primary care clinics located in an urban region of the southwestern United States. 1,2 These clinics primarily serve racially and socioeconomically diverse patients with complex needs, aligning with PHM goals of reducing fragmented care.3
Rationale for a 60-day follow-up window
The 60-day observation period was chosen to align with short-term contract benchmarks commonly employed in risk-based payment arrangements. 4,5 Many payers and policymakers require demonstrated cost offsets and outcome improvements within a few months, making the two-month horizon especially pertinent. By focusing on near-term metrics, the authors aimed to capture the immediate financial and clinical impact of the intervention—information increasingly vital for budgetary cycles and value-based care (VBC) negotiations. 5,6
Intervention versus comparison treatment
Participants in the intervention arm received a structured, four-part care management model:
Patients in the comparison group continued to receive usual care, involving standard office visits and ad hoc clinician-led interventions without systematic monthly SDOH checks. 6,13 At the index date, participants in the intervention arm had been enrolled in the care management program for an average of 1.7 months, with a range of 17 days to 3 months. This design allowed us to assess whether the multifaceted SDOH-focused model produced measurable differences in costs, utilization, and PROs relative to usual care.
Participants and eligibility criteria
We included adults (≥18 years) flagged as HNHC by ≥2 hospital admissions or ≥4 ED visits in a prior 6-month interval, consistent with established PHM thresholds. 5 To track changes over time, participants required baseline PRO data (EQ-5D-5L and Net Promoter Score [NPS]) recorded within 60 days pre-index. 11 Patients under legal guardianship or with severe mental illness or developmental disabilities needing specialized care pathways were excluded, aiming for a relatively homogeneous HNHC sample. 15 After eligibility screening, 526 individuals (263 intervention, 263 comparison) remained post–1:1 nearest-neighbor propensity score matching (caliper = 0.20).
Power and sample size considerations
Although this was a retrospective, propensity score—matched study, the authors conducted a post hoc power analysis to assess whether the final analytic sample (n = 526; n = 263 per group) sufficed to detect observed differences in ED utilization. Drawing on existing literature 1,3 and the documented 0.17 decrease in ED visits among the intervention cohort (P < 0.001), the authors assumed a moderate effect size (Cohen’s d ≈ 0.35–0.50). At two-sided α = 0.05 and 80% power, ∼400–600 participants were needed to detect such differences. Because the authors enrolled 263 patients in each arm, the study exceeded that threshold, conferring adequate power to detect moderate utilization changes.
Data sources and management
All data sources were linked via unique patient identifiers and de-identified before analyses:
This integrated dataset supported tracking of utilization changes (Table 1) and patient-level measures (Figs. 1–3).
Baseline Characteristics of Intervention and Comparison Groups After Propensity Score Matching
SMD <0.1 indicates acceptable balance. Chronic Disease Count† is an aggregated measure of conditions such as diabetes, heart disease, COPD, and depression (Centers for Disease Control and Prevention, 2022).
*EQ-5D-5L, EuroQol 5-Dimension 5-Level measure of health-related quality of life; **NPS, Net Promoter Score (measure of patient satisfaction); SMD, Standardized Mean Difference.
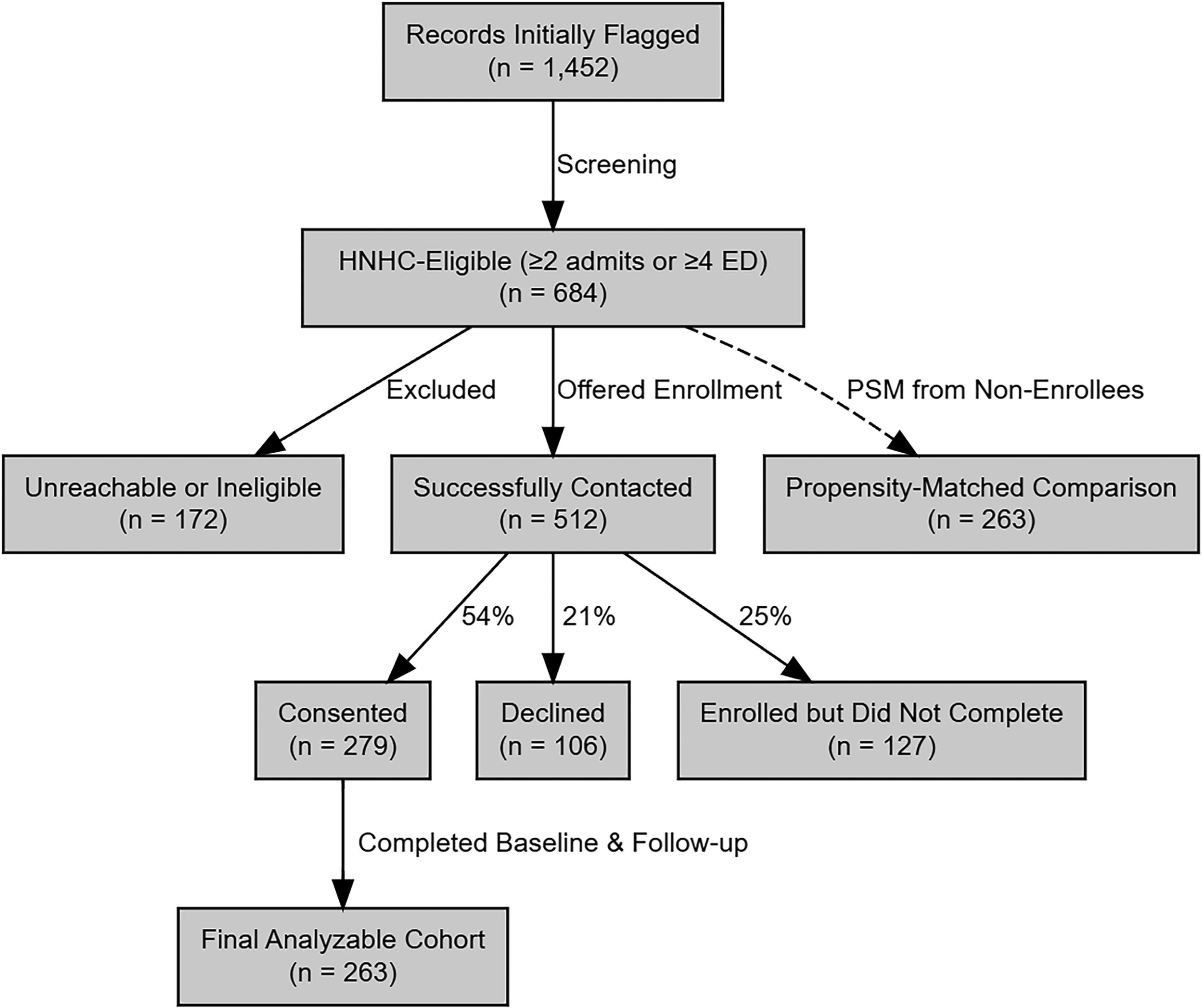
Enrollment and propensity score—matched comparison flow diagram.
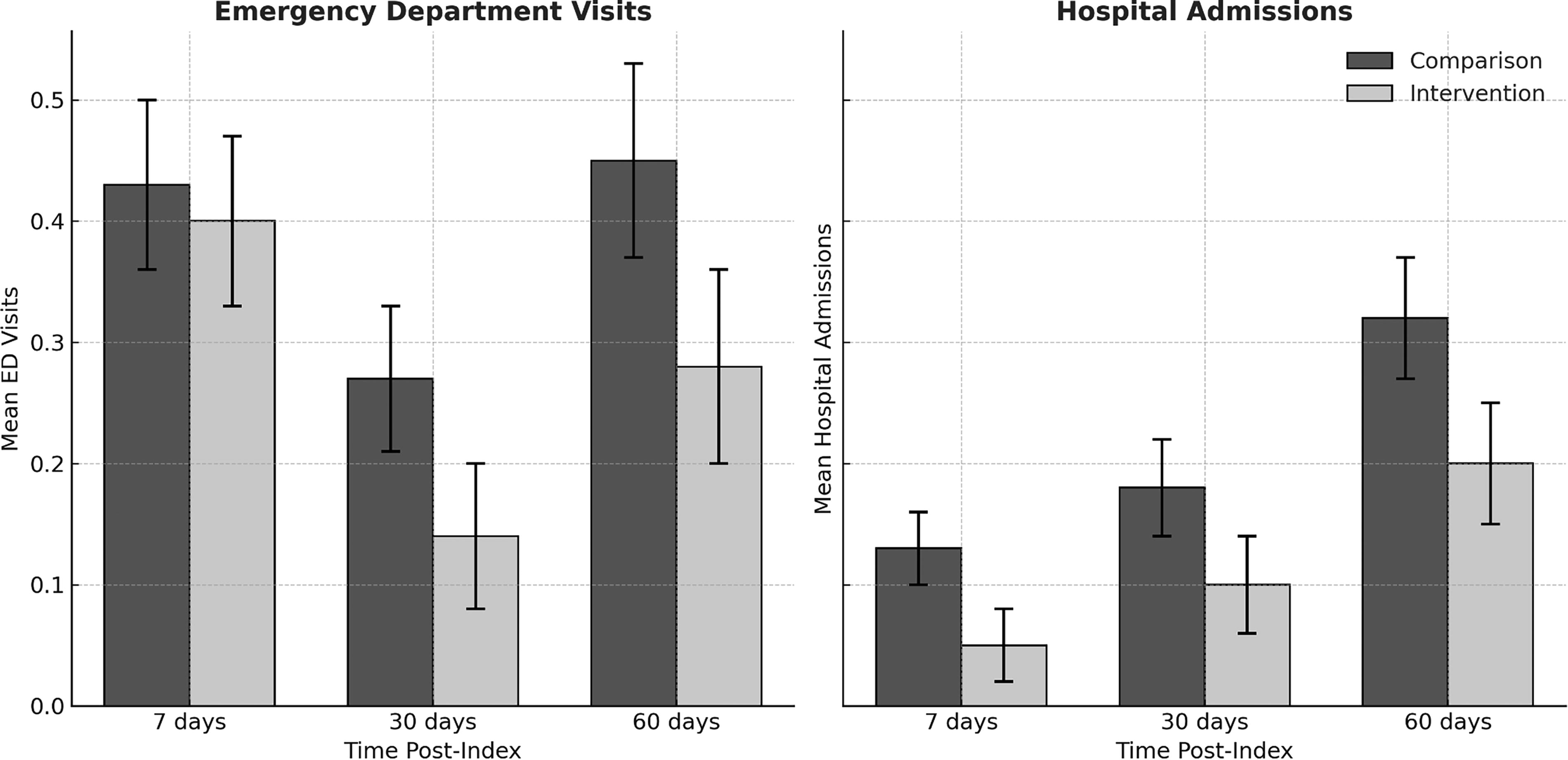
Changes in emergency department visits and hospital admissions over time.
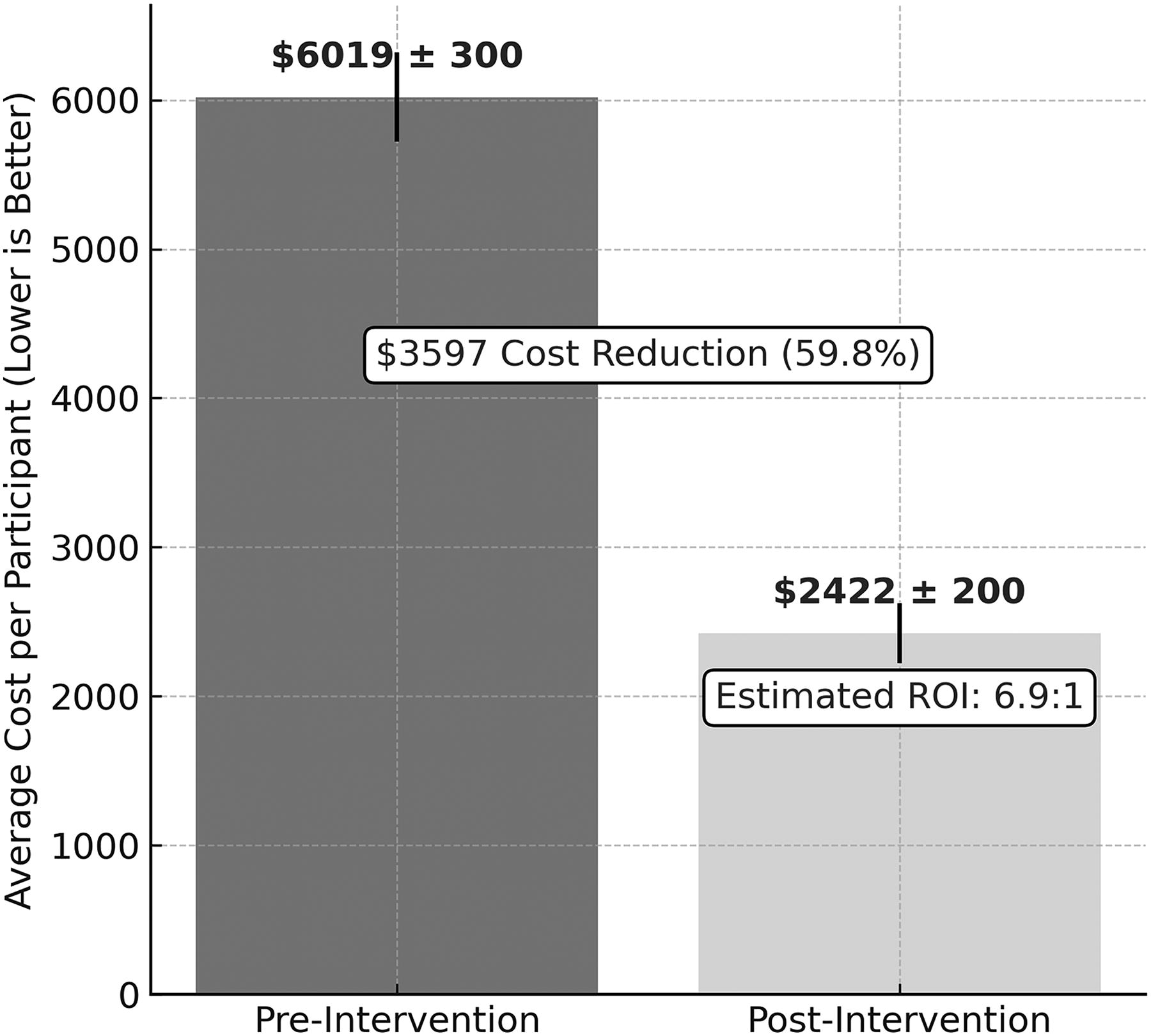
Cost reduction over 60 days and estimated return on investment (ROI).
Operational feasibility and staffing
The intervention relied on care managers, each overseeing approximately 130 patients. Their responsibilities included conducting monthly SDOH reassessments, performing medication checks, and responding to real-time ADT notifications. Care managers also consulted with internal providers and external community-based organizations (e.g., social workers or pharmacists) to address culturally tailored or complex needs. 3,7 Although many core activities—such as screenings and outreach—were integrated into existing staffing structures, the increased workload necessitated additional hiring. Specifically, the organization recruited one supervisory care manager (annual salary $106,842) and two additional care managers (annual salary $70,000 each), totaling $246,842 in new salary costs. Most administrative tasks were absorbed by existing personnel. Consequently, the principal new expenses were these staffing costs and the required health information exchange subscriptions, aligning with typical population health management (PHM) investments. 3,13
Return on investment
Net savings were derived from reductions in emergency department (ED) visits and hospital admissions, averaging $3,222 per participant over 60 days. With 526 participants enrolled, the aggregate net savings totaled approximately $1,694,172. The intervention’s total new staffing cost, $246,842, was distributed across these 526 participants. Accordingly, the ROI was calculated as net savings divided by total intervention costs, yielding $1,694,172 ÷ $246,842 (6.87:1). This indicates that every dollar invested in the supervisory and additional care manager salaries returned $6.87 in avoided acute-care costs within two months. These findings underscore the near-term cost-effectiveness of integrating monthly SDOH screenings, medication oversight, and real-time ADT alerts for high-need, high-cost populations in value-based care environments.
Measures
Net Promoter Score (NPS)—assessing patient satisfaction and willingness to recommend services, with an 8–9 point increase deemed notable in healthcare. 19
Costing methods
We adhered to fixed-unit cost conventions widely used in PHM research, allowing straightforward comparisons across multiple settings. 20,21 Although real-world billing may differ by hospital or payer mix, ±10% cost sensitivity checks revealed no meaningful deviations in short-term cost differentials or ROI estimates. These findings align with earlier studies attributing cost changes primarily to reductions in ED visits and hospital admissions, rather than local fee variation.30, 35
Missing data and sensitivity analyses
We addressed missing data (e.g., incomplete PROs, partial utilization logs) using multiple imputation with fully conditional specification, validated by pattern-mixture modeling. 11,16 No material differences emerged between complete-case and imputed analyses, affirming the robustness of results. All participants included in the final matched sample consistently displayed the core outcome variables at baseline and at least one follow-up point. 6,15
Statistical analysis
Ethical considerations
University Institutional Review Board (IRB) approval was obtained, and the study adhered to the Declaration of Helsinki guidelines. 27 Data were fully de-identified, enabling a waiver of informed consent. Analytic and privacy procedures followed institutional and PHM best-practice guidelines, ensuring confidentiality and compliance with relevant regulations. 28
Results
Participant characteristics and baseline balance
A total of 1,452 patient records were initially screened. Following eligibility checks and propensity score matching (1:1 nearest-neighbor, caliper = 0.20), 526 patients formed the final sample (263 in the intervention group, 263 in the comparison group). Key demographic, clinical, and utilization characteristics are summarized (Table 1). Standardized mean differences below 0.10 for age, gender, race/ethnicity, insurance type, prior ED visits, and hospital admissions indicate successful matching, with no significant between-group discrepancies. 29,30 Baseline patient-reported outcomes (EQ-5D-5L, NPS) also showed no significant differences, confirming a well-balanced starting point for evaluating the intervention’s impact.
ED utilization over time
Temporal trends in ED usage (Fig. 1) reveal a more pronounced decline for the intervention cohort compared to the comparison group over 60 days. ED visits dropped by 0.13 at 30 days (P < 0.001) and 0.17 at 60 days (P < 0.001) in the intervention arm (Table 2), whereas the comparison arm experienced smaller or nonsignificant reductions. These data suggest that monthly SDOH checks, real-time ADT alerts, and medication oversight jointly curtailed avoidable acute care encounters. 31,32 Table 3. displays the baseline-adjusted outcomes for 60 days, including mean rates of ED visits and hospital admissions, total cost differences, and effect sizes. These data summarize both the magnitude and significance of the observed changes relative to the matched comparison group.
Changes in Utilization and Costs at 7, 30, and 60 Days Post-Index
Costs were estimated using standardized unit costs frequently applied in PHM economic evaluations, set at $500 per ED visit and $10,000 per hospital admission. 23 The ROI calculation is based on comparing cost savings to intervention expenses over the 60-day post-index period. A P value <0.05 indicates statistical significance.
ED, Emergency Department; ROI, Return on Investment.
Clinical and Utilization Outcomes After Propensity Score Matching at 60 Days, With Effect Sizes and Adjusted Analyses
Sensitivity analyses included (1) regression models without matching (ordinary least squares or logistic), (2) multiple imputation for missing EQ-5D-5L/NPS data, and (3) ±10% variations in cost estimates. None altered the direction or statistical significance of the main findings.
Confidence intervals or effect-size estimates derived from alternative model approaches or cost definitions.
CI, confidence interval; d, Cohen d; ED, emergency department; NPS, Net Promoter Score; OR, odds ratio; SD, standard deviation; USD, US dollars.
Hospital admissions and cost outcomes
Hospital admission rates also decreased more substantially in the intervention group, with between-group differences of 0.08 at 30 days and 0.12 at 60 days (P < 0.001 for both; Table 2). Concomitantly, the intervention cohort’s per-participant costs fell from $6,019 pre-enrollment to $2,422 post-enrollment, a net decrease of $3,222 (P < 0.001; Fig. 2); this highlights the estimated 6.9:1 return on investment (ROI), underscoring the near-term economic viability of integrating SDOH outreach with medication oversight. 33 Sensitivity analyses adjusting ED and admission costs ±10% did not meaningfully alter these financial conclusions, indicating that the results are robust to modest cost variations. 35
Patient-reported outcomes
EQ-5D-5L (Health-related quality of life)
Across the entire sample (n = 526), EQ-5D-5L scores increased from a pre-intervention mean of 0.700 (SD = 0.15) to 0.765 (SD = 0.14), indicating an overall gain of +0.065 (t(525) = 12.95, P < 0.001). This change corresponded to a Cohen’s d of 0.85, signifying a large effect size in favor of the intervention. In group-specific analyses, the enrolled (intervention) group improved from 0.720 to 0.802 (t(525) = −14.88, P < 0.001), whereas the comparison group’s increase (0.604 to 0.612) was nonsignificant (t(262) = −1.88, P = 0.069). Subgroup analyses revealed that middle-aged adults (36–50) with private insurance achieved the largest EQ-5D-5L gain of +0.137 (95% CI [0.115, 0.159]). 34 These findings suggest that combining monthly SDOH assessments, medication checks, and real-time ADT alerts can drive clinically meaningful short-term improvements in health-related quality of life. 29,30
NPS (patient satisfaction)
For NPS, participants overall exhibited a mean increase from 17.78 (SD = 7.6) to 22.19 (SD = 8.5), a difference of +4.41 [t(525) = 16.75, P < 0.001], equivalent to Cohen’s d = 1.05, denoting a large effect size. Group-specific data indicated that the enrolled arm improved from 19.49 to 28.22 [t(525) = −43.12, P < 0.001], while the comparison group’s change (16.26 to 15.55) was not statistically significant [t(262) = 1.71, P = 0.091]. Subgroup analyses identified younger adults (18–35) with private insurance as having the most substantial NPS gain of +9.56 points. These robust effect sizes underscore that participants experienced not only lower acute utilization (as shown in Table 2) but also higher satisfaction—a critical dimension under value-based care contracts that emphasize patient experience. 31
Subgroup analyses and equity considerations
Analyses by race/ethnicity and insurance status revealed slight variations in effect sizes. Medicare/Medicaid beneficiaries exhibited marginally larger declines in ED use than those with commercial/private insurance (P = 0.026). Although most subgroups benefited, some non-White cohorts exhibited smaller EQ-5D-5L gains, suggesting potential areas for culturally or linguistically tailored interventions. 7 These patterns underscore the importance of ongoing refinements to address disparate outcomes across demographic strata. A separate article is currently under development to explore these subgroup disparities more thoroughly.
Sensitivity analyses and mechanistic insights
Multiple imputation with fully conditional specification confirmed that missing data (e.g., partial monthly SDOH assessments or incomplete baseline PROs) did not bias core findings. Additional pattern-mixture checks showed minimal deviation in cost or utilization estimates. Pharmacy logs further indicated that ∼79% of intervention participants filled at least one new prescription within 7 days of issuance, vs. ∼54% in the comparison group—pointing to improved medication adherence as a likely mechanism behind reduced acute care and heightened patient experience. 35
Discussion
Summary of key findings
These results underscore a critical truth in value-based care: cost and quality goals need not be at odds, especially when multidisciplinary teams unite social, behavioral, and clinical insights to address the root causes of frequent acute utilization. In this retrospective, propensity score — matched study, the authors evaluated a multifaceted, SDOH–centered care management intervention among high-need, high-cost (HNHC) adults. Compared to usual care, the intervention yielded significantly fewer emergency department (ED) visits and hospital admissions by 30 and 60 days, translating into substantial cost reductions and an estimated 6.9:1 return on investment (ROI). Crucially, these financial advantages did not detract from patient experience: over half of the intervention cohort demonstrated clinically meaningful improvements in EQ-5D-5L (≥0.07 gain), and Net Promoter Score (NPS) rose by an average of +8.8 points, underscoring the compatibility of short-term economic gains with enhanced patient-reported outcomes. 36
Mechanisms of action and synergy
Several components likely drove this swift impact. Monthly SDOH reassessments identified evolving social risks—such as housing instability, transportation deficits, or food insecurity—before they escalated. Medication management steps, including pharmacy log checks and medication adherence coaching, helped limit chronic-condition flare-ups that commonly trigger ED visits. Real-time ADT alerts further allowed care managers to rapidly intervene post-discharge, coordinating follow-up appointments and closing care gaps quickly. By fusing these elements, the model minimized fragmentation across social, behavioral, and clinical domains, potentially explaining the relatively robust near-term improvements in costs and patient-reported quality of life. 37
Comparison to previous literature
While past SDOH-based interventions have indicated reduced ED usage or inpatient stays, many report only modest economic benefits within short windows. Single-component pilots (e.g., screening only for food insecurity) may not sufficiently mitigate complex social risks. In contrast, this integrated approach—incorporating monthly screenings, medication oversight, and real-time follow-up—may yield more pronounced early savings by addressing overlapping social and clinical barriers simultaneously. Still, differing patient demographics, regional resources, and data infrastructures can affect generalizability. 38
Policy and practice implications
Strengthen infrastructure for real-time data sharing
Under emerging value-based care (VBC) models, demonstrating short-term cost savings and improved outcomes is pivotal, particularly for high-need, high-cost populations incurring considerable acute-care expenses. 39 As findings illustrate, ADT alerts constitute a crucial mechanism for early detection of clinical or social crises. By leveraging real-time health information exchange (HIE) platforms, care teams can intervene rapidly—scheduling follow-up appointments, arranging transportation, or addressing medication barriers before complications escalate. 13,20 However, this approach requires robust data infrastructures that support interoperability across multiple clinical settings and social service agencies. 14 In regions where digital connectivity remains limited, policymakers could incentivize development of shared data repositories and subsidize the necessary technology to ensure smaller or resource-constrained clinics can participate effectively. 12
Expand multidisciplinary care management teams
The success of any SDOH-focused intervention rests on the ability to coordinate social, clinical, and behavioral services seamlessly. 15 Drawing on the care model’s positive outcomes, the authors recommend forming multidisciplinary teams that include care managers, social workers, pharmacists, and behavioral health specialists. 9,16 This collective skillset allows practices to proactively address not only medical needs—such as medication reconciliation—but also psychosocial factors (e.g., housing, food insecurity) that can undermine adherence and drive ED visits. 7,10 The intervention’s team-based efforts to verify prescription pickups, conduct monthly SDOH reassessments, and facilitate culturally tailored care planning appear to have mitigated health risks and improved satisfaction. 39 Funding mechanisms under VBC contracts can reinforce this approach by rewarding collaboration across disciplines, thereby normalizing integrated workflows that reduce fragmentation and meet the complex needs of HNHC patients. 13
Equity considerations and potential adaptations
Notably, subgroup analyses revealed that some non-White groups experienced smaller gains in patient-reported quality of life compared to their White counterparts, pointing to opportunities for further refinement. While the intervention’s core elements—monthly SDOH reassessments, medication checks, and ADT-enabled follow-up—proved generally effective, future iterations may need to incorporate culturally tailored strategies and stronger community-level collaborations. Engaging these community partners more systematically may also improve resource alignment (e.g., connecting patients to housing support or nutrition services that resonate with cultural dietary patterns). By embedding such adaptations into the existing care management model, subsequent implementations may more effectively mitigate disparities, ensuring that the near-term economic and quality-of-life benefits extend equitably across diverse patient subgroups. 39
Limitations
Despite the application of propensity score matching and sensitivity analyses, this study faced certain constraints. Most notably, the 60-day observation window, while aligning with short-term value-based care benchmarks, may not capture longer-term intervention durability or fluctuations in outcomes. Future studies should extend follow-up to 6 or 12 months to assess whether the observed cost savings, reduced acute utilization, and improved patient-reported outcomes are sustained. Additionally, the reliance on standardized cost values and the reliance on real-time ADT alerts may limit generalizability to other settings lacking similar data infrastructure.
Future directions
Future efforts should extend the follow-up beyond 60 days to verify whether short-term economic and patient-reported gains are sustained. Longer-term studies (e.g., six or 12 months) could reveal whether re-hospitalization rates continue to drop or if intervention effects plateau. Moreover, randomized or stepped-wedge trial designs may address residual confounding and strengthen causal inferences. A separate article is under development, focusing on demographic and subgroup disparities to explore how race, ethnicity, and insurance status may modify the intervention’s effectiveness. By examining intersectional factors more deeply, subsequent adaptations can further address equity goals and reduce persistently observed disparities. Community-based partnerships—ranging from housing authorities to behavioral health agencies—could also refine the model’s capacity to address social risks early and prevent avoidable ED visits. 39
Conclusion
Our findings underscore that a proactive, SDOH-centered care model can deliver swift cost reductions and clinically meaningful patient-reported benefits, reshaping how high-need, high-cost populations are managed under value-based care. This synergy of social, behavioral, and clinical support underscores the feasibility of tackling complex patient barriers while delivering rapid ROI under value-based contracts. Nonetheless, future research should explore long-term impact, refine culturally tailored strategies, and address equity gaps to ensure all patient subgroups benefit equally from this model. 39 Our integrated intervention shows near-term ROI and improved patient experience; the synergy of SDOH screening, medication management, and real-time follow-up is crucial for achieving these outcomes. Future studies should focus on sustaining and scaling the model, with particular attention to cultural tailoring and equity.
Footnotes
Acknowledgment
The authors thank Mary Burleson and Nicole Roberts for their years of dedication and guidance.
Data Availability Statement
The data supporting the findings of this study are not publicly available due to privacy and institutional restrictions. De-identified data may be made available from the corresponding author upon reasonable request and contingent upon appropriate institutional approvals.
IRB Approval and Ethical Compliance
Authors’ Contributions
S.R.S.: Conceptualization (lead), methodology (lead), investigation (lead), formal analysis (lead), writing—original draft (lead), writing—review and editing (equal). L.M.: Conceptualization (supporting), methodology (supporting), formal analysis (equal), writing—review and editing (equal). N.A.: Formal analysis (equal), writing—review and editing (supporting).
Author Disclosure Statement
None of the authors hold any stocks or shares in organizations that may gain or lose financially from this work. They have not received consulting fees or other remuneration from entities that could benefit financially, and they have no patents or patent applications that may be affected by this publication. None of the authors have recent (within the past 5 years), current, or anticipated employment by an organization that may gain or lose financially from publication of this article. The authors do not have any personal relationships or circumstances that could inappropriately influence the research reported or the objectivity of the review of the article. There is no competition, previous disagreement, or bias in professional judgment that could compromise the integrity of this work. The authors report no conflicts of interest.
Funding Information
No funding was received from organizations that may gain or lose financially from publication of this article. There was no provision of salary, equipment, supplies, honoraria, reimbursement for attending symposia, or related expenses.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.