
Abstract
We tested a biofermented nutraceutical (FPP) that has been previously shown to positively modulate nitric oxide (NO). Forty-two healthy middle-aged subjects were given 3 grams of FPP three times a day for 6 weeks, and tests were repeated at 3 and 6 weeks; the control group was given a placebo. Flow-mediated dilation (FMD) was measured together with NO compounds (nitrogen oxides [NOx]: NO2 −+NO3 −) plasma levels and asymmetrical dimethylarginine (ADMA). In the interventional group, overall FMD significantly increased from 4.2% to 7.3% (p<0.05 vs. placebo). A significant increase in plasma NO and a decrease in ADMA were detected after consumption of FPP (p<0.01). Although larger studies are awaited, it appears that, at least in healthy individuals, such nutraceutical intervention by positively acting on significant cardiovascular parameters can be considered in the armamentarium of a proactive age-management strategy.
Introduction
The availability of ROS allows direct generation of cytotoxic radicals and NO inactivation. It has been shown that asymmetrical dimethylarginine (ADMA), an endogenous competitive inhibitor of NO synthase, is produced by methylation of arginine residues in intracellular proteins via arginine N-methyltransferase and causes endothelial dysfunction and atherosclerosis. 4 In this regard, it has been shown recently that daily ingestion of 10 grams of dried broccoli sprouts does not improve endothelial function in the presence of hypertension in humans. 5 Thus, this study was aimed to test whether the biofermented nutraceutical FPP (kindly donated by Osato Research Institute, Gifu, Japan), which has been previously shown to positively modulate NO, 6,7 could positively affect the above parameters in a healthy subject cohort.
Methods
Study design
All 42 participants were healthy middle-aged subjects (42–57 years old; male/female, 27/15) and not taking any drugs or supplements. Before entering the study, those with diabetes mellitus, hypercholesterolemia, or arterial hypertension based on international clinical guidelines were excluded from the study. The subjects maintained their usual diet and lifestyle, excluding all beverages and supplements that could influence vasomotor function except for water; they were provided caffeine-free tea beverages throughout the entire study. After the below-mentioned baseline measurements, subjects were given 3 grams of FPP three times a day for 6 weeks. Tests were repeated at 3 and 6 weeks. The placebo group was given the same quantity of flavored sugar.
Endothelial function assessment
Endothelial function was measured on each individual three times, at the start of treatment and twice during the 6 weeks of treatment with an interval of 2 weeks. Blood samples for erythrocyte content, lipids, blood glucose, and inflammation were taken at each visit to insure that the stimulus for measuring flow-mediated dilation (FMD) was as uniform as possible for each visit, considering that a considerable variation in blood viscosity could affect the shear stress of the vessel wall and thereby increase the measured FMD. The participants were instructed to arrive for the investigation after fasting for the last 12 hr, including medication. After arrival, they were placed in a supine position for at least 15 min before initiation of measurements in a quiet examination room with a temperature of about 22–C.
Measurements was performed on the brachial artery of the right upper arm 10 cm above the antecubital fossae with the pneumatic tourniquet placed distally to the ultrasound transducer immediately below the fossae at the area of greatest width of the forearm. The arterial diameter was measured at a fixed distance from an anatomical marker, such as a bifurcation, with ultrasonic calipers. The baseline diameter of the brachial artery was measured from two-dimensional ultrasound images using a high-frequency, 10- to 15-MHz vascular ultrasound transducer. Arterial flow velocity was measured by means of a pulsed Doppler signal at a 70° angle to the vessel, with the range gate in the center of the artery. Flow was determined by multiplying the arterial cross-sectional area (πr 2) by the Doppler flow velocity. The tourniquet was inflated to a pressure of 300 mmHg for a period of 4 min and 45 sec. During the last 15 sec of inflation and the initial 15 sec after deflation of the tourniquet, a Doppler spectroscopy of the flow through the brachial artery was recorded, to assess the flow increase through the brachial artery.
Cuff deflation induces a brief high-flow state through the brachial artery to accommodate the dilated resistance vessels. The resulting increase in shear stress causes the normal brachial artery to dilate. A pulsed Doppler signal was obtained within 15 sec of cuff release to calculate hyperemic velocity, and a longitudinal image of the artery was recorded from 20 sec to 2 min after cuff deflation. All images were synchronized with a continuous electrocardiogram (ECG) monitor and obtained at end diastole. FMD was measured as the percent change in brachial artery diameter from precuff inflation to 60-sec postcuff release. In addition to brachial diameter at 60 sec postcuff release, flow after cuff deflation within the initial 15 sec was used as an indicator of stimulus potency, hyperemic flow being the trigger for endothelial reactivity. To account for potential variability in stimulus strength, FMD was divided by flow at 15 sec. Measurement of FMD was given as the relative increase in diameter in percent compared to the baseline diameter of the brachial artery. The visits were made on the same time of the day to minimize diurnal variation.
Biochemical analyses
To assess the possible changes of shear stress during the study, blood samples were analyzed for the relative content of red blood cells and inflammatory markers (leukocytes and C-reactive protein [CRP]) because these factors are relevant contributors to the viscosity of the blood. Blood samples were collected from the subjects during the study and stored at −70°C until assayed. The plasma levels of the NO compounds (nitrogen oxides (NOx): NO2 −+NO3 −) and ADMA were measured using high-performance liquid chromatography methods described elsewhere. Lipid peroxides (malondialdehyde [MDA] and 4-hydroxynonenal [4HNE]) and soluble CD40 ligand [sCD40L]) were measured by enzyme-linked immunosorbent assay (ELISA). The biochemical measurements were duplicated and the averages used for the analysis.
Statistical analysis
Results were expressed as mean±standard deviation (SD). Statistical analysis was done by the SPSS statistical package (15.0 version). For continuous variables, the Kolmogorov–Smirnoff test was used to analyze normality in the distribution. Then, the Student two-sample t-test was used for variables that followed a normal distribution, and the Mann–Whitney test was used for the rest of variables. The results of each table were corrected for multiple comparisons by the use of Bonferroni correction.
Results
MDA, sCD40L, and human CRP were within normal limits in all subjects and were not changed by FPP consumption (data not shown). In the interventional group, overall FMD significantly increased from 4.2% to 7.3% (p<0.05 vs. placebo; Fig. 1). Few subjects (3 in placebo group and 5 in FPP group) had abnormal levels of 4HNE at baseline (outside the reference range given by the manufacturer), which did not change the overall significance. However, only those subjects in the FPP group normalized this value. A significant increase in plasma NO and a decrease in ADMA levels were detected after consumption of FPP (p<0.01).
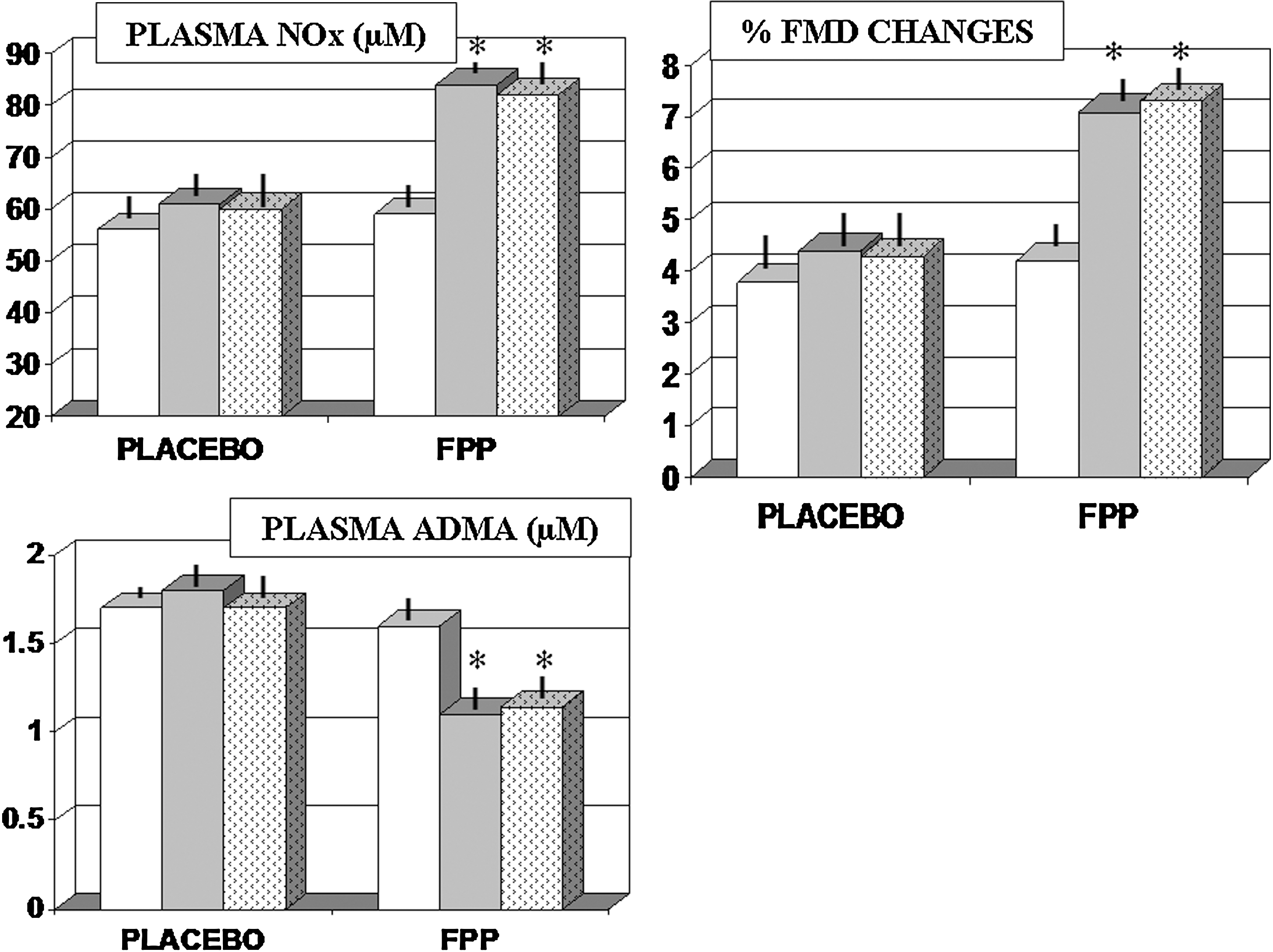
Effect of FPP supplementation on plasma levels of nitrogen oxide (NOx) and asymmetrical dimethylarginine (ADMA) and on percentage variations of flow-mediated dilation (FMD). (White bars) baseline values; (grey bars) 3 weeks observation; (dotted bars) 6 weeks observation. (*) p<0.01.
Conclusion
Endothelial function refers to arterial vasomotor responses mediated predominantly by the discharge of NO (vasodilating) and endothelin (vasoconstricting) from the vascular endothelium 8 and plays a relevant function in the pathogenesis of atherosclerosis, hypertension, cardiovascular disease, and diabetes. 9 We noted in our study that the baseline levels of NO and of ADMA were somewhat in the lower or higher range, respectively, of the normal levels expected for healthy subjects. 10,11 When analyzing the family history retrospectively, we found out that 9 subjects in the placebo group and 12 subjects in the interventional group had first-generation relatives with history of hypertension, diabetes, and/or metabolic syndrome. These data suggest that future studies should be directed to investigating the role of possible interfering genetic factors by a further screen for major susceptibility genomic polymorphisms. 12
Nonetheless, whatever the genomic or gender interplay, 13 endothelial dysfunction in resistance vessels, conduit arteries, or coronary arteries has increasingly been viewed as an independent surrogate marker of cardiovascular events, in addition to systemic vascular damage, 14,15 and its amelioration as an indicator of risk reduction. 16 In particular, given the observed basal decrease in NO levels and a decreased ratio of the vasodilator NO to the vasoconstrictor endothelin-1 as well as elevation of ADMA in cardiovascular patients, 17 –19 the present beneficial effect of FPP on the above biochemical parameters together with the functional FMD data are worth some consideration.
One limitation of this study is the single-blind protocol, although the person who evaluated the FMD and biochemical parameters had no information about the characteristics of the study participants. Moreover, we have to consider that circulating NOx levels are not an expression of NO pathway activation only because they are also derived from the catabolism of NO and its breakdown by oxidative stress. Whereas a recent study has proved that oral administration of arginine could improve the biochemical profile of myocardial infarction patients, 20 to the best of our knowledge, this is the first study showing that a nutraceutical is able to significantly and beneficially affect biochemical and functional markers of vascular health, and this may also be in conjunction with our prior research in healthy aged individuals. 21 Although our data cannot be directly translated into an integrative therapeutic approach in cardiovascular patients, they may be worth consideration in view of a wider healthy aging perspective.
Footnotes
Author Disclosure Statement
No competing financial interests exist.