
Abstract
Adverse clinical events (ACEs) are common in post–acute hospital care. We aimed at developing and validating a method, able to be administered in hospital wards, for identifying elderly patients at increased risk of ACEs after transferral to post–acute care (PAC) facilities. This was a prospective observational study, including 502 patients admitted to 19 PAC facilities in northern Italy from July 1st to August 14th, 2009. A standardized form was used to collect data. Variables showing stable association with ACEs in testing group were used to derive the score. The relative risk (RR) of developing ACEs according to the score was measured in the validation group. Age ≥87 years, delirium, pressure sore, indwelling bladder catheter, malnutrition, and acute infection on admission were identified as stable ACE predictors. A score of 1 was assigned to each predictor. Subjects were classified as having low (score=0), medium-low (score=1), medium-high (score=2–3), or high (score≥4) risk of ACEs. The RR of developing ≥1 ACE increased progressively from low (RR=1) to medium-low (RR=1.5, 95% confidence interval [CI] 1.1–1.9), medium-high (RR=1.6, 95% CI 1.3–2.1), and high (RR=1.8, 95% CI 1.4–2.3) risk score. The RR of being not discharged to home increased monotonically from 1.0 in low-risk to 2.7 in high-risk groups. In conclusion, this study proposes a method, able to be administered in hospital wards, for identifying patients at increased risk of ACEs after transferral to PAC. The score might also be used to identify people who will not return to home after PAC discharge.
Introduction
Within this context, a significant proportion of patients who need rehabilitation also require extra attention in terms of clinical and nursing care. Indeed, the interaction between age, disabilities, and co-morbidity frequently results in serious adverse clinical events (ACEs), such as infections, confusion, and others, 8 –10 which might delay length of rehabilitation or lead to poor outcomes. 5,8,9 However, although the identification and quantification of ACE risk factors has obvious clinical and economic implications, 10 to our knowledge there is no method to stratify patients admitted to PAC facilities according to their likelihood of ACEs. Furthermore, a scale to detect patients at risk is not yet available.
On the basis of these considerations, the aim of the present study was to develop and validate a score, able to be administered in hospital or immediately after transferral to PAC faciltities, for identifying subjects at increased risk of ACEs. Second, we aimed to assess whether this method can be used in PAC facilities to predict a patient's risk of being not discharged to home. In the authors' opinion, this tool might be especially useful for identifying patients who may require a prevalent rehabilitative intervention from those requiring a combination of rehabilitation and medical–nursing approaches.
Methods
Description of PAC settings and study subjects
This prospective study was carried out in Lombardia, Italy. This region has 10,021 beds devoted to the rehabilitation, with a ratio of 1.14 beds every 100 subjects aged 75 years or older. The beds are incorporated in a regional network service, with three different types of rehabilitation being provided: Intensive, geriatric, and long-term care rehabilitation. Intensive rehabilitation settings are similar to the U.S. inpatient rehabilitation facilities,
11
geriatric rehabilitation to skilled nursing facilities,
11,12
and long-term care settings to the long-term care nursing homes. All the PAC settings are licensed by the Regional Health Government to deliver a mix of rehabilitative and medical approaches to patients transferred from acute hospital wards. Furthermore, they are required to comply with both infrastructural (e.g., the size of the rooms) and professional (e.g., staffing levels) standards in accordance to the Regional policy (see
We contacted all of the PAC facilities sited in the Lombardia Region and affiliated with the Italian Society of Geriatrics and Gerontology (SIGG) and/or the Italian Society of Physical and Rehabilitation Medicine (SIMFER), and we checked their willingness to participate in this study. Nineteen out of 30 agreed, totaling 2,058 beds (65.5% of all total beds). Of these PAC facilties, 11 had beds for intensive, geriatric, and long-term care rehabilitation, 5 had beds only for intensive and geriatric rehabilitation, and 3 had beds only for geriatric and long-term care rehabilitation.
Prior to the start of the project, three introductory meetings were held to explain the aim of the study, the data collection form, and the methods to collect them. The senior physicians of each PAC participated in the meetings, which were led by two of us (G.B. and B.B.). A manual describing the procedures for data collection was provided to every facility. All physicians participating in the survey (a senior and a junior doctor for each PAC) were trained in data collection through simulation of clinical scenarios, completion of virtual data collection forms, and open discussion of the clinical cases. Patients admitted to the participating PAC facilities in the period from July 1st to August 14th, 2009, were eligible for the study if: (1) Aged 65 or older and (2) a written informed consent was obtained from the patient or relative/legal representative prior to study entry. The study was conducted according to the Declaration of Helsinki and the guidelines for Good Clinical Practice and was approved by the Ethics Committee of the Geriatric Research Group, Italy.
Description of the data collection form
The data collection form used in this study is reported in the Appendix 1. It consisted of general variables and a core set of dichotomous standardized indicators and validated assessment tools. The first section assessed demographics, general variables, and the Rehabilitation Impairment Categories, 12 –14 a classification system commonly used in rehabilitation to define the main impairment category on admission. The second section consisted of typical measures of multidimensional assessment, including the modified Rankin Scale (mRS), 15 the Barthel Index (BI), 16 and the Mini-Mental State Examination (MMSE). 17 The first two tools (i.e., mRS and BI) were used to assess, based on proxy reports, the functional status referenced to 1 month prior to admission for nonsurgical patients and prior to the acute event leading to surgery for surgical patients. The BI was also used to assess functional status on admission and at discharge. The MMSE was evaluated only on admission. The degree of walking dependence, using the BI walking subscore and the need of walking aids, 18,19 was assessed both on admission and at discharge.
The third section assessed the presence of organ dysfunction/failure in six body systems (chronic heart failure, chronic respiratory failure, hepatic failure, chronic renal failure, severe dementia, and the presence of active cancer), according to well-validated criteria. 20 –22 These variables were based on history taking and chart reviews and were referenced to 1 month before admission. For example, a patient was defined as having chronic heart failure if he/she was permanently in the III–IV class of the New York Heart Association 20 despite optimal treatment, and having chronic respiratory failure if he/she had chronic pulmonary disease with dyspnea at rest (class 3 or more at the GOLD classification) 21 or required oxygen supplementation. Dementia severity was defined with a cutoff of 3/5 using the Clinical Dementia Rating. 22 Active cancer was recorded as present if the patient had a malignant disease that required specific treatments (any type) in the last year. In this section, we also recorded a lack in the patient's social support (“social frailty”).
The fourth section assessed the presence on admission of 14 relevant clinical conditions. Impaired alertness was assessed using the Glasgow Coma Scale, 23 and delirium was assessed using the Diagnostic and Statistical Manual of Mental Disorders, 4th edition Text Revision. 24 According to previous studies, 7,25 medical instability was defined based on five vital signs (temperature≥37.8°C; heart rate [HR]≥100 bpm/min; systolic blood pressure ≤90 mmHg; respiratory rate ≥24/min; oxygen saturation rate <90% in patients not receiving mechanical ventilation or supplemental oxygen by face mask). Patients were considered medically unstable if at least one vital sign was altered in the 24 hr following PAC admission. Acute infection was defined according to the initial clinical examination and/or biochemical values from patient's blood samples; antibiotic treatment at discharge from acute hospital wards was accounted as an infection. Depression was assessed with the “Two-question case-finding instrument.” 26 The two questions were: “During the past month, have you often been bothered by feeling down, depressed, or hopeless?” and “During the past month, have you often been bothered by having little interest or pleasure in doing things?” If the patient responded “yes” to either question, the patient was considered depressed. Pain was recorded as present if the Numeric Rating Scale score was ≥6/10. 27 Dysphagia and malnutrition were defined based on the on admission clinical examination. Dysphagia was assessed using the 3-oz swallowing test, 28 and malnutrition with the body mass index (BMI) 29 and/or the Mini Nutritional Assessment. 30 Urinary incontinence was defined as the complaint of an involuntary leakage of urine, based on patient's history and/or caregiver's reports. 31 The presence of nasogastric/endogastric tubes, indwelling bladder catheter, pressure sore, tracheostomy, and/or central venous catheter was assessed directly by clinical examinations on admission.
The fifth section assessed the patient's level of dependence on admission in three motor tasks (control of the body trunk, transferring from bed to chair, and walking without aids), assigning a score of 1 if the patient required even a minimal aid to perform the task or a score of 0 if not. This section measured the level of patient's functional impairment and therefore the need of rehabilitation on admission.
The sixth section assessed the occurrence of four types of ACEs (urinary tract infections [UTI]; non–urinary tract infections [non-UTI]; other noninfectious adverse events such as cardiovascular, respiratory, or gastrointestinal; and falls). The importance of these ACEs has been highlighted in several previous studies on geriatric populations. 5,8,25,32,33 This section was used as a proxy of resource consumption, because each of these conditions obviously impacts on nursing and physician time expenditure in addition to daily routine. Each ACE was assessed according to validated criteria 34,35 and was defined as a change in clinical status that required a specific diagnostic workup and therapeutic initiatives. The seventh section assessed the destination at discharge, including return to home, transfer to other PAC facilities, nursing home, hospitalization, and death.
The interrater agreement between raters was assessed with the Cohen kappa (κ) coefficient, and was shown to be good (κ>0.71) for sections 3 and 4, and excellent (κ>0.81) for sections 5 and 6 of the standardized form.
Development and validation of the score
Complete clinical data were available for 502 patients. Their clinical characteristics are shown in supplementary files (Tables S1a and S1b) (Supplementary Data are available at
The initial sample was split into two independent subsamples with a jackknife method. The first sample was used to identify stable predictors of ACEs and to develop the score (testing group, n=252); the second sample was used to validate the score (validation group, n=250). Variables significantly associated with ACEs were identified with a stepwise regression model, entering the independent variables as follows: The first block included one dichotomous variable coding for elderly age, and the second block included the candidate clinical predictors (stepwise selection). The arithmatic sum of incident ACEs was entered as the dependent variable. Elderly age was defined as the 80th percentile of the age distribution, corresponding to a cutoff of 87 years. Those clinical variables that lacked variability in responses (i.e., variables in which more than 95% of subjects had the same score) were not included in the regression model. A bootstrap technique was used to draw n=10,000 random samples (with replacement) from the testing group and to perform a stepwise multiple regressions on each sample. The inclusion and exclusion p value thresholds were p=0.05 and p=0.10, respectively. The n=10,000 regression models generated, for each independent variable, a distribution of values (unstandardized β regression coefficients and p values), and quantitative indices of stability (frequency of inclusion in the model, number of sign changes of the β coefficients). The following criteria were then used to identify stable predictors: (1) Frequency of inclusion greater than 60%, and (2) no change in the sign of the β coefficients.
The variables obtained with this procedure were tested for reproducibility with a second model based on linear multiple regression and permutation testing. This model generated n=10,000 random subsamples (without replacement) of fixed size (66% of the testing group, i.e., n=168 subjects). For each subsample, all the candidate predictor variables were entered into the linear regression model (without stepwise selection), and ACEs were entered as the dependent variable. Significant predictors of ACEs were defined as those variables whose p values distribution showed a stable (i.e., p<0.10) association with the dependent variable.
The surviving clinical variables were then used to compute the ACE risk score. An integer weight was assigned to each predictor variable according to its relevance in the model (β regression coefficients), and the ACE risk score was computed by summing the weighted predictor factors. The relative risk (RR) of developing ACEs was computed in the testing and validation group as the rate for a given category of the score as compared with the reference category. To ease the interpretation of the results, we dichotomized the outcome (number of ACEs) at different levels of clinical severity: (1) No ACEs versus one or more ACEs; (2) no ACEs versus two or more ACEs; (3) no ACEs versus three or more ACEs. Finally, the RR of being discharged to other destinations than home was computed in the testing and validation groups.
Statistical analysis was performed using SPSS software (version 17.0). The association between clinical conditions and ACEs was assessed with tests for trend (general linear model for continuous variables and the Cochran–Armitage test for trend in proportions). The stepwise regression model with bootstrap sampling was implemented within SPSS. The linear regression model with permutation testing was implemented within R (version 2.12;
Results
Identification of stable predictors
Table 1 shows that the majority of the clinical variables on admission were significantly associated with the outcome ACEs (p<0.05 on test for trend). Six variables were excluded from the analysis due to the lack of variability in response: Chronic respiratory failure, chronic renal failure, chronic hepatic failure, presence of nasogastric/endogastric tubes, tracheostomy, and central venous catheter. The final model therefore included 19 variables (elderly age and 18 clinical variables). Six variables were identified as stable predictors of ACEs in the stepwise regression model: Acute infection, indwelling catheter, pressure sore, delirium, malnutrition, and age (Table 2, left panel). These variables were confirmed to be stable predictors of ACEs by the multiple regression method with permutation testing (Table 2, right panel).
Data denote mean (standard deviation [SD]) or frequency (%). P denotes significance on tests for linear trend (general linear model for continuous variables and the Cochran–Armitage test for trend in proportions).
Denotes significance on chi-squared test.
ACE, Adverse clinical event; MMSE, Mini-Mental State Examination; BI, Barthel Index; mRS, modified Rankin Scale; PAC, post–acute care; AHCPR, Agency for Health Care Policy and Research.
Indicates whether the variable is a stable predictor of ACEs, i.e., the variable is included in the stepwise model with a high frequency (>60%) and without changes in the beta coefficients sign. The B, CI (5%, 95%), and p values denote the median unstandardized regression coefficients, lower and upper confidence intervals, and significance values obtained from the n=10,000 stepwise regression analysis carried out on the testing group (n=252) with a bootstrap approach (left panel).
Stable predictors of ACEs are shown in bold. A linear regression model and permutation testing confirmed that these same variables were found to be stable (p<0.10) predictors of ACEs with a permutation testing approach and linear regression models (right panel).
CI, Confidence interval; ACE, adverse clinical event.
Development of the risk score
Since the predictor's β coefficients were very similar (Table 2), all of the predictor variables were assigned a weight of 1. The ACE risk score was built by summing the weighted predictor variables. For ease of clinical implementation, the risk score was coded into four categories: Low (0 risk factors on admission), medium-low (1 risk factor), medium-high (2 or 3 risk factors), and high (≥4 risk factors). The developed predictive score was significantly associated with the outcome (testing group, F=42.38, p<0.001 on test for trend; validation group, F=14.72, p<0.001; Fig. 1). The frequency of ACEs risk scores according to the outcome in the testing and validation group is shown in Table 3.
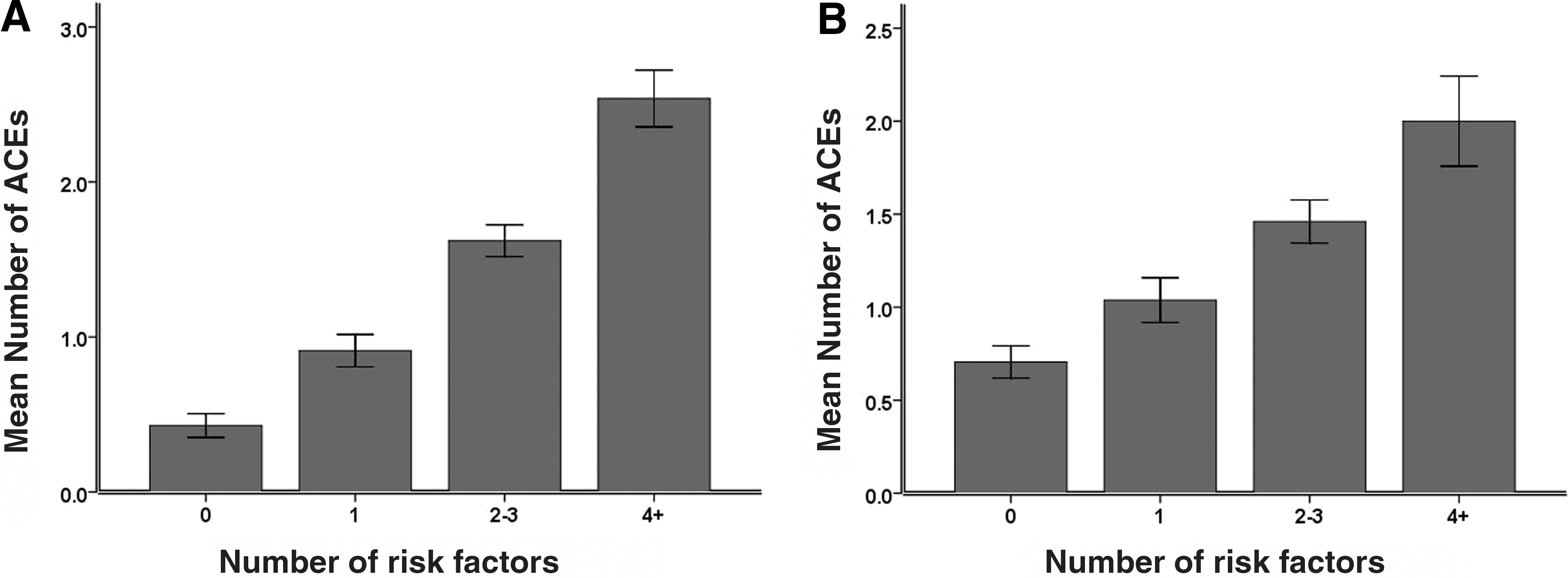
Histogram showing the mean (±standard error [SE]) number of adverse clinical events (ACEs) during post–acute care (PAC) stay according to the number of risk factors on admission in the testing (
The score was built by assigning a weight of 1 to each predictor variable (listed in bold in Table 3). Subjects with a score of 2 or 3 were assigned to “2–3” category, and subjects with 4 or more risk factors were assigned to “4+” category.
Values denote % frequency.
1+ denotes one or more ACEs.; 2+ denotes two or more ACEs.; 3+ denotes three of more ACEs.
ACE, Adverse clinical event.
Validation of the score
The relative risk (RR) of developing a given number of ACEs during rehabilitation increased monotonically with increasing risk score on admission (Table 4). In the validation group, the RR of developing one or more ACEs increased from 1.0 (low risk group) to 1.5 (95% confidence interval [CI], 1.1–1.9) in patients with a medium-low risk, to 1.6 (95% CI 1.3–2.1) in patients with a medium-high risk, to 1.8 (95% CI 1.4–2.3) in patients with an high risk score. The RR of developing two or more ACEs progressively increased from 1.0 (reference group) to 2.0 (95% CI 1.1–3.5), to 3.0 (95% CI 1.9–4.8), to 3.7 (95% CI 2.3–5.9) respectively. The relative risk to develop three or more ACEs increased from 1.0 to 2.0 (95% CI 0.6–6.5), to 4.7 (95% CI 2.0–10.9), to 7.7 (95% CI 3.4–17.5).
The table shows the relative risk values computed in the testing (left) and validation (right) groups.
Worked example: On the basis of this score, a 88-year-old person admitted to a PAC facility with an indwelling bladder catheter has a three-fold increased risk of having two or more adverse clinical events.
CI, Confidence interval; ACE, adverse clinical event.
The frequency of a discharge destination other than home according to the risk score is shown in Fig. 2. The RR of not being discharged to home increased from 1.0 (low risk group) to 1.2 (95% CI 0.7–1.9) in patients with a medium-low risk, to 2.1 (95% CI 1.5–3.0) in patients with a medium-high risk, to 2.7 (95% CI 1.8–3.9) in patients with a high risk score.

Histogram showing the frequency of discharge other than home in patients according to the number of risk factors on admission in the testing (
In the testing group, the RR values showed similar patterns, but values were obviously higher within the group used to develop the score (Table 4).
Discussion
This study proposes a practical score, able to be administered in hospital wards or immediately after transferral to PAC facilties, for identifying patients at increased risk of developing ACEs. The score was able to classify people developing ACEs in nearly two-thirds of all cases, with good discriminant capability either in developmental and prospective validation tests. The score was also able to prognosticate people who will not return to home after PAC discharge.
Incident ACEs are a major problem in post-hospital settings. In a landmark study on this topic, Bernardini and colleagues retrospectively evaluated the clinical charts of 106 patients admitted after neurological (mainly cerebrovascular) and osteoarticular (mainly hip fractures) problems, finding that 89% of all the patients experienced at least one ACE and a significant proportion of them (71%) two or more. 36 More recently, in a population of patients admitted to a geriatric rehabilitation, Mas demonstrated that ACEs can determine interruptions to the planned program in nearly one out of five admissions and that, after interruption, many patients cannot be discharged to home. 9 Other studies have demonstrated that mortality and hospital readmission rate among patients in rehabilitation and PAC settings has steadily increased in the recent decades, one of the main reasons being patient's clinical instability on admission. 1,37,38 Therefore, the ability to predict, at the time of hospital discharge, patients who will develop ACEs and who will have poor outcome is of crucial importance.
In this study we have identified six demographic and clinical variables independently associated with ACE occurrence (Table 5), and we used them to develop and validate a risk score: Age ≥87 years, indwelling bladder catheter, pressure sore, acute infection, delirium, and malnutrition. Possible explanations of these findings may be as follows. The observation that older age predicts ACE occurrence in PAC facilities is consistent with other studies 7,12 and with the view that the oldest old may be more vulnerable to clinical problems. 39 Other risk factors, such as indwelling bladder catheter and pressure sore, may be surrogate markers of impaired mobility or might reflect inadequate medical practice at hospital and iatrogenic complications. 37,40,41 Inadequate or inefficient management of patients in acute hospital wards, as well as patient's frailty, might be related to the presence of acute infections on admission to PAC facilities. 41 Malnutrition and delirium (and again pressure sores) are typical geriatric syndromes 43 whose prevalence is high among older adults, although they are often unrecognized in hospital wards. 43,45 All of these variables have been previously associated with poor outcomes, including a high rate of functional decline, long length of stay, increased costs of medical care, and mortality. 41,44 –50
DSM, Diagnostic and Statistical Manual of Mental Disorders; PAC, post-acute care.
To date, however, the practical utility of these variables to predict ACEs and related outcomes is limited. Physicians know that patients with one or more of these conditions have an increased risk of subsequent adverse events, but generally they do not have the means to estimate the odds of these risks. Furthermore, even admitting that they become alerted in the face of these conditions, the accuracy of the estimated risk may be poor because not all of these variables have the same potential burden. For example, while delirium and pressure sores are known predictors of future adverse events, this is not for old age. Conversely, the score that we have constructed has allowed us to define four grades of risks of future ACEs and of not returning to home after a PAC stay. To our knowledge this is the first description of a score created with this specific aim. Of note, the score was developed from a number of variables potentially related to ACEs, including clinical, functional, cognitive, nutritional, and social parameters. Using complex statistical procedures, such as logistic regression models and permutation testing, we developed and validated a tool based on a few parameters that constitute the core background of the everyday clinical practice.
This tool may have several implications for the patients' management. The first implication is that physicians at the hospitals can more easily select the appropriate setting for patients after discharge. Establishing the right level of post–hospital care is difficult and the risk of transition of critical patients towards inappropriate settings (with subsequent rapid rehospitalization) is high. 11 Such a problem is strongly felt in Italy. 51
Our study proposes a score that could be used by physicians in the hospital to target patients for different types of care transition. According to this score, patients with a low risk might be discharged toward settings with a prevalent rehabilitative imprint. On the other hand, patients with high risk scores could be discharged toward long-term care clinical settings. Moreover, the tool may be used by trained nurses as well, because the predictors variables are simple to detect, have an intrinsic face validity, and do not require a particular expertise with the only exception possibly being the evaluation of delirium, which might require a preliminary rater's training. Overall, the completion of the score should not require more than 10 min. Furthermore, from a health-care perspective, this score could be helpful to promote benchmarking by comparing the complexity of patients discharged from various hospitals. The implementation of this tool on a national level would enable policymakers to improve care among PAC facilties and hospitals, through a reduction of hospitalization costs and the promotion of excellence, e.g., by penalizing facilities with poor patient outcomes despite favorable risk profiles.
This study is not without limitations. Information regarding the time interval between admission to acute hospital ward and the transferral to the PAC facilities was not collected. Therefore, we cannot exclude that the wide variability of the data collected was influenced by nonclinical factors, such as the prompt availability of beds in the receiving (PAC) settings or of a prolonged length of stay in the sending hospitals. Another limitation is represented by the generalizability of the results. We acknowledge that the study was carried out on a proportion of PAC facilities drawn from a single region (Lombardia) in Italy, and thus our results cannot be generalized to the whole nation or other countries. Also, transition care policies differ across nations, as well as the epidemiology of disease burden. However, because the standard of care among PAC facilities in Lombardia is constantly monitored by Healthcare Government Agencies, which use data for financial purposes, it is very likely that the PAC facilties participating in our survey represent a pool of excellence in this context and that, therefore, the data collected depict a typical picture of patient's health conditions at discharge from hospitals.
Further studies are needed to validate the risk score in other clinical settings and countries. A third limitation is that we did not assess co-morbidity using a validated index, such as the Charlson Index or the Cumulative Illness rating Scale. 52,53 However, it is of interest that we assessed the presence of six severe organ dysfunctions and that none of them was included in the final score, suggesting that co-morbidity was not so determinant, in our population, to the development of ACEs. Finally, we recognize that the ideal setting to measure the score would be the acute hospital's wards, prior to transferral to the PAC facilities. On the one hand, however, practical difficulties limit the implementation of the protocol in acute hospital ward in Italy. On the other hand, the assessment of patients occurred invariably on admission to each PAC facility, i.e., only a few hours after acute hospital discharge. Therefore, we are confident that our score closely reflects the patients' clinical condition at the acute hospital's wards. Accordingly, we believe that our score may work well also in acute hospitals, provided that adequate training and resources are available in these settings.
In conclusion, the present study proposes a practical and simple score for identifying patients at increased risk for ACE and poor outcome at PAC facility discharge. This score may be used to target clinical interventions and to guide patterns of transition care from hospital to PAC facilities.
Footnotes
Acknowledgments
The authors are grateful to the Regional Healthcare Government, the Regional Sections of the Italian Society of Geriatrics and Gerontology (SIGG), and the Italian Society of Physical and Rehabilitation Medicine (SIMFER) for supporting this study.
The following persons participated in the present study: Steering Committee: G. Bellelli, Monza (chairman); B. Bernardini, Milan (co-chairman); M. Trabucchi, Roma; Database Production and Management: G. Bellelli, M. Pievani, GB. Frisoni, Department of Clinical and Preventive Medicine, University of Milano-Bicocca and Geriatric Clinic, S. Gerardo Hospital, Monza, Geriatric Research Group, Brescia; LENITEM-Laboratory of Epidemiology, Neuroimaging and Telemedicine, IRCCS Fatebenefratelli, Brescia.
Participants and centers: R. Bagarolo and E Segato, Istituto Don Orione Milano; R. Bagnoli and P. De Luca, Dipartimento Degenza Geriatrica Riabilitativa Pio Albergo Trivulzio, Milano; F Bombelli and L. Grossi, Fondazione Benefattori Cremaschi-Onlus, Crema; A. Pani, Azienda Speciale Comunale “Cremona Solidale”; C. Meinecke, Riabilitazione Specialistica e Generale-Geriatrica Azienda Ospedaliera di Cremona; M. Cottino Istituto Geriatrico Golgi, Abbiategrasso (MI); C. Sacchelli, Fondazione G Brunenghi Castelleone Cremona; P Crippa, Riabilitazione Neurogeriatrica Domus Salutis Brescia; G. Gelmini, Ospedale di Viadana (Mn); S. Gentile and D. Villani, Fondazione Sospiro, Sospiro (Cr); E. Facchi, Fondazione Ospedale Richiedei Gussago e Palazzolo (Bs); PG Bellani, Fondazione Vismara De Petri ONLUS, T. Suardi and G Barletta, ASP Istituto Piero Redaelli, Milano; A. Ponzoni, Istituto Don Orione, Bergamo; G Musolino, Fondazione Opera Pia Colleoni-Onlus, Asso (LO); R. Giani, Fondazione Gaetano e Piera Borghi, Brebbia (VA); R. Bottura and E. Muti, Fondazione Mons Mazzali, Mantova; A. Bianchetti, Dip Riabilitazione Istituto Clinico S. Anna, Brescia, G. Migliorati ASP Istituto Valsasino, S Colombano al Lambro; R. Giani and M. Bertoni, Fondazione Gaetano e Piera Borghi, Brebbia (Va); M. Mauri and G Tomasoni, Centro Girola Fondazione don Carlo Gnocchi ONLUS, Milano; A Frustaglia, E. Comi and C Rutili, Istituto Redaelli Vimodrone, (Mi).
The investigators had full access to the data and were responsible for the study protocol, progress of the study, analysis, reporting of the study, and the decision to publish.
Author contributions: Study conception and design
Author Disclosure Statement
No competing financial interests exist.
Appendix 1. Data Collection Form (see Methods for Further Details)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.