
Abstract
A short average telomere length is associated with low telomerase activity and certain degenerative diseases. Studies in animals and with human cells confirm a causal mechanism for cell or tissue dysfunction triggered by critically short telomeres, suggesting that telomerase activation may be an approach to health maintenance. Previously, we reported on positive immune remodeling in humans taking a commercial health maintenance program, PattonProtocol-1, composed of TA-65® (a natural product–derived telomerase activator) and other dietary supplements. In over a 5-year period and an estimated 7000 person-years of use, no adverse events or effects have been attributed to TA-65 by physicians licensed to sell the product. Here we report on changes in metabolic markers measured at baseline (n=97–107 subjects) and every 3–6 months (n=27–59 subjects) during the first 12 months of study. Rates of change per year from baseline determined by a multi-level model were −3.72 mg/dL for fasting glucose (p=0.02), −1.32 mIU/mL for insulin (p=0.01), −13.2 and −11.8 mg/dL for total cholesterol and low-density lipoprotein cholesterol (LDL-C) (p=0.002, p=0.002, respectively), −17.3 and −4.2 mmHg for systolic and diastolic blood pressure (p=0.007 and 0.001, respectively), and −3.6 μmole/L homocysteine (p=0.001). In a subset of individuals with bone mineral density (BMD) measured at baseline and 12 months, density increased 2.0% in the spine (p=0.003). We conclude that in addition to apparent positive immune remodeling, PattonProtocol-1 may improve markers of metabolic, bone, and cardiovascular health.
Introduction
Telomerase, the enzyme that synthesizes telomeric DNA, 17 can slow or even reverse telomere shortening in normal human cells in culture 18,19 and contribute to slowing or reversal of degenerative, age-related disease in animals. 14,20 –22 In almost all large-scale cross-sectional studies in humans, telomere length is inversely correlated with chronological age; but with the recent interest in longitudinal tracking of telomere length in humans, evidence for possible telomere lengthening within an individual is emerging. 23 –31 Because telomere length can vary within different cell lineages, average telomere length is a function of the distribution of different cell types and their telomere lengths at any given time. Thus, for complex tissues, one cannot easily distinguish between true telomere length changes versus a shift over time in subsets of cells in the sampled tissue(s).
In the late 1990s, we (Harley and colleagues at Geron Corporation and the Hong Kong University of Science and Technology) conducted a screening program for telomerase activators, which led to the discovery that certain small-molecule components of Huang Xi, a traditional Chinese medicine reputed to maintain health, were activators of telomerase. 1,22,32 –34 Definitive pharmacodynamic studies and randomized, placebo-controlled studies with these molecules in humans have not been completed, but the majority of studies to date have suggested that they modestly activate telomerase and/or help maintain telomere length in vitro and in vivo, and that they have positive functional effects on human cells. In addition, a number of recent studies have suggested that telomerase activation in mice with shortened telomeres and signs of engrained age-related disease can be rescued in part through telomerase activation without signs of increased global cancer risk. 14,20 –22 Thus, telomerase activation is gaining support as a potential treatment or prevention of degenerative diseases using drugs and for health maintenance using dietary supplements.
In our first analysis of PattonProtocol-1, a commercial health maintenance program composed of TA-65® (a natural product–derived telomerase activator), other dietary supplements, and physician counseling, we reported positive immune remodeling over a 1-year period relative to baseline values. 1 These changes included significant declines in senescent cytotoxic (CD8+/CD28−) T cells, particularly in cytomegalovirus (CMV)- seropositive subjects. In addition, we found that TA-65 alone increased telomerase in human cells in culture. In aged mice with shortened telomeres, TA-65 reduced the percentage of cells with short telomeres and improved the structure of multiple tissues. 22 A recent study on the association between telomere length and experimentally induced upper respiratory track viral infection in healthy adults 35 underscored the predictive value of short telomeres for viral infections and clinical illness, especially when telomere length was measured in CD8+/CD28− cells.
Here we report on observed changes from baseline in metabolic and cardiovascular markers, including bone mineral density, from the same set of subjects consuming TA-65 for a 1-year period.
Methods
PattonProtocol-1
PattonProtocol-1 was launched in January, 2007, by TA Sciences (New York, NY) as a commercial age-management product composed of a natural product-derived telomerase activator (TA-65®, described below), a dietary supplement pack, laboratory testing, and physician counseling. Further details are found in Harley et al. 1 All subjects signed a comprehensive Customer Acknowledgement Form. Baseline assays (Table 1) indicated that most individuals were within the normal ranges (data not shown). The consulting physician prescribed new medications for only 3 subjects. There was no qualitative change in the overall conclusions whether these subjects were included or excluded from the analyses. The number of subjects at 3, 6, 9, and 12 months for most tests was 43, 59, 27, and 37, respectively. The age and gender frequencies of the subset at each time-point were similar to those of the total baseline population (n=114; 63±12 years, 72% male).
The mean, standard deviation, and linear regression statistics for test values vs. age are provided for all baseline subjects (n=number).
Slope (m) of the linear regression line of test value versus age of subjects.
p value for significance of the regression line slope. p values less than 0.05 are shaded.
DHEA, dehydroepiandrosterone; LDL, low-density lipoprotein; SD, standard deviation; NA, not applicable; SBP, systolic blood pressure; DBP, diastolic blood pressure.
TA-65®
TA-65® was exclusively licensed from Geron Corporation (Menlo Park, CA) to TA Sciences (New York, NY). It is a single-molecule entity with 95% purity by high-performance liquid chromatography (HPLC) derived from a proprietary extract of the dried root of Astragalus membranaceus. All data in this report are from the original TA-65 product. Post 2011, the purity of the manufactured product has improved from roughly 95% to >98%.
Clinical laboratory assays
At baseline and each time point after initiation of the product, blood samples were drawn from each subject (for plasma or serum assays) and shipped the same day at ambient temperature to appropriate commercial, academic, or contract laboratories. Assays for standard blood counts, blood chemistry (including glucose, insulin, hemoglobin A1c, and serum vitamins), specialized immune subsets (CD8+, CD28−, and CD95−, both gated on CD8+), CMV antibody titer, and inflammation markers (homocysteine and cardio C-reactive protein) were all conducted at a standard clinical laboratory (either Quest Diagnostics, Bio-Reference Laboratory, or UCLA Clinical Laboratories and Pathology Services). Data related to the immune markers have been reported previously. 1
Bone mineral density
Bone mineral density (BMD) was analyzed at baseline and at 12 months on the first available 31 subjects at PhysioAge Medical Group (New York, NY) to reach the 12-month time point. Full anteroposterior (AP) spine L1–L4 and dual proximal femur (neck, trochanter, and dual mean) bone density data were generated using a dual-energy X-ray absorptiometry (DEXA) instrument (GE Healthcare).
Statistics
Because data were collected primarily as a hypothesis-generating exercise and the clients were not participating in a controlled clinical study, statistical analysis was not formally defined a priori. Baseline data were primarily analyzed for cross-sectional donor age effects to compare results with the PattonProtocol-1 population. Where significance of linear regression lines is reported for cross-sectional analysis, the F-distribution was used to calculate the probability that the observed correlation occurred by chance and p values are reported. Modeling of the 1-year change in values used a multilevel or mixed model with random intercepts and slopes. Each person had an individual starting point and an individual slope for change over time on treatment. For each dependent variable, we first graphed the data, looking for outliers and for points that indicated the presence of disease. Erroneous data entries were corrected, as were entries indicating either a failure to follow protocol (e.g., glucose over 125 or insulin over 20 indicating non-fasting). Systolic blood pressure (SBP) over 160 or diastolic blood pressure (DBP) over 100 was taken to indicate hypertension. These relatively high cutoffs for SBP and DBP were chosen so as not to exclude those individuals with possible metabolic syndrome but not currently carrying a diagnosis of hypertension or on anti-hypertensive medication. Graphs were examined for non-linear trends, and multi-level models were used to account for dependence in the data. For each dependent variable, we tested a relatively full model that included fixed effects of time, time squared, baseline age, sex, telomere length, and CD8+CD28− T cells using unstructured co-variance. Time, age, and sex were kept in all models. Other variables were eliminated if the parameter estimate was close to 0 and the p value above 0.10. The initial model included random effects for intercept, slope, and slope squared. The random effect of slope squared was deleted if the fixed effect for time squared was deleted. The resultant model was tested with three different covariance structures, unstructured, compound symmetry, and auto-regressive, and the choice made was based on the Akaike information criterion (AIC).
Results and Discussion
Key baseline observations
Most subjects for this study were relatively affluent individuals motivated to maintain personal health, and thus may not reflect the general population. Table 1 shows mean values, standard deviations, count, slope, and R 2 from linear regression on subject age, and the statistical significance of the slope for the baseline tests investigated in this report. As expected, this population showed a statistically significant increase as a function of client age in fasting blood glucose (0.33 mg/dL/year), SBP (0.51 mmHg/year), and homocysteine (0.066 μmol/L/year), and a significant decrease in dehydroepiandrosterone (DHEA) sulfate (−2.6 μg/dL/year). The increase in serum folate (0.12 ng/mL per year) was unexpected but may reflect the relatively greater use of folic acid–containing multivitamins in older compared to younger subjects prior to starting the protocol.
As described previously, 1 by cross-sectional analysis, telomere length declined in a characteristic manner in this population as a function of client age in both lymphocytes and granulocytes (55 and 34 bp/year; p=10−15 and 10−8, respectively).
Changes from baseline while on PattonProtocol-1
The baseline analysis confirmed that test data from TA Sciences subjects were similar to those reported in other elderly groups and provided a benchmark 36 against which we could plot relative changes with time on the PattonProtocol-1. As discussed earlier, it is important to note that we cannot determine the contribution of any single component of the PattonProtocol-1 to the observed changes. Changes from baseline that are unusual in comparison to other dietary supplement studies could be due to TA-65® and its effects on telomeres, but it is also possible that placebo effects or the unique combination of ingredients in the TA Sciences dietary supplement pack also play a role. Medical/lifestyle questionnaires at baseline and after the 12-month period for each client were used to record changes in medications, diet or exercise while on the PattonProtocol-1. No clients reported significant changes in diet or exercise, but where clients reported a change in drug therapy, the test results that the physician felt could be significantly impacted by the medication change were excluded from the analysis. Because this study did not have a control group, seasonal effects could also be a factor, but as the 114 clients studied here were enrolled over a 2.5-year period, it is unlikely that seasonal effects influenced the observed changes from baseline. With these caveats in mind, we summarize the most interesting findings below.
Observed changes from baseline: Blood sugar, cholesterol, blood pressure, inflammatory markers, vitamin levels, and BMD
Fasting glucose and insulin levels both declined with time in clients on the PattonProtocol-1 (at a rate of −3.72 mg/dL and −1.32 mIU/mL per year, respectively; Table 2). Decreases of this magnitude for fasting glucose are significant relative to the mean baseline values and the donor-age dependent change per year in the baseline population (98 mg/dL and +0.34 mg/dL per year, respectively, from Table 2). In the general population, Sehl et al. 36 reports 0.5–1.5 mg/dL per year increase in fasting glucose. On a relative basis, PattonProtocol-1 apparently reversed ∼11 years of mean increase in fasting glucose. The concomitant reduction in fasting glucose and insulin is indicative of an improvement in insulin sensitivity. Shorter leukocyte telomere length has been associated with insulin resistance, oxidative stress, and metabolic syndrome. 37 –39 It is possible that the combination of anti-oxidants and increased telomerase activation improved insulin sensitivity in our subjects, although the exact mechanism is unknown.
Shown are the parameter estimates and (p-values) from the model as described in the Methods section.
LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Total cholesterol and low-density lipoprotein cholesterol (LDL-C) also decreased significantly. At 12 months, the 13.2 mg/dL and 11.8 mg/dL decreases in total cholesterol and LDL-C, respectively, were statistically significant (p=0.002 for both) and large compared to the small decrease associated with client age in this population (−0.29 mg/dL per year and −0.37 mg/dL per year, respectively). Cholesterol generally increases with age, 40 possibly due to reduced clearance of LDL from circulation and reduction in conversion of cholesterol to bile acids, but some studies have suggested a flat profile with aging or even a reduction in total cholesterol with age attributed to poor health. 41 Because the baseline average total cholesterol in the PattonProtocol-1 clients was borderline high (mean 188 mg/dL, Table 2), we consider the declines of ∼10 mg/dL in total cholesterol and LDL-C to be beneficial because it is comparable to what has been achieved in successful diet and exercise programs. 42 The mechanism of the reduction in cholesterol is unclear, but given that no subjects reported changes in their exercise or dietary habits, it is possible that increased telomerase activation from the PattonProtocol-1 contributed. A small study demonstrated that increased telomerase activity in peripheral blood mononuclear cells (PBMCs) is significantly associated with a decrease in LDL-C. 43
SBP and DBP declined 17.8 mmHg and 4.2 mmHg, respectively, over the 1-year period (Table 2). In the baseline population, DBP was relatively flat but SBP increased 0.51 mmHg/year (Table 2), comparable to that seen in other studies, 44 suggesting that the PattonProtocol-1 may have reversed >30 years of increase in SBP. The decrease in SBP is comparable to first-line therapy with diuretics, which confer a significant reduction in cardiovascular events. Using the Framingham 10-year CVD event calculator, these reductions would cause a 25% reduction in 10-year risk for males (from 8% to 6%). Mechanisms are difficult to determine given the observational nature of the study, but telomere attrition has been associated with higher blood pressure and increased aldosterone production, 45 which in turn can increase oxidative stress and blood pressure by reducing nitric oxide production. If the reduction in percentage of short telomeres and senescent cytotoxic T cells we reported previously also resulted in decreased inflammatory cytokines (such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6), this process could have been reversed in our cohort and could explain the reduction in blood pressure. This reversal of inflammation along with increased telomerase activation could rescue pre-senescent endothelial cells and increase the production of nitric oxide, which could reduce SBP. The supplement packs could also have contributed.
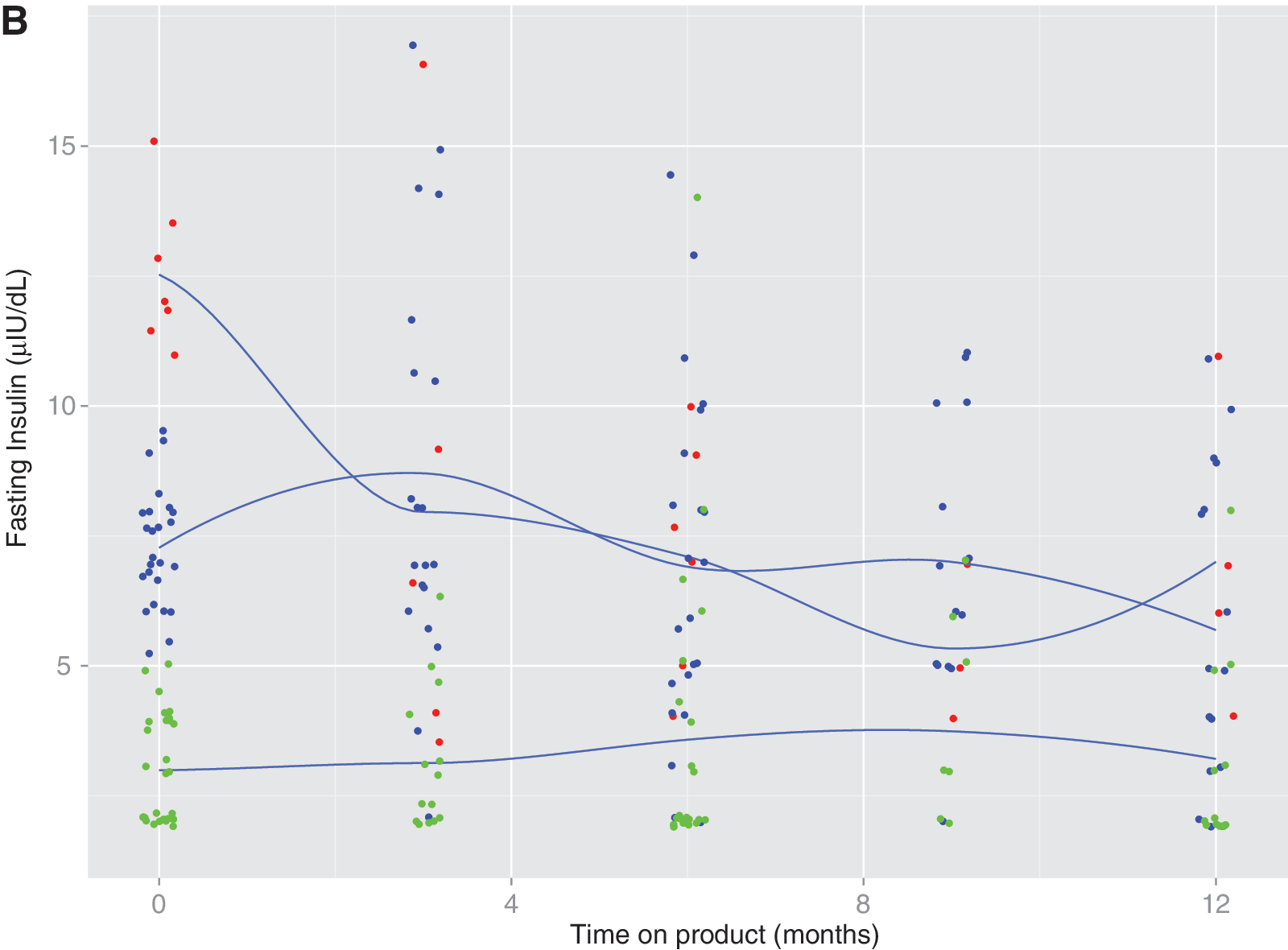
The changes we observed could not continue year after year. To explore whether the slope of observed trends is constant regardless of the starting level of the dependent variable, we generated sub-group spline graphs. Figure 1A shows a graph of fasting glucose levels over time. Levels of glucose at baseline were divided into three groups: Low (below 88 mg/dL), high (above 102 mg/dL), and middle (the middle 50%). Splines were fit to each group. The overall trend was for those in the highest group to have relatively large declines, those in the mid-range smaller declines, and those in the lowest group a slight increase. Figure 1B is similar for insulin, except here groups were set based on medical expertise: High (above 10 mg/dL), low (below 5 mg/dL), and middle and patterns were similar to those for glucose. These patterns suggest an improvement in insulin sensitivity. Insulin resistance is a cardinal element of the metabolic syndrome and thought to be a result of increased inflammation, which the PattonProtocol-1 might have reduced. From a clinical standpoint, this pattern of effectiveness is similar to metformin, a first-line therapy for pre-diabetes.
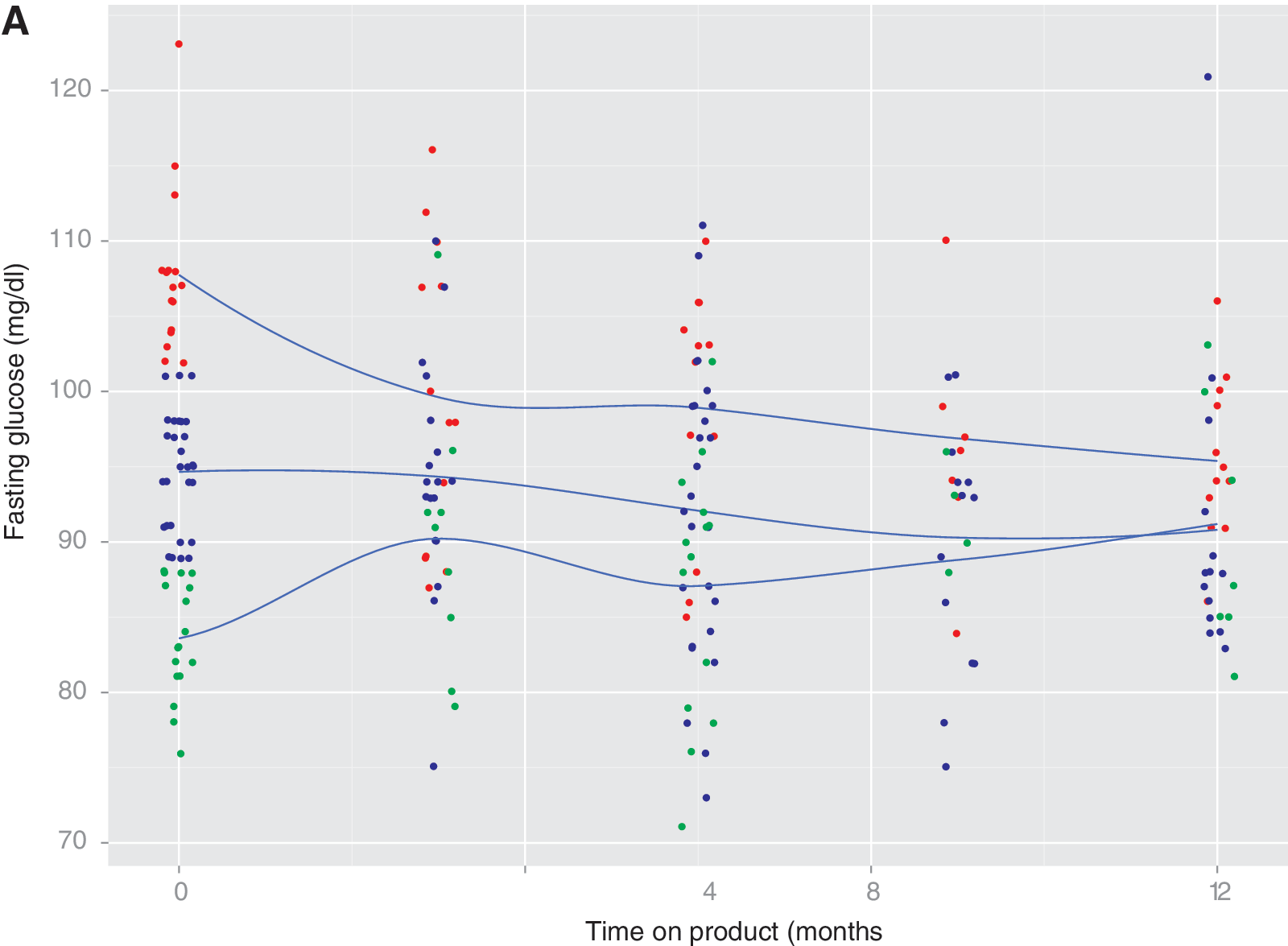
Spline graphs based on the multi-level model, representing the change over time (baseline to 12 months) for fasting glucose (
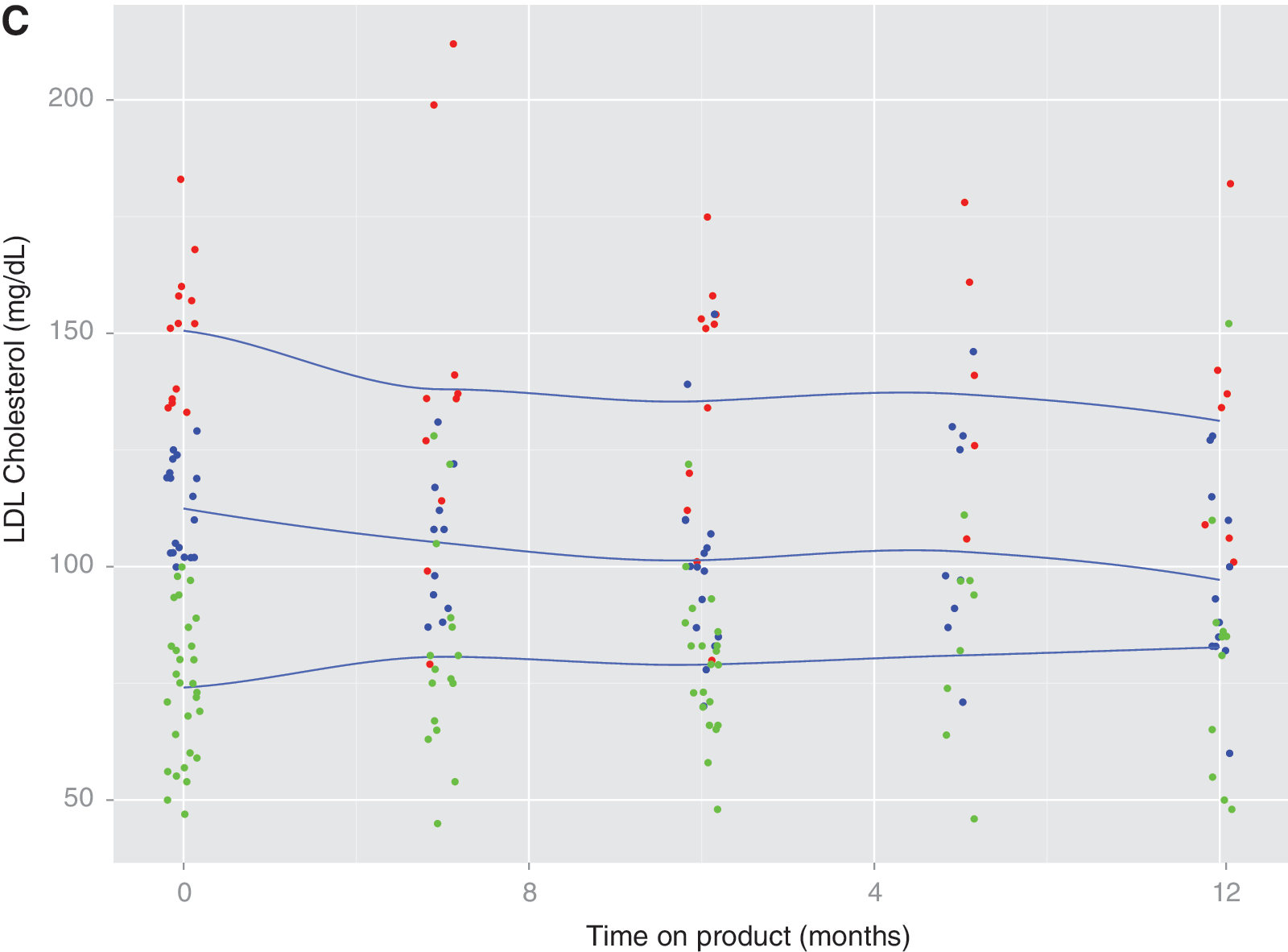
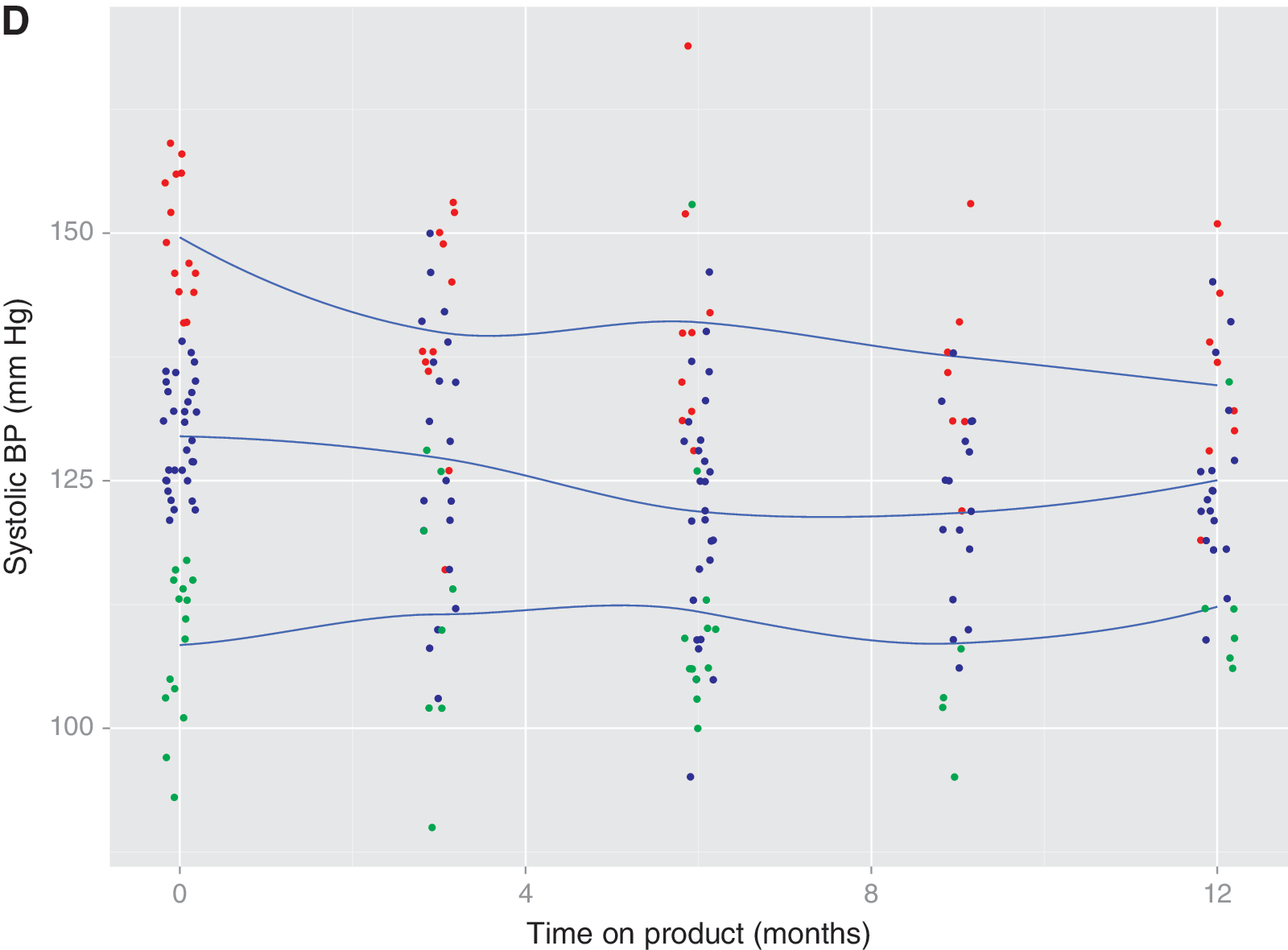
The same pattern is demonstrated by the spline graphs for LDL-C (Fig. 1C) and SBP (Fig. 1D). The cholesterol groups were divided by the treatment categories defined by the National Cholesterol Education Program: Low (<100 mg/dL), middle (100–130), and high >130), and the SBP groups were tertiles, where high was above 138 mmHg, low below 120 mmHg, and middle 120–138 mmHg. The moderating trends show biomarker improvements in those that need it, with little or no change in those within the normal biomarker range. The moderating trend for SBP fits with the mechanisms of SBP reduction discussed above in which a dysfunctional endothelium (in those with higher baseline SBP) is repaired, rather than a direct anti-hypertensive effect, which could result in hypotension. One might see these moderating trends as regression to the mean, but the decreasing variance over time that is evident from all four of the spline graphs argues against this.
Homocysteine and C-reactive protein (CRP) are significant markers of inflammation and are associated with arterial dysfunction and cardiovascular disease risk. 16,46 We observed significant reductions in both homocysteine (Table 2) and CRP (not shown) while clients were on the PattonProtocol-1, but for CRP, a number of individuals had acute spikes in CRP, possibly related to infections, which confounded the analysis. The 3.6-μmol/mL decrease in homocysteine in clients on the Protocol (p≤0.001) is dramatic compared to the general increase with age (0.066 μmol/mL per year). It is likely that folate and vitamins B12 and B6 in the supplement packs played a role in the decline in homocysteine, but a number of individuals who were taking potent supplement packs before initiation of the protocol also showed reductions in homocysteine, including some subjects whose folate levels actually decreased (data not shown). It is also possible that other components of the Protocol reduced inflammatory response and improved health through elongation of short telomeres and remodeling of the immune system. If reduction in inflammation and cardiovascular risk could be achieved through PattonProtocol-1 without high levels of folate found in some dietary supplement programs, this would be beneficial because supra-physiological levels of folate could be detrimental. 47,48
Finally, bone mineral density was measured at baseline and 12 months in an essentially random subset of individuals (n=31). Of the 31 subjects, 26 were either not on hormone therapy or made no change in hormone therapy during the 1-year period. The remaining five subjects who changed therapy were excluded from the analysis. Of the 26 analyzed subjects, one had osteoporosis and four others had varying degrees of osteopenia. In the overall group, there was a 2.0% increase in AP spine L1–L4 BMD (p=0.003) (Table 3). This is as large an increase in BMD as seen in a 3-year study of calcium and vitamin D therapy in comparable subjects without osteoporosis 49 and certainly contrasts with the expected ∼0.5% decrease per year. There were no significant changes in hip BMD (data not shown). Moreover, because the average baseline vitamin D levels were well into the normal range, it is less likely that the approximately 20% increase in vitamin D contributed significantly to the BMD increase. A plausible alternative explanation for this improvement in BMD could be related to the emerging understanding of the relationship among hyperlipidemia, T cells, and bone density. 50 The reduction in senescent suppressor cells that we previously reported 1 combined with the reduction in LDL-C could decrease the number of activated T cells in the bone marrow and thereby reduce activated RankL and other inflammatory cytokines. This would reduce osteoclast activity and potentially explain the improved bone density.
Bone mineral density (g/cm3) data are reported for 26 evaluable subjects (individuals who changed hormone therapy during the 12-month period were excluded). p values less than 0.05 are shaded. Average age of males at baseline was 64.9±12.0 and that of females was 58.3±5.1.
Discussion and Conclusions
This study adds to the observations from 2011 that PattonProtocol-1, containing conventional supplements plus TA-65, a small-molecule telomerase activator, has a positive impact on biomarkers of aging or age-related disease. The initial observational study of roughly 50 subjects on product 1 focused on results from independent diagnostic laboratory testing of immunological markers over a 1-year period, while here we focus on similar laboratory testing of metabolic biomarkers and bone mineral density in the same cohort over the same 1-year period. We found reductions in fasting blood sugar, insulin, cholesterol, blood pressure, and homocysteine, and increases in bone mineral density, all considered positive health changes. These data suggest that PattonProtocol-1 (TA-65 in combination with other supplements and physician counseling) improves health and may reduce risk of morbidity and mortality.
The major limitation of these observational studies is that they are not randomized, placebo-controlled trials with defined dosing of TA-65. Such a study is in progress, but the observation that TA-65 was primarily beneficial to CMV-positive humans who were “blind” to their CMV status, 1 and that TA-65 had positive effects when given to aged telomerase-positive but not telomerase-negative mice, 51 suggests that TA-65 is an active molecule that should be investigated further.
Because telomerase may extend the life span of relatively rare pre-malignant cells that otherwise might die due to critical shortening of telomeres, it is possible that a telomerase activator could increase cancer risk in some individuals. However, prevention of critical shortening of telomeres in multiple tissues throughout an aging human by telomerase activation could be a net tumor suppressive mechanism by reducing genomic instability and maintaining health of normal tissues. Much larger controlled studies will be needed to assess the potential risk and benefits of TA-65 in humans.
Subjects taking TA-65 or any dietary supplement should consult their doctor and carefully consider the product's potential risks and benefits. There had been approximately 260 person-years of TA-65 dosing, mainly in the 5–50 mg/day range through June, 2010, with no reports of new diagnoses of cardiovascular disease or cancer. This represented age-adjusted incidence rates significantly below the average US rates for CVD and cancer. As of June, 2013, there are now an estimated 7000+ person-years of TA-65 exposure at an average 50-mg TA-65 dose equivalence. Disease and mortality were not formally tracked, but TA Sciences reports few if any adverse events, and no cases of adverse events being attributed to TA-65 by the subjects' doctors. In the overall (all ages) US population, 7000 person years of life would entail about 30 new diagnoses each for cancer and CVD, and about 60 deaths, based on data from the Centers for Disease Control and Prevention. Because of lack of matching demographics for the study population, as well as lack of exact disease and mortality data, we cannot make a reliable comparison of incidence rates in the study population versus the general population, but the data to date do not point to increased risk of morbidity or mortality in subjects taking TA-65. In conclusion, TA-65, a moderate telomerase activator, is a novel dietary supplement that may enhance one's health span.
Footnotes
Acknowledgments
We thank Dr. Russ Kerschmann and Dr. Lennart Olsson for critical review of the manuscript.
Author Disclosure Statement
C.B.H. is one of the inventors of TA-65, is a paid consultant to TA Sciences, and is the Chief Scientific Officer of Telome Health, Inc., which has a license arrangement with TA Sciences. C.B.H. owns stock and stock options in Telome Health. W.L. is an employee of TA Sciences. J.M.R. offers TA-65 in his office and is on TA Sciences Scientific Advisory Board. P.L.F. declares no conflicts of interest.