
Abstract
Background and Aims:
Advanced glycation end products (AGEs) contribute to cardiovascular disease in patients with hemodialysis (HD). We have recently found that carnitine levels are inversely associated with skin AGE levels in HD patients. We examined whether
Methods:
This was a single-center study. One hundred and two HD patients (total carnitine levels <50 μmol/L) were enrolled and randomized to either oral administration of
Results:
There were no significant differences of clinical variables at baseline between the control and
Conclusions:
The present study demonstrated that oral
Introduction
R
Carnitine, a natural substance that could contribute to transport long-chain fatty acids from the cytoplasm to mitochondria, has been known to play a central role in fatty acid β-oxidation and subsequent adenosine triphosphate (ATP) production in a variety of cells. 20 Furthermore, because carnitine regulates the function of mitochondrial respiratory chain and oxidative stress generation as well, 20 carnitine deficiency might be involved in muscle weakness, cardiac hypertrophy, and accelerated atherosclerosis in hemodialysis (HD) patients. 21 –23
We have found that serum carnitine levels are inversely associated with skin accumulation levels of AGEs evaluated by SAF in patients with HD.
23
Given the inhibitory potential of
Methods
Patients and study protocol
This study was a prospective, randomized, comparator-controlled, single-center trial involving 6 months of study drug administration and follow-up. In all, 102 HD patients (mean age, 67.5±12.7 years old; mean duration of HD, 99.5±85.3 months), whose serum total carnitine levels were less than 50 μmol/L, were enrolled in this study. Age- and sex-matched healthy subjects (n=75, mean age 65.4±10.3 years old) were used as a control. HD patients were randomly assigned to oral
Informed consent was obtained from all subjects, and the study protocol was approved by the Institutional Ethics Committees of Kurume University School of Medicine and Sugi Cardiovascular Medicine Hospital, Japan. This work was conducted in accordance with the Declaration of Helsinki. This trial was registered with the University Hospital Medical Information Network clinical trials database (UMIN000010953).
Data collection
Medical history was ascertained by a questionnaire. Blood pressure was measured in the sitting position using an upright standard sphygmomanometer just before starting HD. Vigorous physical activity and smoking were avoided for at least 30 min before blood pressure measurement.
Blood was drawn from an arteriovenous shunt just before starting the HD session for determinations of hemoglobin, total protein, albumin, lipids (low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides), blood urea nitrogen, creatinine, uric acid, calcium, phosphate, and C-reactive protein (CRP). Whole parathyroid hormone (PTH) was evaluated by an immunoradiometric assay (IRMA; Allegro I-PTH, Nichols Institute, San Juan Capistrano, CA). β2-microglobulin (β2-MG) was measured by a latex immunoagglutination assay (Eiken Chemical Co., Ltd. Tokyo, Japan). Serum carnitine levels were determined by enzyme cycling methods, as described previously. 25 Other blood chemistries were measured at standard enzymatic methods as described previously (Wako Pure Chemical Industries, Ltd, Osaka, Japan). HD adequacy was evaluated by a single-pool fractional clearance of body water for urea (Kt/V). 26 Tissue accumulation levels of AGEs were evaluated quantitatively by measuring SAF with an AGE reader according to the supplier's recommendations (DiagOptics BV, Groningen, Netherlands). 15 We measured SAF just before HD sessions on non-shunt arm. Use of skin creams was prohibited when measuring the SAF.
Statistical analysis
Data are presented as mean±standard deviation (SD). Use of renin–angiotensin system (RAS) inhibitors and statins and the presence or absence of diabetes mellitus were coded as dummy variables. Because triglycerides and whole PTH levels were not normally distributed, log-transformed values were used for analysis. An unpaired t-test was performed to compare clinical valuables among healthy subjects, controls, and the
Results
Demographic data at baseline
Thirty-two patients did not complete the assessment or treatment of the study. Finally, 70 patients completed the study (n=38 in the control group and n=32 in the

Enrollment, randomization, and follow-up of the study patients. CVD, cardiovascular disease.
Demographic data at baseline are shown in Table 1. There were no significant differences of baseline data between the two groups, including metabolic, hemodynamic, anthropometric, and inflammatory variables. At baseline, total and free carnitine levels were significantly lower, whereas acyl carnitine, acyl/free carnitine ratio, and SAF were higher in HD patients compared with healthy subjects (total, free, acyl carnitine, acyl/free carnitine ratio, and SAF in HD and control subjects; 36.3±7.6 vs. 59.3±10.6 μmol/L (p<0.001), 21.7±4.5 vs. 47.3±9.2 μmol/L (p<0.001), 14.6±3.9 vs. 12.1±3.7 μmol/L (p<0.01), 0.69±0.18 vs. 0.26±0.09 (p<0.001), and 3.17±0.80 vs. 2.25±0.44 (p<0.001), respectively.
Values are shown as mean±standard deviation (SD) or range.
These variables are shown in the original scale after using log-transformed values.
No., number; HD, hemodialysis; BUN, blood urea nitrogen; Cr, creatinine; Ca, calcium; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; PTH, parathyroid hormone; CRP, C-reactive protein; β2-MG, β2-microglobulin; SAF, skin autofluorescence; RAS, renin–angiotensin system.
Effects of l -carnitine supplementation on clinical variables
Total, free, acyl carnitine, LDL-C, and triglycerides levels just before the HD session were significantly increased by
Values are shown as mean±standard deviation (SD) or range.
These variables are shown in the original scale after using log-transformed values.
AST, aspartate transaminase; ALT, alanine transaminase; BUN, blood urea nitrogen; Cr, creatinine; Ca, calcium; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; PTH, parathyroid hormone; CRP, C-reactive protein; AGEs, advanced glycation end products; β2-MG, β2-microglobulin.
Effects of l -carnitine supplementation on skin AGE levels
After 6-month treatments, skin AGE levels measured by SAF were significantly decreased in the
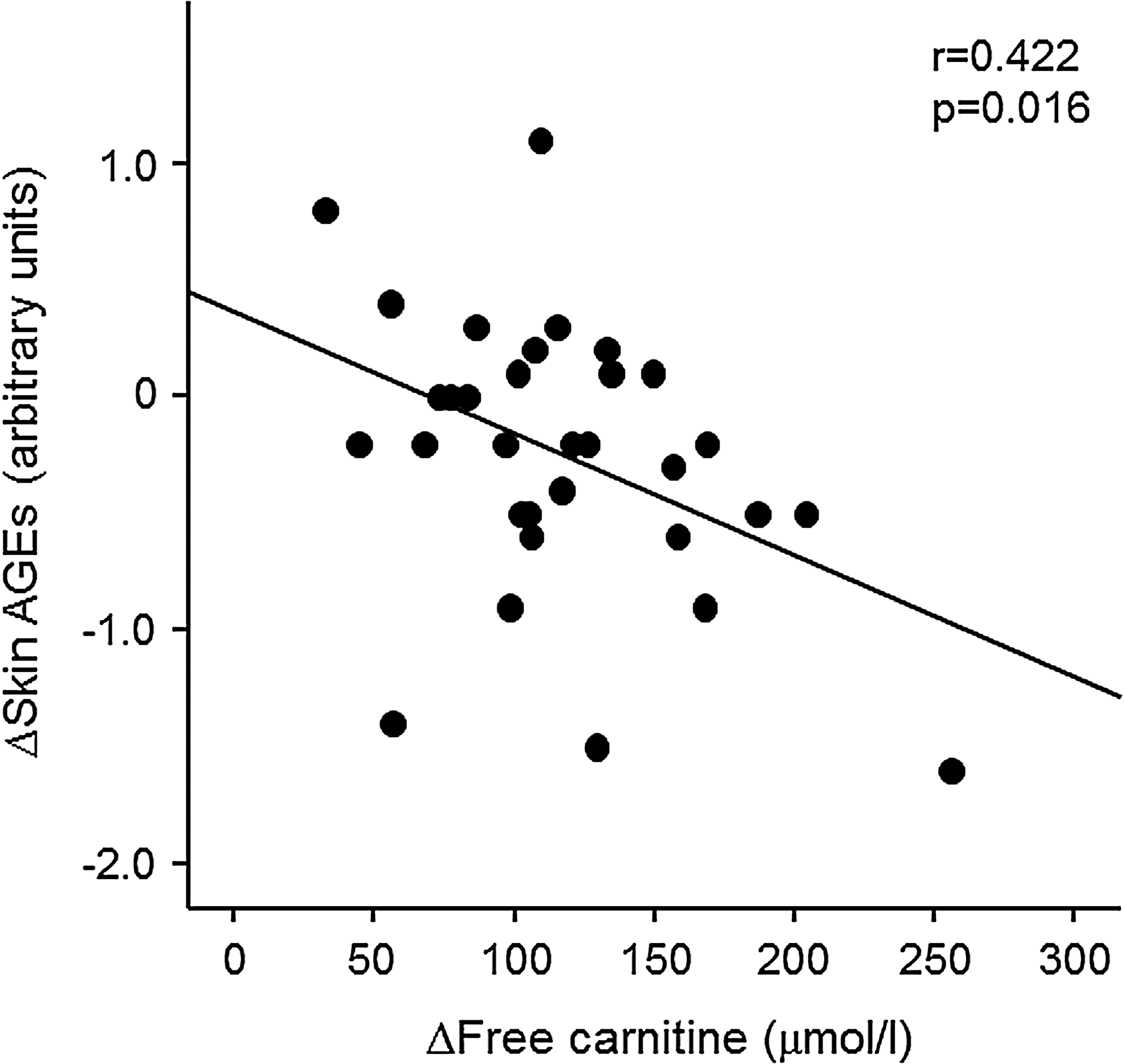
Correlation between Δskin advanced glycation end products (AGEs) and Δfree carnitine in
R 2=0.178
AST, aspartate transaminase; ALT, alanine transaminase; BUN, blood urea nitrogen; Cr, creatinine; Ca, calcium; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; PTH, parathyroid hormone; CRP, C-reactive protein; β2-MG, β2-microglobulin.
Discussion
We found here that: (1) Total, free, and acyl carnitine levels were significantly lower in HD patients, whereas tissue accumulation levels of AGEs evaluated by SAF were higher, (2) 900 mg of
In vitro study has shown that
Tissue accumulation levels of AGEs evaluated by SAF are elevated in HD patients.
15,16
Furthermore, we, along with others, have shown that SAF is correlated with high-sensitivity CRP and the carotid pulsatility index and could predict future cardiovascular events and death in end-stage renal disease patients undergoing HD.
15,16
These observations suggest that reduction of AGE accumulation in the skin might be a novel therapeutic target for preventing CVD in HD subjects. Given the facts that: (1) Carnitine levels were associated with the increased risk of CVD in uremic patients,
28
(2) administration of
β2-MG has been shown to contribute to HD-related amyloidosis.
30,31
Furthermore, its serum levels are positively correlated with inflammatory variables
30
and inversely associated with circulating endothelial progenitor cell number.
31
These findings suggest that increased β2-MG could contribute to impaired endothelial cell repair, thus being involved in CVD in HD subjects. In this study,
Malnutrition is one of the strongest predictors for disabilities and high mortality rate in patients with HD.
33
We have recently shown that serum albumin and LDL-C levels are significantly decreased in HD patients, and these levels were positively associated with serum carnitine levels.
23
In the present study, after 6-month observation periods, total protein and albumin levels were significantly decreased in control group, whereas LDL-C and triglycerides levels were increased in the
Limitations
In this study, we used only SAF to assess tissue AGEs. This might be a weak methodology because it is nonspecific. Thus, it would be helpful to examine whether
In the present study, SAF not only decreased in the intervention group but also in the control group, although the change did not reach significance in the latter group. Furthermore, there was no significant difference (only trend) of ΔSAF between the two groups. Therefore, the effects of
Some of the data points on ΔSAF over 6 months were >1 arbitrary unit change. However, because we measured SAF just before HD sessions and that the use of skin creams was prohibited when measuring the SAF, it was unlikely that these factors could affect the present results.
Footnotes
Acknowledgments
This work was supported in part by a Grant-in-Aid for Welfare, and Scientific Research (C) (no. 25461239) from the Ministry of Education, Culture, Sports, Science and Technology of Japan (K.F) and by Grants of MEXT-Supported Program for the Strategic Research Foundation at Private Universities, the Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan (S.Y.).
Author Disclosure Statement
The authors have no conflicts of interest to declare.