
Abstract
To evaluate a possible involvement of the brain-derived neurotrophic factor (BDNF) Val66Met polymorphism in susceptibility to Parkinson's disease (PD), we performed a meta-analysis of all studies on the topic published from 2002 to 2014. This article reviews and compares the data from two previous meta-analyses, including two studies not previously considered. We selected studies referring to a genetic comparison between PD patients and healthy controls, so 15 studies involving 3754 cases and 4026 controls were included in our meta-analysis. We found no association between the Val66Met polymorphism and the risk of developing PD in our overall analysis. The ethnicity-specific meta-analysis produced no significant association either. Our data do not support a major role for the BDNF Val66Met polymorphism in the pathogenesis of PD.
Introduction
P
It has been proposed that the neurodegenerative process may result from an insufficient supply of neurotrophic factors, a family of proteins that aid in the differentiation, survival, and maintenance of specific neuronal populations, including the brain-derived neurotrophic factor (BDNF), which promotes dopamine uptake of midbrain dopaminergic neurons in vitro. 2 Decreased BDNF mRNA expression and protein content have been observed in the substantia nigra of PD patients, 3,4 making BDNF a logical candidate gene for susceptibility to PD. Over the past decade, the potential role of the BDNF gene in the pathogenesis of PD has been the object of much investigation, leading to inconsistent results. The most explored polymorphism in BDNF is a common non-conservative single-nucleotide polymorphism (SNP), Val66Met, located at nucleotide 196 (G/A) in the pro-protein of BDNF. This functional polymorphism produces an amino acid change at codon 66, resulting in abnormal intracellular distribution and low activity-dependent secretion of BDNF. 5,6 Numerous research groups investigated a probable association between this SNP and the risk of PD with conflicting results, and this discrepancy might be attributable to different factors, such as sample size, statistical power, clinical heterogeneity, or combination of them. To overcome the limitations of individual studies and resolve inconsistencies, this meta-analysis represents an important research strategy to combine different results and determine whether variations in effect among them are due to different analytical approaches, to variations in the samples used, or to random statistical fluctuation. Very recently, two meta-analyses have tested the pooled data on this issue and have come to different conclusions. 7,8 In an attempt to resolve these contradictory results, we performed the current meta-analysis including two new studies and comparing the data from the two previous meta-analyses.
Methods
Selection of studies
To identify appropriate studies for meta-analysis, we searched PubMed, Scopus, and the ISI Web of Knowledge using the keywords “Parkinson's disease,” “BDNF,” “G196A,” “Val66Met,” and their combinations in PubMed. We selected papers from 2002 to 2014 and without any language limitation. After reviewing the contents of this first selection, we also reviewed their reference lists to search for additional studies via Google Scholar. We followed the procedural steps indicated by Cochrane (
In Fig. 1, we reported the flowchart that represents the inclusion and exclusion criteria of studies. We included only studies: (1) Showing comparative analyses of PD and healthy populations; (2) analyzing the association between G196A polymorphism of BDNF gene and PD; (3) in which raw data of allele or genotype frequencies or counts were available. The allele was G/A, and the genotype covered GG, AG, and AA. For studies published by the same group on the same gene and markers, only the first report was included.
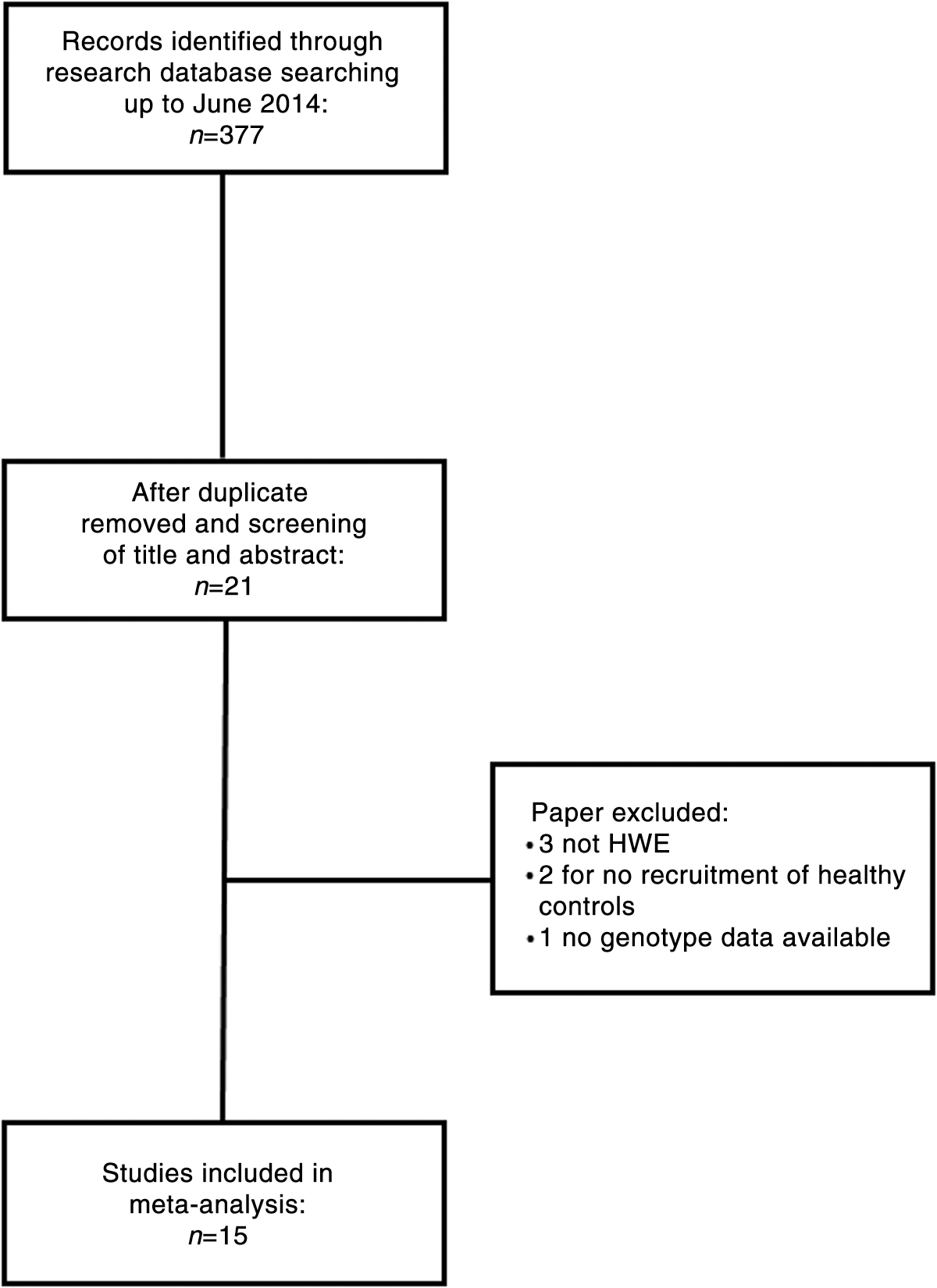
The flowchart of the studies included in the meta-analysis. HWE, Hardy–Weinberg equilibrium.
Data extraction
Two reviewers independently extracted the following data from each study: Name of the first author, year of publication, ethnicity, and both in cases and controls sample size, mean age and percentage of female, and allele and genotype distribution.
Statistical analysis
To investigate the association of the G196A polymorphism with PD, the allele and genotype frequencies of the SNP between PD patients and healthy controls were compared and expressed in terms of odds ratio (OR) with the corresponding 95% confidence interval (95% CI). In each study, three ORs and their corresponding 95% CIs were calculated: (1) Dominant OR (GA+AA versus GG); (2) recessive OR (AA versus GA+GG); 3) OR A versus G; (4) OR GG versus AA. Between-study heterogeneity was assessed by the Q-statistic test and I2 statistic. A p value <0.1 was considered statistically significant for the Q-statistic test. I2 ranges between 0% and 100%; a value of 0% represents no heterogeneity, and larger values represent increasing heterogeneity. A fixed-effect model was performed to obtain the pooled OR, and if there was evidence of study heterogeneity, a random-effects model was applied.
Subgroup analysis was performed to evaluate the possible effect of ethnicity. We performed a separate meta-analysis combining the data of studies that categorized the PD sample based on cognitive impairment 9 –12 or specifically declared to exclude patients with neurological disease. 13,14 A possible effect on the OR of the difference in mean age and gender distribution between PD and control groups was investigated by performing a meta regression analysis. Sensitivity analysis was performed excluding studies that considered patients with PD family history. Publication bias and small-study bias were evaluated with a funnel plot of the data and with the Egger test. Temporal effect was also estimated with a cumulative meta-analysis. A fixed continuity correction was added when a study contained a zero cell. Statistical significance was defined as p<0.05. All statistical analyses were performed using STATA v. 10.1 (Stata Corp, College Station, TX).
Results
Description of studies
By the initial research, a total of 15 studies were eligible for inclusion in our analysis as described in a flowchart (Fig. 1). Characteristics of studies included in meta-analysis are reported in Table 1. Important articles have been excluded from our analysis for different reasons: Three studies were not included because the genotype distributions of controls was not in Hardy–Weinberg equilibrium (HWE). 15 –17 We left out the Foltynie et al. studies 18,19 because they did not report a healthy control group for comparison. Finally, the Karamohamed et al. study 20 was excluded because it did not report the genotype frequency of healthy controls.
HWE, Hardy–Weinberg equilibrium.
In our meta-analysis, a pooled total of 3754 PD patients and 4026 healthy controls was analyzed. The mean age ranged from 57.914 to 69.5 years 11 in PD patients, and from 59.214 to 71.6 years 12 in controls. The percentage of women in PD groups varied from a minimum of 28% 21 to a maximum of 60.5% 22 and in control groups from 33% 21 to 65.7%. 11 Seven studies 13,14,21 –25 were conducted on Asian subjects, six studies 9,11,12,26 –28 were conducted on Caucasian population, one study 29 was conducted on American population, and one had Caucasian background except three patients. 10 Genotype and allele distribution of the G196A polymorphism of the BDNF gene from each study are reported in Table 2. All studies observed HWE. Four studies 11,14,24,28 also included in the PD group patients with a PD family history, so we repeated the analyses excluding them to verify the robustness of our results.
BDNF, brain-derived neurotrophic factor; PD, Parkinson's disease; HWE, Hardy–Weinberg equilibrium.
Four studies stratified the PD sample based on cognitive impairment, 9 –12 two specifically declared to exclude patients with neurological diseases, 13,14 whereas the others omitted this clinical information.
Quantitative synthesis
Allele and genotype distributions of the G196A polymorphism from each study included in meta-analysis are shown in Table 2. Overall the results of our meta-analysis on the basis of different genetic models (dominant, recessive allelic, and homozygote) revealed no significant association between PD patients and the G196A polymorphism. In the fixed-effects model, the pooled OR for the dominant model (GA+AA vs. GG) was 1.07 (95% CI 0.97–1.19, p=0.157; I2=7%). A similar result was obtained when we considered the recessive model (AA vs. GA+GG) OR=1.04 (95% CI 0.91–1.19, p=0.552; I2=9%). No association between the BDNF (AA) genotype and PD was found, pooled OR was 1.06 (95% CI 0.91–1.24, p=0.456; I2=9%), and also between allele A and PD, pooled OR was 1.03 (95% CI 0.96–1.11, p=0.377; I2=24%). All ORs were pooled through a fixed-effects model (Fig. 2).
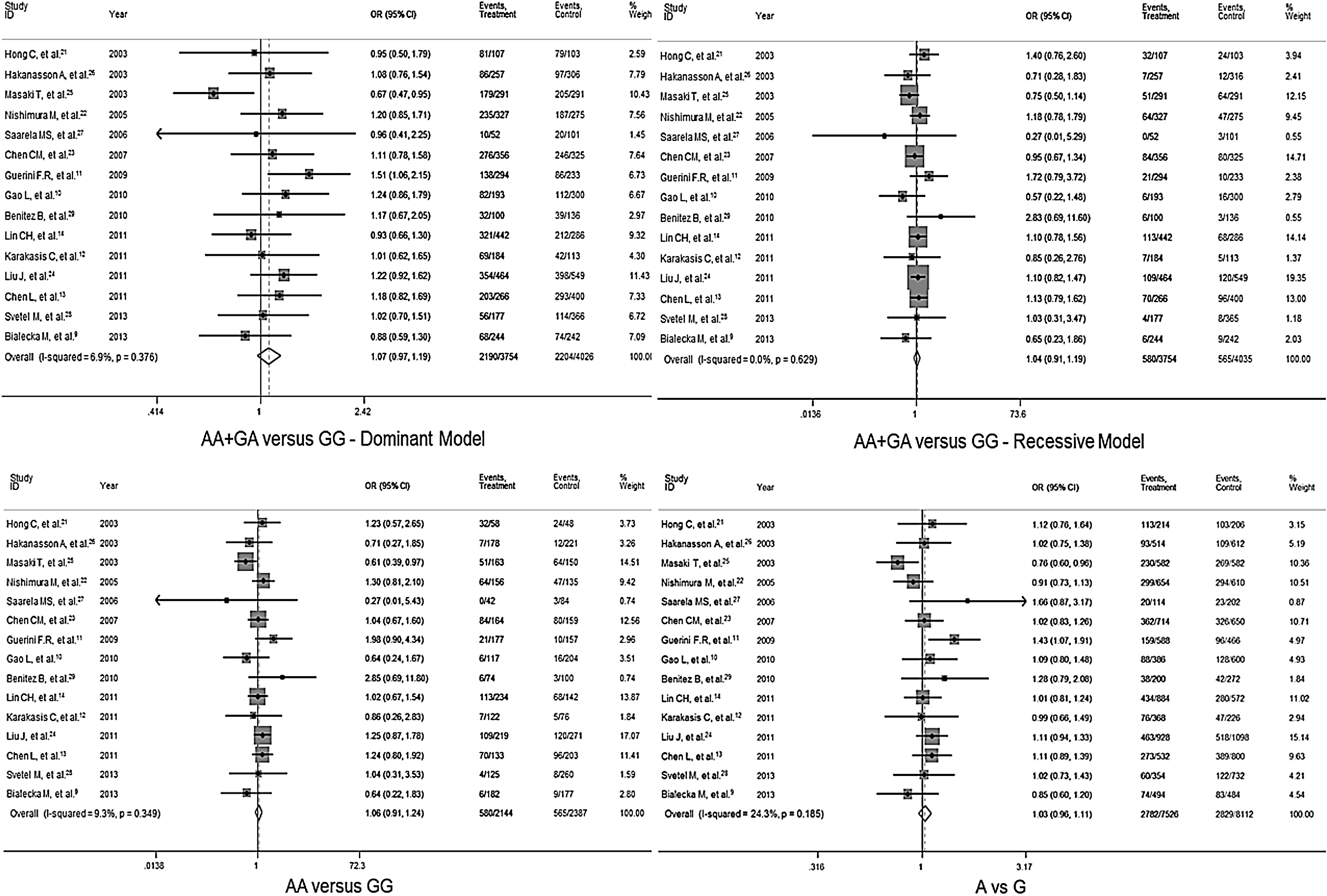
Forest plot of the bone-derived neurotrophic factor (BDNF) G196A polymorphism and Parkinson's disease (PD) risk. OR, odds ratio; CI, confidence interval.
The meta-regression analyses revealed no effect of the difference in the mean age of PD and control groups (dominant model, coefficient=1.0195% CI −0.2, 0.06, p=0.511; recessive model, coefficient=0.99, 95% CI 0.95, 1.04, p=0.659; AA vs GG: coefficient=1.00, 95% CI 0.93, 1.06, p=0.911; A vs. G, coefficient=1.01, 95% CI 0.98, 1.04, p=0.490), as well as for difference in sex distribution between the two groups (dominant model, coefficient=0.99, 95% CI 0.98, 1.0, p=0.192; recessive model, coefficient=1.00, 95% CI 0.98, 1.01, p=0.554; AA vs. GG, coefficient=0.99, 95% CI 0.97, 1.01, p=0.290; A vs. G, coefficient=0.99, 95% CI 0.99, 1.00, p=0.165). Sub-groups analysis showed no effect of the ethnicity in each genetic model. Overall, no evidence of publication bias was present; funnel plots seemed to be symmetrical, and the Egger regression model confirmed this assessment (dominant model, bias=0.61, 95% CI −3.21, 1.99, p=0.620; recessive model, bias=−0.26, 95% CI −1.33;0.80, p=0.602; AA vs. GG, bias=−0.34, 95% CI −1.69, 1.01, p=0.594; A vs. G, bias=0.97, 95% CI −1.14, 3.07, p=0.340). A temporal effect was excluded by cumulative analysis.
Association between the G196A polymorphism and PD with dementia was also calculated by performing a meta-analysis that considered only the four studies that stratified the PD patients on the basis of cognitive impairment 9 –12 and two studies that excluded patients with neurological diseases. 13,14 Information about allele G and A frequencies was absent in one study. 10 For each genetic model, the random-effects model was applied, and the pooled ORs showed no significant association (Table 3).
PD, Parkinson's disease; OR, odds ratio; D-L, DerSimonian-Laird; CI, confidence interval.
Sensitivity analysis
Sensitivity analysis was conducted to verify the robustness of our results. For each genetic model, the exclusion of studies where allele frequencies exhibited a significant deviation from the HWE as well as the exclusion of the studies that considered patients with PD family history showed no important different results.
Discussion
Recently two important meta-analysis have investigated the role of the BDNF 196 G/A polymorphism as potential risk factor for PD reporting conflicting results. 7,8 This topic was already addressed in a previous meta-analysis, including six studies of 1419 PD patients and 1406 healthy subjects, suggesting no association between this polymorphism and susceptibility to PD. 30 This result should be taken with caution because either the sample size was relatively small or the genotype distribution in two included studies 15,16 was not in HWE. Therefore, we have focused only on the two most recent meta-analyses, aiming at resolving the contradictory results. More precisely, Lee and Song 8 identified an association between the BDNF 196 AA+AG genotype and PD in Europeans, but not in Asians, conducting their analysis on 12 separate comparisons corresponding to 2891 patients and 3132 controls. Dai et al., 7 encompassing one additional study 14 and covering 3333 PD patients and 3418 controls, found no association, even after stratifying the analysis on the basis of the ethnicity. This disagreement could be explained by the fact that Dai et al. 7 have considered the PD cases from Gao et al. 10 as a mixed population for the presence of two patients from North Africa and one with a gypsy background, whereas Lee and Song 8 considered the overall sample as European.
Reviewing all of these data, we confirmed that the difference observed between the two meta-analyses was merely due to the diverse interpretation of the data reported by Gao et al. 10 Concerning the studies on Asian samples, the two meta-analyses did not differ for the results, even though Lee and Song 8 had omitted the Lin et al. study 14 in their analysis.
In our meta-analysis, we included two recent case–control studies corresponding to 425 new PD patients and 608 controls and the overall results did not show significant association between 196 G/A polymorphism and PD risk, in line with data reported by both previous meta-analyses. In the sub-group analysis on the basis of the ethnicity, we still confirmed no association as described by Dai et al. 7 and contrary to what was found by Lee and Song. 8 We have repeated the analysis also excluding the Gao et al. study 10 by Caucasian sample and we again obtain negative results. This evidence underlines the focal influence of ethnicity on the frequencies of 196 G/A polymorphism. In fact, the inclusion or exclusion of a sample from a specific ethnic group did provide different outcomes of the analysis. There are numerous findings in the literature regarding the ethnic differences in allelic frequencies of the 196 G/A polymorphism between Caucasian and Asian populations. 31
Positive or negative associations between this polymorphism and some diseases, such as schizophrenia, depression, eating disorders, alcoholism, substance abuse, and anxiety, have been reported in Caucasian and Asian participants and might be explained by ethnic differences. 32 –36 BDNF plays a role in eating behavior, food intake, and energy expenditure. 37 Therefore, ethnic differences in the BDNF 196 G/A polymorphism might be associated with different dietary habits or be affected by exposure to various environmental factors. 38
The PD patients included in the meta-analysis were well defined, although they were not identical in terms of demographics and clinical symptoms, and this variability might be a possible confounder. To avoid this bias, we performed multivariate analyses to reveal possible effects due to difference in the age, ethnicity, sex distribution, or family history of PD patients and healthy subjects. None of these potential confounders seem to influence the results of the analyses. The effects of BDNF on cognitive processes are well known 39 ; therefore, we performed a meta-regression to examine the association between the BDNF G196A polymorphism and PD in patients with and without impaired cognitive abilities. Summarizing the clinical data available in six studies, we found no correlation between the BDNF G196A genotype and cognitive impairment. Heterogeneity is a potential problem that might have affected the interpretation of the results, even though it was not significant. In addition, funnel plots and Egger tests did not find potential publication bias. Results from sensitivity analysis and cumulative meta-analysis suggested high stability and reliability of our results.
In conclusion, this meta-analysis revises the previous incomplete data and supports the lack of association between the BDNF G196A polymorphism and the risk of PD.
Footnotes
Acknowledgments
R.S. thanks the National Research Council Aging Program 2012–2014; MIUR Cod. 1182/Ric/V o prot. 2010SH7H3F Functional connectivity and neuroplasticity in physiological and pathological aging [ConnAge]; FISM–Fondazione Italiana Sclerosi Multipla Cod.2011/R/32 Fatigue Relief in Multiple Sclerosis by transcranial Direct Current Stimulation (tDCS): Can we Differentiate stimulation Targets within the primary sensorimotor cortices? [FaReMuS DiCDiT]; and Ministry of Health Cod. GR-2008-1138642 Promoting recovery from Stroke: Individually enriched therapeutic intervention in Acute phase [ProSIA]; Ricerca Corrente, Italian Ministry of Health.
Author Disclosure statement
No competing financial interests exists.