
Abstract
The autoimmune diseases are among the 10 leading causes of death for women and the number two cause of chronic illness in America as well as a predisposing factor for cardiovascular diseases and cancer. Patients of some autoimmune diseases have shown a shorter life span and are a model of accelerated immunosenescence. Conversely, centenarians are used as a model of successful aging and have shown several immune parameters that are better preserved and lower levels of autoantibodies. The study reported here focused on clarifying the connection between longevity and some autoimmune and allergic diseases in 29 developed Organisation for Economic Co-operation and Development (OECD) countries, because multidisciplinary analyses of the accelerated or delayed aging data could show a distinct relationship pattern, help to identify common factors, and determine new important factors that contribute to longevity and healthy aging. The relationships between the mortality rates data of multiple sclerosis (MS), rheumatoid arthritis (RA), asthma, the incidence of type 1 diabetes (T1D) from one side and centenarian rates (two sets) as well as life expectancy data from the other side were assessed using regression models and Pearson correlation coefficients. The data obtained correspond to an inverse linear correlation with different degrees of linearity. This is the first observation of a clear tendency of diminishing centenarian rates or life expectancy in countries having higher death rates of asthma, MS, and RA and a higher incidence of T1D in children. The conclusion is that most probably there are common mechanistic pathways and factors affecting the above diseases and at the same time but in the opposite direction the processes of longevity. Further study, comparing genetic data, mechanistic pathways, and other factors connected to autoimmune diseases with those of longevity could clarify the processes involved, so as to promote longevity and limit the expansion of those diseases in the younger and older population.
Introduction
A
Among environmental factors implicated in the development of rheumatoid arthritis (RA), smoking showed the strongest association. 7 Disease clusters of T1D in children implied the involvement of factors such as infectious diseases and environmental contamination. 8 A significant correlation was found between childhood T1D incidence rates within Europe during the period 1989–1994 and indicators of national prosperity, such as infant mortality (a negative correlation) and gross domestic product (a positive correlation). 9 The most prominent evidence regarding the association between environment and autoimmunity has been reported in systemic lupus erythematous, rheumatoid arthritis, systemic sclerosis, and T1D. 10 Concerning the research on genetic factors, a recent genome-wide study in more than 100,000 people of European and Asian descent 11 discovered 42 new sites of genetic variation involved in risk for RA, bringing the catalogue of confirmed risk variants for RA to over 100 genetic loci. A striking degree of genetic sharing among the autoimmune diseases has been found 12 in DNA changes located outside the genes. Multiple DNA changes worked together to affect genes, leading to autoimmune diseases including RA, Crohn's disease, celiac disease, multiple sclerosis (MS), lupus, and colitis. For each disease, multiple different genes were manipulated by several small differences in DNA. Mutations in human sirtuins (SIRT1), best known for their role in aging, were recently found to cause a familial form of autoimmune diabetes. 13
Immune aging is known to result in a decline of the protective immune responses, leading to an increased incidence of infections, autoimmune diseases, and cancer. Studies have shown that changes in the immune system during aging affect the onset of autoimmune diseases. 14 Many autoimmune diseases occur preferentially in the second half of adulthood when immune competence has declined and thymic T cell generation has ceased. The defense mechanisms in the adaptive immune system primarily consist of T and B lymphocytes, which can respond to specific antigens and subsequently acquire an immunological memory. Cells of the adaptive immunity that respond to self-antigens are termed “autoimmune cells.” Although autoimmune T cells exist in all healthy individuals, they are frequent in the elderly, in whom autoimmune diseases are rare due to various mechanisms that constantly regulate the activity of autoimmune cells. A type of immune cells that drive many autoimmune diseases are helper Th17 cells. 2,15 B cells can also express antibodies reacting against the body and subsequently act as drivers of pathogenesis in autoimmune diseases. 16
Manipulating Foxp1 protein activity, a key controller of our immune system, as a negative regulator of the differentiation of helper T cells provides a useful pathway for suppressing those cells and treating autoimmune disorders. 17 Some investigators have suggested that the role of gender 18 in the regulation of longevity may be linked to gender-specific genetic differences. The factors that affect the development of autoimmune diseases and the regulation of longevity may share common mechanistic pathways. Other factors that may play a role include telomere and telomerase and changes in mitochondrial DNA. Inflammatory and regulatory pathways such as insulin/insulin-like growth factor (IGF) signaling and target of rapamycin (TOR) signaling may also play a role in longevity and aging-related diseases. 18
Centenarians, on the other hand, are used as a model of successful aging where several immune parameters are found to be better preserved. 19,20 Centenarians are known to show very low levels of organ-specific autoantibodies. 21,22 Data on RA and MS and very recently on autoimmune T1D 23,24 have shown that the patients have a shorter life span and life expectancy and could be used as a model of accelerated immunosenescence. 25 The complex interactions between genetics, environmental, economic, and other factors on ageing, longevity, and immune system diseases have been studied extensively. 26 –30
To clarify the connection between longevity and some autoimmune diseases and find further suggestions of common mechanistic pathways and factors influencing both processes, I report here results on the relations between longevity parameters (centenarian rates and life expectancy) and data on some autoimmune and allergic diseases.
Methods
As an indicator of longevity, the centenarian rates (CR) (50–54) were used calculated for the year 2010 (CR*) by dividing the number of the centenarians in 201029 with the number of people aged 50–54 in 1960, multiplied by 10,000 as well as the CR (50–54) for 2011, data already calculated by other authors. 29 The CR enabled the control of migration and infant mortality on the population numbers. The CR and LE data of 29 Organisation for Economic Co-operation and Development (OECD) countries were compared with the data 31 –34 on the age-standardized death rates of RA, MS, asthma, 33 and the incidence 31 of T1D in children ages 0–14. The data with the numbers in thousands of living centenarians or with other ages during the period 1950–2010 were taken from the last United Nations data. 35 The life expectancy (LE) data, corresponding to year 2014, were found in the CIA World Factbook. 36 Some countries have been excluded from the CR (50–54) analyses because of insufficient information regarding the CR (50–54) or when the number of centenarians was equal to zero (in thousands) or too low to permit reliable calculations.
To examine the associations, multiple regression models were used and the Pearson correlation coefficients were determined for the relationships between the two sets of CR (50–54), the LE data, and the data of the above four diseases. In addition a search on MEDLINE and PubMed was conducted for articles published during the last few years using the combinations of “autoimmune,” “aging,” “longevity,” “centenarians,” and the terms “autoimmune disease,” “type 1 diabetes,” “MS,” “asthma.” and “RA,” where a total of more than 200 studies were identified; more than 30 articles have been referred to in this study.
Results and Discussion
Data were collected on the incidence or the death rates of T1D,31,32 RA, MS, and asthma 33,34 of 29 developed Organisation for Economic Co-operation and Development (OECD) countries. These data were compared with two sets of data on centenarian rates, which represent the rate of living centenarians per 10,000 inhabitants of a country: One set CR was found in the literature 29 and another set of centenarian rates, CR*, was calculated on the basis of the last published United Nations population data. 35 To make calculations possible and limit the error, only countries with more than 1000 living centenarians were included (Table 1).
This is the first observation of a clear tendency of diminishing CR in countries having a higher incidence of T1D in children aged 0–14 years and higher death rates of MS, RA, and asthma. The associations between the mortality rates or incidence of those diseases and the CR (50–54) were assessed using regression models and Pearson correlation coefficients. They all corresponded to an inverse correlation with different degrees of linearity, disappearing in some cases (RA with the set CR*) and with Pearson correlation coefficients between the CR (50–54) or CR* (50–54) and MS (r = −0.37 and r* = −0.38), T1D (r = −0.33 and r* = −0.16), asthma (r = −0.34 and r* = −0.30), and RA (r = −0.24). The lower the incidence of T1D or the lower the mortality rates of MS, asthma, and RA, the higher are the centenarian rates, representing the numbers of the living centenarians in the country (Figs. 1 and 2). The United Nations and the WHO advise high prudency when comparing data originating from different countries. It has often been stated in reports that the growing invalidity and high incidence of autoimmune diseases in the developed countries are due to the growing life expectancy and the total aging of the population.
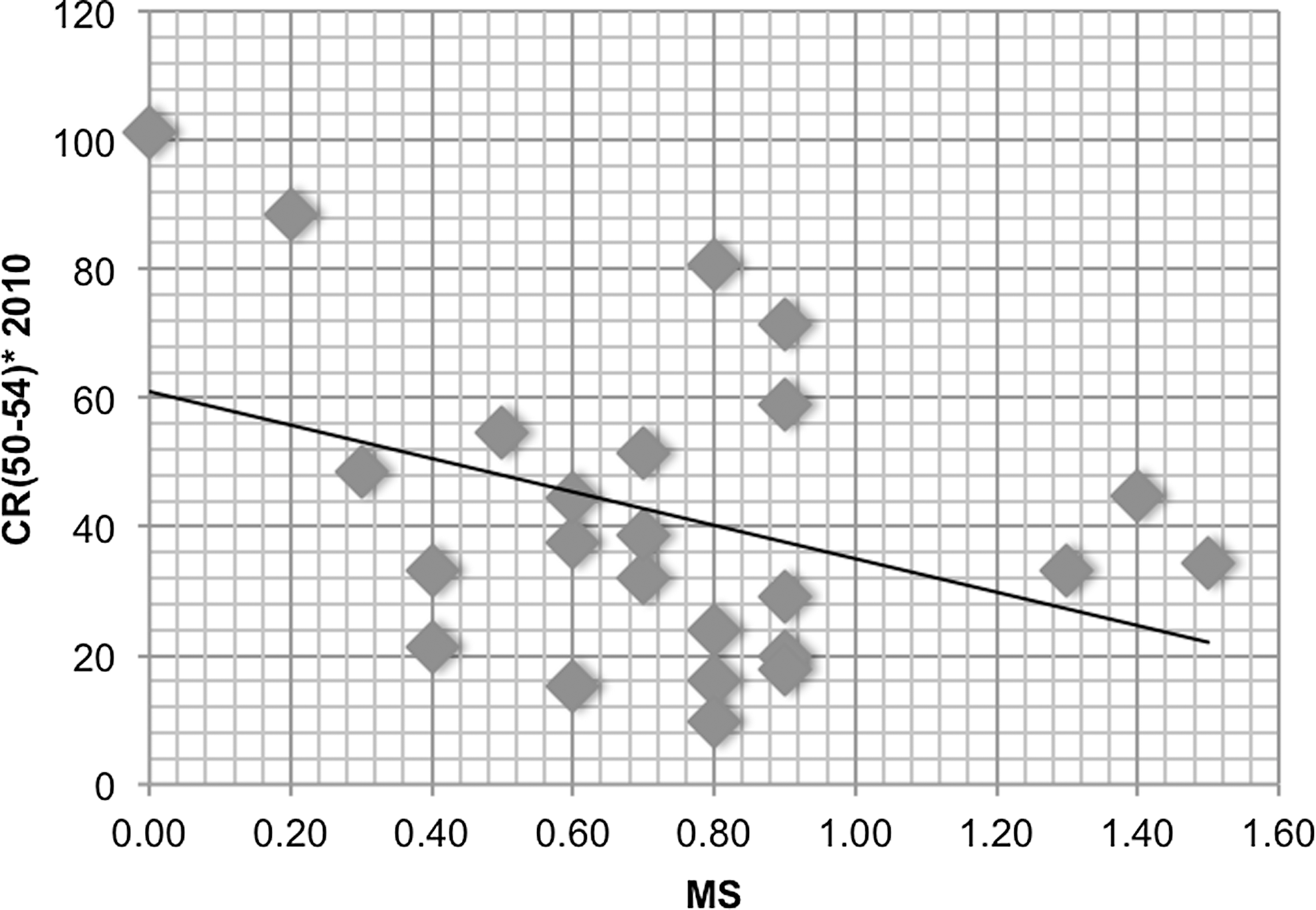
The scatterplots of the death rates of multiple sclerosis (MS) for the centenarians rates (CR*) (50–54) in 24 Organisation for Economic Co-operation and Development (OECD) countries. (x axis) Estimated death rates of multiple sclerosis per 100,000 population; (y axis) centenarian rates CR(50–54)* (2010).
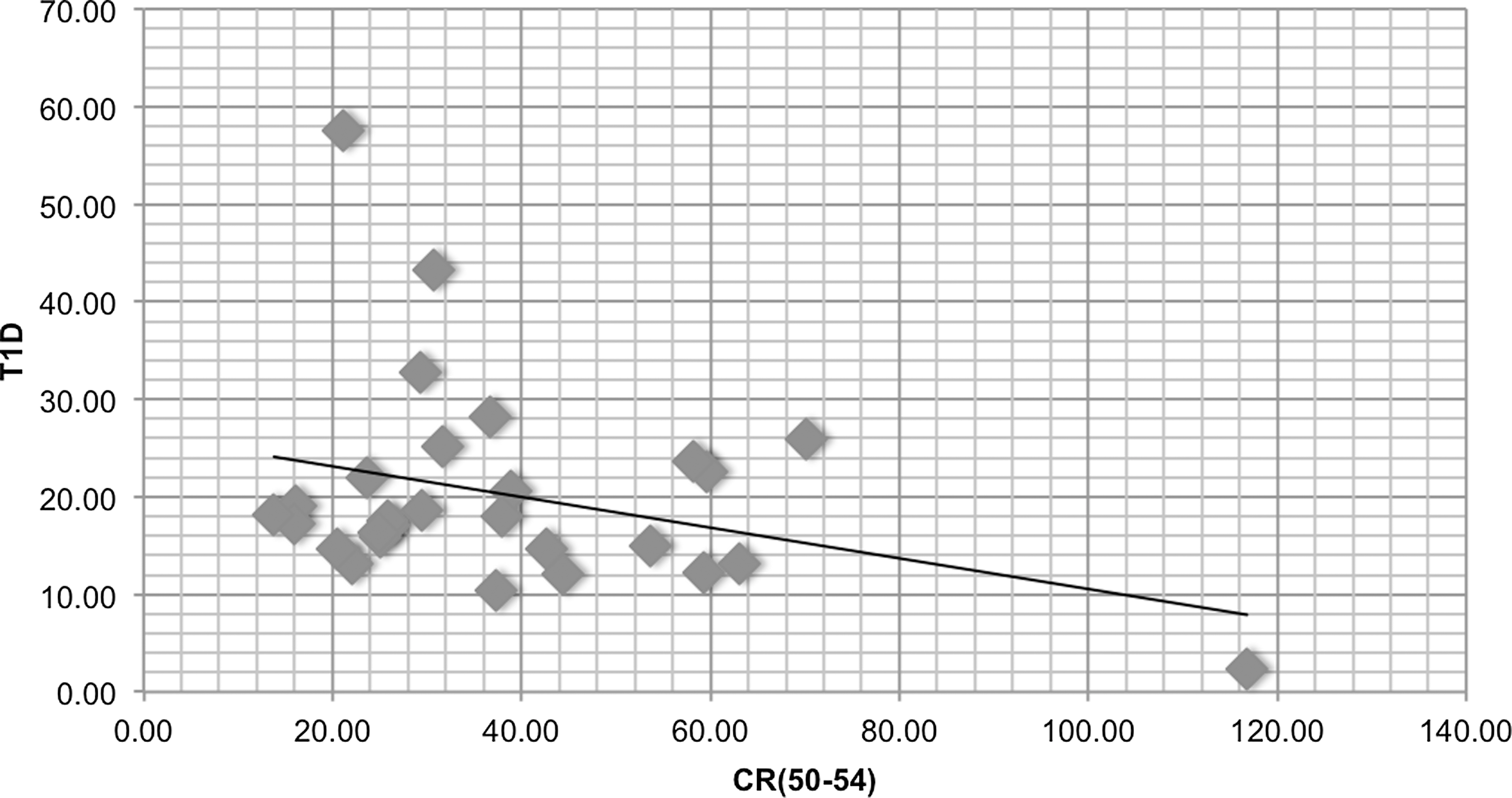
The scatterplots of the incidence of type 1 diabetes (T1D) for the centenarians rates (CR) (50–54) in 29 Organisation for Economic Co-operation and Development (OECD) countries. (x axis) Centenarian rates CR (50–54) 29 ; (y axis) incidence T1D (0–14 years old) per 100,000 population.
To clarify further the connections between longevity and these diseases and confirm the negative correlations observed, data of another parameter of longevity, the countries' LE, 36 were collected. The regression models on the data of the above 29 countries and the same diseases (T1D, MS, RA, and asthma) were applied. Again, an inverse linear correlation between the life expectancy and the death rates was observed with a strong linearity and Pearson coefficients of asthma (r° = −0.63), RA (r° = −0.33), and MS with a lower degree of linearity (r° = −0.15) and a practically non-existent linear relationship with the incidence of T1D data. The observed negative correlations also indicate that the higher the death rates of asthma, RA, and MS in a country, the lower is the country's life expectancy (Figs. 3 and 4). On the basis of these results, the expansion of these diseases is not positively connected to the growing life expectancy, and we do not necessarily have to pay the price of more invalidism if we live longer, as has often been stated.

The scatterplots of the death rates of rheumatoid arthritis (RA) for the life expectancy (LE) in 29 Organisation for Economic Co-operation and Development (OECD) countries. (x axis) Estimated death rates of RA per 100,000 population; (y axis) LE.

The scatterplots of the death rates of asthma for the life expectancy (LE) in 29 Organisation for Economic Co-operation and Development (OECD) countries. (x axis) LE; (y axis) estimated death rates of asthma per 100,000 population.
The worst correlated points and highest values of diseases' data correspond to the data of Finland (for T1D and RA), of Denmark and Norway (MS), countries for which other authors have attributed the high incidence of some autoimmune diseases to their genetic profile, whereas for asthma they correspond to the data for Turkey and Estonia. The differences in the longevity parameters in neighboring countries, which supposedly have similar genetic profiles and environment, as well as the lower degree of linear relation observed in some cases, could point to the importance of other factors (life style, social, economic, etc.) and to complex interactions of several factors influencing the processes of the diseases and the longevity in different degrees and in the opposite direction.
The observed negative correlation between the longevity parameters from one side and the diseases that have been studied here from the other side could suggest common mechanisms and factors affecting the development of those autoimmune diseases, previously rarely studied in a group. The same mechanisms and factors most probably play a role in the processes of aging, longevity, and preserving the centenarians' optimal immunity. Comparing the genetic variations involved in the risks of obtaining these diseases or their mechanistic pathways with the genetic variations found in centenarians or the mechanistic pathways connected to healthy aging and longevity could throw new light on these processes and be a subject of further investigation
Conclusions
There is a clear inverse relation, described here for the first time, between the centenarian rates and the life expectancy as indicators of longevity from one side and the death rates of MS, RA, asthma, and the incidence of T1D in children aged 0–14 in 29 developed OECD countries from the other side. The expansion of the diseases studied here certainly has a negative influence on longevity (LE and CR) by eliminating the possibility of survival or as a predisposing factor for other deadly diseases. There are most probably common mechanistic pathways and factors that affect the development of MS, T1D, RA, and asthma and in the opposite direction the processes of aging and longevity. Further integrated multidisciplinary study comparing genetic data, mechanistic pathways, and other factors connected to autoimmune diseases with those of longevity could clarify the processes involved to promote longevity and healthy aging and limit the expansion of those diseases in the younger and older population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.