
Abstract
A decline in physical and/or cognitive function is a common feature of aging, and frailty has been shown to be associated with cognitive impairment and dementia. This study aimed to evaluate the association between dynapenia, sarcopenia, and cognitive impairment among community-dwelling older people in Taiwan. Data from the I-Lan Longitudinal Aging Study (ILAS) were retrieved for study. Global cognitive function was assessed by Mini-Mental State Examination (MMSE), whereas the Chinese Version Verbal Learning Test, Boston Naming Test, Verbal Fluency Test, Taylor Complex Figure Test, Digits Backward Test, and Clock Drawing Test were used to assess different domains of cognitive function. Association between sarcopenia and global cognitive function as well as all different dimensions of cognitive function were evaluated. Data from 731 elderly participants (mean age 73.4 ± 5.4 years, 53.8% males) were used for study analysis. The overall prevalence of sarcopenia was 6.8%, which was significantly higher in men (9.3% versus 4.1%, p < 0.05). The mean MMSE score was 23.4 ± 4.4 for all participants, and 10.3% of the study participants were cognitively impaired. Sarcopenia was not significantly associated with global cognitive function (odds ratio [OR] = 1.55, p = 0.317), but global cognitive impairment was significantly associated with low physical performance (OR = 2.31, p = 0.003) and low muscle strength (OR = 2.59, p = 0.011). Nonetheless, sarcopenia was significantly associated with impairment in the verbal fluency test (OR = 3.96, p = 0.006) after adjustment for potential confounders. Dynapenia was significantly associated with cognitive impairment in multiple dimensions and global cognitive function, but sarcopenia was only associated with an impaired verbal fluency test. Reduced muscle strength and/or physical performance related to non-muscle etiology were strongly associated with cognitive impairment. More longitudinal studies are needed.
Introduction
A
It has been reported that neurocognitive degeneration is a core feature of aging, 10 especially dementia. Dementia affects more than 6% of people and over 22% of people aged 85 years and older worldwide, 11 which may result in great health care challenges internationally. 12 The number of people with dementia is estimated to double every 20 years, which may cause an exponential growth in health care expenditure. 13 In addition to conventional risk factors of dementia, declining physical function provides additional effectiveness in predicting the occurrence of dementia. 14 On the other hand, neuromuscular deterioration, hormonal dysfunction, decreased physical activities, inadequate protein intake, and chronic inflammation are all potential patho-etiological factors for sarcopenia. 15 Because dementia and sarcopenia share many common risk factors, such as immune or inflammatory response, oxidative stress, and hormonal dysregulation, 16 cognitive impairment and sarcopenia may be highly interrelated. A number of studies have evaluated the potential association between sarcopenia and cognitive impairment, but no conclusion could be reached. 17 Therefore, the main aim of this study was to evaluate the potential association between sarcopenia and impairment of different cognitive domains through a community-based aging cohort study in Taiwan.
Methods
Study subjects
The I-Lan Longitudinal Aging Study (ILAS) is a community-based aging cohort study in Taiwan that explored the complex interrelationship between aging, frailty, sarcopenia, and cognitive decline. 18 People living in the Yuanshan Township of I-Lan County in Taiwan aged 50 years and older were randomly sampled and invited by mail or telephone. The response rate was 70%. A total of 1839 people were recruited, and subjects with any of the following conditions were excluded: (1) Instability to communicate to complete an interview; (2) functionally dependent, i.e., unable to walk for 6 meters within a reasonable period of time; (3) limited life expectancy (less than 6 months) due to major illnesses; (4) currently institutionalized; and (5) contraindicated for brain magnetic resonance imaging. The study was approved by the Institutional Review Board of Taipei Veterans General Hospital and National Yang Ming University. In this study, data were retrieved from the first wave of the study cohort for cross-sectional analysis. Data were obtained from 761 participants aged 65 years and older, and data from 30 participants were excluded due to incomplete data (Fig. 1).
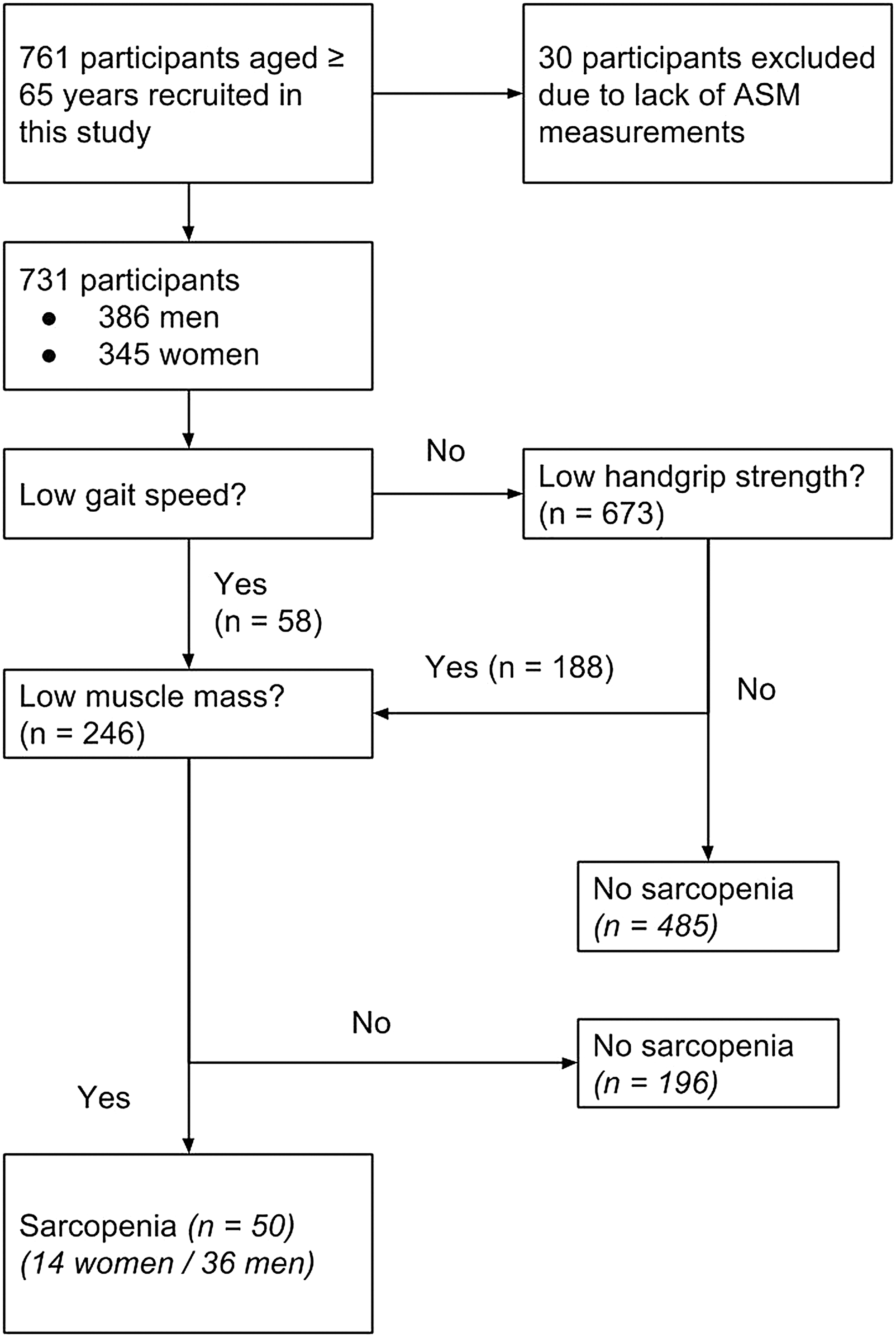
Flow diagram depicting the study population by using criteria of the Asian Working Group for Sarcopenia. ASM, appendicular skeletal muscle.
Demographic data and functional assessment
Demographic characteristics of all participants, including age, gender, height and weight, and body mass index (BMI) were obtained for analysis. Past medical history and personal health behavior were all carefully recorded. Blood sampling after overnight fasting was performed for all study subjects. The activities of daily living were assessed by the Functional Autonomy Measurement System (SMAF). 19 Mood condition was evaluated by Center for Epidemiologic Studies Depression Scale (CES-D), where a score for 16 points or more was considered depressive. 20 Physical activities was evaluated by using the International Physical Activity Questionnaire–Short Form (IPAQ-SF), and high-level physical activity was defined as at least 3000 metabolic equivalent of task (MET)-minutes per week. 21
Muscle mass measurement
In this study, all participants received whole-body dual-energy X-ray absorptiometry (DXA) scans to obtain total fat mass, percentage of fat-free lean body mass (LBM), and bone mineral density using the standardized procedures of the period calibrated manufacturers (GE Lunar, Madison, WI, and DPX-NT, Madison, WI). 22 The mean of coefficient of variation of daily quality assessment within the study period was 0.37%. Height-adjusted relative appendicular skeletal muscle (RASM) was used for diagnosis of sarcopenia. 8
Muscle strength and physical performance measurement
The handgrip strength of the dominant hand was measured using a dynamometer (Smedlay's Dynamo Meter; TTM, Tokyo, Japan) to assess muscle strength. Participants were allowed a pre-test trial in an upright standing position with arms straight down at their sides. All participants were instructed to hold the dynamometer with a dominant hand without squeezing their arms to the body. The best performance was taken for analysis. 23 Physical performance was evaluated by a 6-meter walk. Participants walked straight for 6 meters, and the time they spent was measured by a skilled staff using the same stopwatch (HS-70W, Casio Computer Co. LTC, Tokyo, Japan). 24
Diagnosis of sarcopenia
Sarcopenia was diagnosed based on the diagnostic criteria of the AWGS. Low muscle mass was defined as RASM lower than 7.0 kg/m2 for men and 5.4 kg/m2 for women, respectively. Low muscle strength was defined as handgrip strength less than 26 kg for men and less than 18 kg for women, and slow gait speed was defined as being lower than 0.8 meters/sec. 25
Cognitive function
In this study, global cognitive function was evaluated by the Mini-Mental State Examination (MMSE). 26 Cognitive impairment was defined on the basis of the education-adjusted cutoffs of MMSE scores—less than 16 points for the illiterate, less than 21 points for those had 6 years of education or less, and less than 24 points for those had more than 6 years of education. 27 Other dimensions of cognitive function were assessed by using the Chinese Version Verbal Learning Test (CVVLT), Boston Naming Test (BNT), Verbal Fluency Test (VFT), Taylor Complex Figure Test (CFT), Digits Backward Test (DB), and Clock Drawing Test (CDT). Cutoff points were determined by their age and education level-categorized norm, and impairment was defined as 1.5 standard deviations (SD) lower than the average in each category.
The CVVLT was modified from the California Verbal Learning Test, which was focused on the memory domain of cognitive function. 28 The CFT was used to assess the memory domain and visuoconstructive ability. The DB test was used to assess attention domain, and the BNT was used to evaluate language ability. The VFT was used to assess both executive function and language ability, while the CDT was used to assess memory and visuoconstructive and executive function.
Statistical analysis
Data of continuous variables were expressed as mean ± SD, and categorical data were expressed as numbers and percentage. All of the statistical analysis was performed by commercial software (SPSS 16.0, Chicago, IL). Comparisons of continuous variables were performed by Student's t-test or Mann–Whiney U-test, and comparisons of categorical variables were done by the chi-squared test or Fisher's exact test when appropriate. The association between sarcopenia and cognitive impairment was evaluated by logistic regression, and impairment in global cognitive function and each cognitive function test was regarded as a dependent variable. Age, gender, and all variables with a p value <0.10 in univariate analysis were entered for regression model. For all tests, a two-tailed p value <0.05 was considered statistically significant.
Results
Among 761 elderly participants, data of 30 participants were excluded for analysis due to incomplete data. Data of the remaining 731 participants (mean age: 73.4 ± 5.4 years, 52.8% males) were used for analysis. Table 1 summarizes the demographic characteristics of all study participants. The mean RASM of the study participants was 6.3 ± 0.7 kg/m2 for women and 7.6 ± 0.8 kg/m2 for men. The mean gait speed for all the participants was 1.3 ± 0.4 meters/sec; 58 (7.9%) people were considered having slow gait speed. The mean handgrip strength was 19.0 ± 5.1 kg for women and 30.3 ± 7.1 kg for men; the prevalence of weakness was 25.4% men (n = 98) and 38.0% in women (n = 131). On the basis of the AWGS criteria, 50 people (36 men and 14 women) were considered as having sarcopenia (Fig. 1). The overall prevalence of sarcopenia was 6.8% in this study, which was higher in men (9.3%) than in women (4.1%).
Activity cutoff point: 3000 metabolic equivalent of task (MET)-min/week.
Adjusted by education.
According to Consensus Report of the Asian Working Group for Sarcopenia.
p value <0.05.
p value <0.01.
p value <0.001.
IPAQ-SF, International Physical Activity Questionnaire–Short Form; SMAF, Functional Autonomy Measurement System; CES-D, Center for Epidemiologic Studies Depression Scale; MMSE, Mini-Mental Status Examination; ASM, appendicular skeletal muscle mass; RASM, relative appendicular skeletal muscle mass.
Table 2 summarizes comparisons between subjects with and without sarcopenia. A total of 50 (6.8%) participants were classified as having sarcopenia by definition of the AWGS. Compared to non-sarcopenic participants, sarcopenic subjects were significantly older (76.7 ± 5.3 years vs. 73.1 ± 5.4 years, p < 0.001), male predominant (72.0% vs. 51.4%, p = 0.005), had lower cognitive function (MMSE scores: 21.3 ± 5.3 vs. 23.5 ± 4.3, p = 0.001), and a higher Charlson's co-morbidity index (2.1 ± 1.4 vs. 1.6 ± 1.4, p = 0.012). The sarcopenic subjects were less physically active (7661.3 ± 2932.7 vs. 9669.7 ± 4295.8 MET-min/week, p < 0.001), were more depressed (8.0% vs. 2.6%, p = 0.032), had lower BMI values (21.6 ± 2.7 vs. 24.9 ± 3.5, p < 0.001), and were more likely to consume alcohol (38.0% vs. 24.8%, p = 0.040). Moreover, sarcopenic participants were more likely to have cognitive impairment (22.0% vs. 9.4%, p = 0.005).
All presented as mean ± standard deviation or number (percentage).
According to Consensus Report of the Asian Working Group for Sarcopenia.
Adjusted by education.
Activity cutoff point: 3000 metabolic equivalent of task (MET0-min/week.
CESD cutoff point, ≥16 points.
p value <0.05.
p value <0.01.
p value <0.001.
MMSE, Mini-Mental Status Examination; IPAQ-SF, International Physical Activity Questionnaire–Short Form; SMAF, Functional Autonomy Measurement System; CES-D: Center for Epidemiologic Studies Depression Scale.
Results of univariate analysis showed a significant association between sarcopenia and global cognitive impairment (odds ratio [OR] = 2.72, 95% confidence interval [CI] 1.33–5.57, p = 0.006), and the association remained significant after adjustment for age and gender (OR = 2.27, 95% CI 1.07–4.86, p = 0.033). However, the association became insignificant in a multiple logistic regression model when other potential confounding factors entered the model (OR = 1.50, 95% CI 0.64–3.49, p = 0.352). MMSE-defined global cognitive impairment was independently associated with weakness (OR = 2.23, 95% CI 1.29–3.86, p = 0.004) and slowness (OR = 2.60, 95% CI 1.25–5.40, p = 0.011), which suggested the association of cognitive impairment and muscle performance. For other dimensions of cognitive function, impaired verbal function was significantly associated with sarcopenia (OR = 3.84, 95% CI 1.46–10.10, p = 0.006). Slowness was significantly associated with impairments of most cognitive dimensions, except VFT and DB. Weakness was significantly associated with poorer performance in MMSE, VFT, and DB (p all <0.05). However, low muscle mass with not associated with impairment of each individual cognitive function test after adjustment of confounding factors (Table 3). Sub-group analysis showed no interaction between gender and sarcopenia (not shown in table).
Mode1 1, no adjustment; Model 2, adjusted by age and gender; Model 3, adjusted by age, gender, body mass index, alcohol drinking, Charlson Co-morbidity Index, International Physical Activity Questionnaires–Short Form, Functional Autonomy Measurement System, and Center for Epidemiologic Studies Depression Scale.
Adjusted by education.
Adjusted by age and education.
p value <0.05.
p value <0.01.
p value <0.001.
OR, odds ratio; CI, confidence interval, presented as lower limit–upper limit;
MMSE, Mini-Mental Status Examination; CVVLT, Chinese Version Verbal Learning Test; BNT, The Boston Naming Test; VFT, Verbal Fluency Test; CFT, Taylor Complex Figure Test; DB, Digits Backward Test; CDT, Clock Drawing Test.
Discussion
The prevalence of sarcopenia among community-dwelling people in Taiwan ranged from 7.1 to 30.9%. 29 In this study, the prevalence of sarcopenia was 6.8% by using the AWGS diagnostic criteria. 25 The low prevalence of sarcopenia in this study may be related to the extraordinarily high physical activities of the subjects because the majority of the study participants were still active working farmers. Nevertheless, the education level–adjusted prevalence of cognitive impairment was 10.3%, which was higher in international studies 13 and a previous study in Taiwan. 30
The low educational level of older people living in the agricultural communities is common in Taiwan. Our previous work showed that sarcopenia was significantly associated with lower MMSE among men aged 80 years and older. 31 However, results of the EPIDOS study did not support the association between sarcopenia and cognitive impairment. 32 Compared to previous studies, our study participants were relatively younger, having remarkably higher physical activities, lower prevalence of sarcopenia, and better cognitive performance, which may explain the negative association between sarcopenia and global cognitive performance. However, the association of global cognitive impairment with weakness and slowness were compatible with previous studies. Low muscle mass was not independently associated with any cognitive impairment, whereas slowness was associated with impairment in VFT and DB and weakness was associated with VFT, DB, and MMSE. It has been proposed that dynapenia, age-associated loss of muscle strength, was mostly attributed to nerve or muscle etiology. 4 Results of this study imply that dynapenia of neurological etiology may be strongly associated with cognitive decline and even subsequent dementia.
Among the cognitive tests, only impairment in VFT was significantly associated with sarcopenia as well as dynapenia. VFT was used to screen dementia and mild cognitive impairment with a special focus on executive function and language ability. 33 Abnormal VFT may indicate the presence of cognitive impairment 5 years before the clinical diagnosis of dementia. 34 Poorer VFT performance may represent impairment of executive function, which was often related to frontal lobe dysfunction and possibly a sign of mild cognitive impairment or early dementia. 35 Also, language disability may be related to the dysfunction of the temporal cortex. Previous studies have shown that muscle quantity was associated with gray matter volume, especially the prefrontal and temporal areas, 36 and the smaller prefrontal area was related to slower gait speed. 37 Moreover, the strong association between cognitive impairment and white matter lesions has been reported, 38 and VFT was considered the best cognitive test to evaluate cognitive impairment related to white matter lesions. 39 Moreover, white matter volume has been reported to be associated with muscle mass and physical performance. 40 Altogether, the sarcopenia-related cognitive impairment was mainly in executive function and may be associated with dysfunction of frontal and temporal lobes and/or white matter lesions. This association might interact bi-directionally or occur concurrently sharing the same etiology.
Several possibilities may link sarcopenia to cognitive impairment of older people. First, the association of executive dysfunction and elevated serum levels of C-reactive protein implies a potential role of chronic inflammation in cognitive impairment, 41 and chronic inflammation also plays an important role in the development of sarcopenia. 15 Second, hormone replacement therapy, especially growth hormone–releasing hormone (GHRH), has been shown to improve cognitive function 42 as well as sarcopenia. 15 This suggests that both cognitive impairment and sarcopenia may share the same hormonal deficits. Third, metabolic dysregulation, such as insulin resistance and diabetes, worsen cognitive function and sarcopenia. 15 Therefore, the development of sarcopenia and cognitive impairment may be mediated through similar patho-etiological factors, and a potential sequential effect may exist.
Despite all the efforts of this study, there were still several limitations. First, the prevalence of sarcopenia was low in this study, which may limit the power of statistical analysis. Second, the study participants were mostly actively working farmers in rural communities, so they were physically active and had extraordinarily higher daily activities than the general population. Therefore, results of this study may not be completely extrapolated to other populations. Third, the educational levels of the study participants were low. Although low educational level was a common condition for Taiwanese elderly in rural communities, 30 the higher prevalence of education-adjusted cognitive impairment of the study participants may be related to their simple lifestyles. Fourth, the sample size in our study was not large enough and thus might underestimate the association between cognitive function and sarcopenia. Last, due to the cross-sectional study design, the causal relationship between sarcopenia and cognitive impairment remains to be determined using longitudinal studies.
To the best of our knowledge, this is the first study to evaluate the association of sarcopenia and various domains in cognitive function. Sarcopenia-related cognitive impairment was mainly in the executive function instead of the global cognitive function. Moreover, dynapenia with non-muscle (nerve) etiology may be a stronger risk factor for cognitive decline in the late life. More longitudinal studies and brain imaging studies are needed to clarify the inter-relationship between aging, sarcopenia, and cognitive impairment.
Footnotes
Acknowledgments
This study was supported by the Aging and Health Research Center, National Yang Ming University, Center for Geriatrics and Gerontology, Taipei Veterans General Hospital, as well as the Ministry of Science and Technology of Taiwan (MOST 103-2633-B-400-002; and MOST 101-2314-B-010-008).
Author Disclosure Statement
No competing financial interests exist.
Author contributions were as follows: C.Y. Huang, data collection, interpretation, and manuscript writing; A.C. Hwang, data analysis and manuscript preparation; L.K. Liu, data collection; W.J., Lee, data collection and manuscript preparation; L.Y. Chen, data collection; M.H. Lin, data interpretation; L.N. Peng, data interpretation; L.K. Chen, study design and manuscript preparation.