
Abstract
Low hemoglobin (Hb) levels are attracting interest as a risk factor for cognitive impairment, but with contrasting evidence emerging from the current literature. The aim of our work was to investigate the relationship between baseline serum Hb levels and the incidence of cognitive impairment in older people over a follow-up of 4.4 years. Our study considered a sample of 1227 elderly subjects cognitively intact at baseline, enrolled under the Progetto Veneto Anziani (Pro.V.A.) among 3099 screened subjects. For all participants, we measured serum Hb levels on blood samples; incident cognitive impairment was defined as a Mini Mental State Examination (MMSE) score <24 and confirmed by geriatricians skilled in psychogeriatric medicine. No differences in baseline MMSE scores across Hb tertiles emerged in either gender. After the 4.4 years of follow-up, we identified 403 new cases of cognitive impairment (147 men and 256 women). Cox's regression analysis showed that participants with the lowest baseline Hb concentrations carried a significant 37% higher risk (95% confidence interval [CI]: 1.08–1.75; p = 0.01) of being diagnosed with cognitive impairment during the follow-up. Considering the gender separately, the risk of cognitive impairment only increased significantly, by 60%, for men in the lowest Hb tertile (95% CI: 1.06–2.41; p = 0.02), but not for women (hazard ratio = 1.32; 95% CI: 0.97–1.79; p = 0.08). In conclusion, low Hb concentrations may predict the onset of cognitive impairment in the elderly, apparently with a stronger association in men than in women.
Introduction
C
Low hemoglobin (Hb) levels are also not unusual in older people and have been analyzed as a factor potentially predisposing to dementia and poor cognitive performance, 11 since this condition seems to promote neuron degeneration. 12 It is difficult to confirm this relationship, however, due to the contrasting findings reported in the literature. Most of the published prospective studies found a significant relationship between low baseline Hb levels and cognitive decline during follow-up periods ranging from 3 to 9 years, 13 –16 but some authors found no such significant association. 17,18 Two studies only considered women 15,18 and consequently could not examine the influence of gender on the relationship between Hb concentrations and cognitive decline.
Men and women seem to have different risk profiles in this setting, 19 as well as the well-known gender-related variability in Hb levels also persists with aging. 20 Moreover, to avoid additional biases, Hb should also be measured at the follow-up because it could change considerably even in the short term, given elderly people's often labile health status.
In our study, we hypothesized that low Hb levels could predict the onset of cognitive impairment in the elderly. The aim of this work was therefore to investigate the association between baseline serum Hb concentrations and the incidence of cognitive impairment over a follow-up of 4.4 years in a cohort of elderly men and women who were cognitively intact at baseline, also considering the possible role of gender.
Methods
Data source and subjects
This work analyzes data obtained with the Progetto Veneto Anziani (Pro.V.A.), an observational cohort study on the Italian population older than 65 years of age. The study population included 3099 age- and sex-stratified white participants (1854 women and 1245 men) randomly selected between 1995 and 1997 using a multistage stratification method. Sampling procedures and data collection methods have been described extensively elsewhere. 21 For the present study, we considered the incidence of cognitive impairment after 4.4 ± 1.2 (mean ± standard deviation [SD]) years of follow-up.
The Local Ethics Committees of Padova University and the Local Health Units (USSL) n. 15 and n. 18 of the Veneto Region approved the study protocol, and participants provided their written informed consent.
Clinical data
Participants were examined at city hospitals by trained physicians and nurses. Information was collected on their educational level, income, physical activity, smoking and alcohol drinking habits, and whether or not they lived alone during a face-to-face interview.
Educational level was classified as ≤5 or >5 years (5 years being the duration of primary school in Italy). Monthly income was assessed considering a cutoff value of 500 €/month. Regular physical activity was defined as ≥4 hours/week in the previous month of at least moderate physical activity (brisk walking, cycling, gardening, dancing, or physical exercising). Smoking status was classified as “never,” “previous” (for at least a year in the past), and “current” smokers. Alcohol drinking (defined as drinking any alcoholic beverage in the previous month) and living alone were both categorized as “yes” versus “no.” Body weight and height were measured by trained physicians, and body mass index (BMI, kg/m2) was calculated.
Several questionnaires were used to assess participants. Functional status and social independence were measured using two validated scales, the Activities of Daily Living (ADL) for the former and the Instrumental Activities of Daily Living (IADL) for the latter. 22,23 Physical performance was estimated with the Short Physical Performance Battery (SPPB), measuring three lower extremity functions (gait speed, static balance, and chair stand time) to obtain a total score ranging from 0 to 12, where higher scores reflect a better physical performance. 24 Depression was assessed with the 30-item Geriatric Depression Scale (GDS), an accurate validated method for rating depressed mood in the elderly, with a score higher than 10 indicating the presence of prevalent depressive symptoms. 25
Participants' clinical status and comorbidities were assessed by board-certified physicians using standardized questionnaires and considering medical history, self-reported symptoms, medical and hospital records, blood tests, and physical examination.
For the purposes of our study, the following diseases were recorded: hearing loss, vision loss, diabetes, cardiovascular diseases (CVD), chronic obstructive pulmonary diseases (COPD), osteoarticular diseases (OAD), cancer, and hypertension. 21 Diabetes was defined as fasting plasma glucose levels ≥7.0 nmol/L, HbA1c ≥6.5%, the use of glucose-lowering drugs, or a history of a 2-hour postload glucose ≥11.1 nmol/L. 26 CVD was defined as any of the following: congestive heart failure, angina requiring a stent, angioplasty or hospitalization, myocardial infarction, and stroke. OAD was defined as hip fracture, osteoporosis or arthritis (of the upper or lower extremities). Hypertension was defined as a systolic blood pressure (BP) ≥140 mm Hg, a diastolic BP ≥90 mm Hg, or the routine use of antihypertensive medication. 27
Definition of exposure and outcome
Complete blood counts were obtained using a colorimetric enzymatic method with an intra- and interassay coefficient of variation (CV) <2%, taking Hb as the main parameter of anemia. Since there was a significant difference in serum Hb levels between genders (p < 0.0001), we divided the sample into gender-specific Hb tertiles using the following cutoffs: 13.9 and 14.9 g/dL for men; and 12.8 and 13.7 g/dL for women.
Cognitive function was assessed at baseline and at the follow-up by administering the 30-item Mini Mental State Examination (MMSE), a validated tool to estimate changes in cognitive status. 28 Scores lower than 24 indicate a cognitive impairment according to the recent literature. 29 Any diagnosis of cognitive impairment was confirmed by geriatricians skilled in psychogeriatric medicine using a standardized questionnaire, and also checking for additional relevant information such as signs and symptoms of cognitive impairment and medical records.
Statistical analyses
All measures assessed at baseline and at the follow-up were used in the data analysis. For continuous variables, normal distributions were tested using the Shapiro–Wilk test. Participants' characteristics were summarized using mean ± SD for continuous variables, and counts and percentages for categorical variables across gender-specific baseline Hb tertiles. Age-adjusted p-values for trends were calculated as follows: for continuous variables, the differences between the means of the covariates across Hb tertiles were analyzed using a general linear model; for categorical variables, logistic regression was applied.
The rate of incident cognitive impairment was calculated as the number of new cases of cognitive impairment per 1000 person-years during the follow-up period. Cox's proportional hazard models were used to assess the associations between baseline Hb levels and incident cognitive impairment. The proportional hazards assumption was checked by plotting the Schoenfeld residuals versus time.
Factors known to be associated with Hb and/or cognitive impairment were considered for inclusion in the analysis. To see whether a variable should be included as a predictor in the final survival model, the log-rank test of equality across strata was performed for all the categorical variables, and Cox's univariate proportional hazards regression for all the continuous variables. The predictors included in the final model were all the variables significantly differing across Hb tertiles in at least one gender, and the variables reaching p < 0.20 in the univariate analyses taking follow-up cognitive impairment as outcome. Collinearity among covariates was estimated with the variance inflation factor (VIF), using a value ≥2 as an exclusion criterion, but no variables were excluded for this reason.
A stepwise selection (backward logistic regression) was performed to obtain the most effective set of variables for predicting the dependent variable. Hazard ratios (HRs) and 95% confidence intervals (CIs) were used to compare cognitive impairment rates across Hb tertiles, taking those in the top tertile (with the highest Hb levels) for reference. p-values for trend across tertiles of baseline Hb concentrations were calculated using the Wald test, taking a score corresponding to the median value of each tertile for reference. A similar analysis was run considering Hb as a continuous variable (for 1 mg/dL or for a 1 SD increase).
All analyses were performed using the SPSS 21.0 for Windows (SPSS, Inc., Chicago, IL). All statistical tests were two tailed and statistical significance was assumed for a p-value ≤0.05.
Results
Figure 1 shows the flowchart of our analysis. Among 3099 participants enrolled in the study, we excluded 1529 with a diagnosis of cognitive impairment already at baseline, 32 whose Hb levels were not measured, 100 lacking follow-up data, and 211 who died during the follow-up, leaving a final sample of 1227 participants (511 M, 716 F) (Fig. 1).
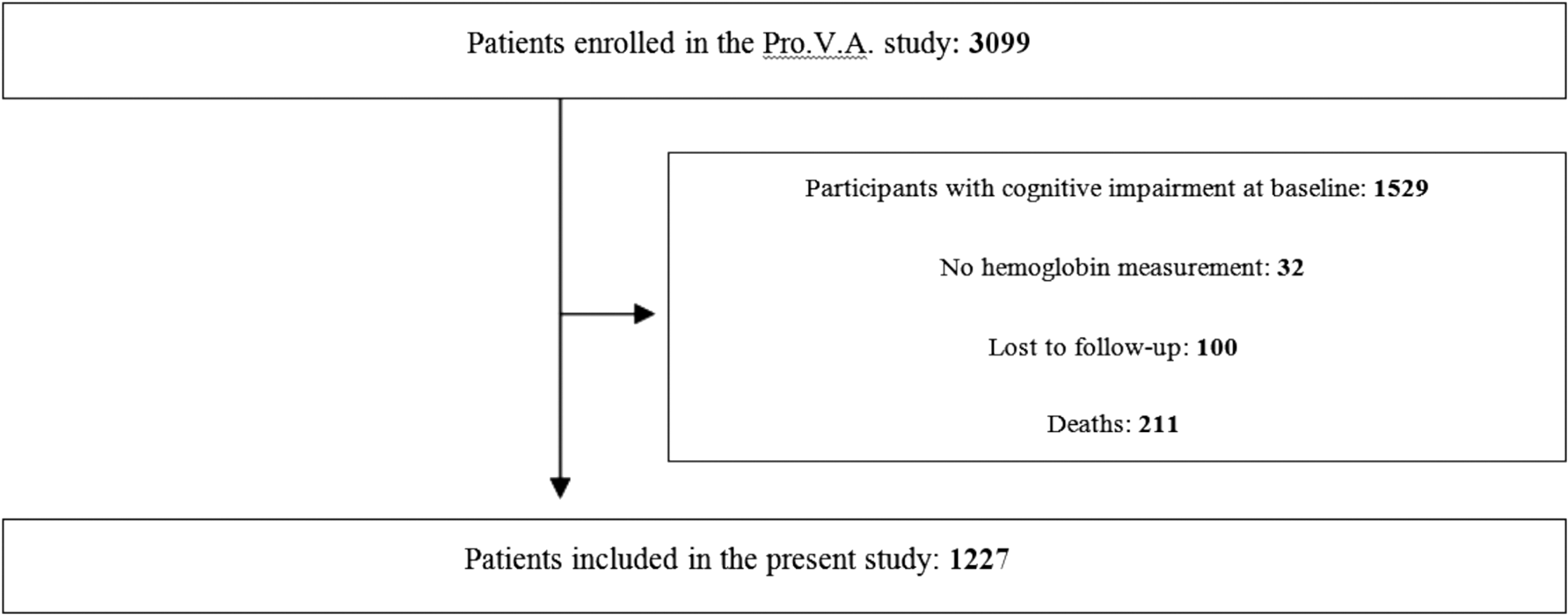
Flowchart for the study.
By comparison with the sample completing follow-up, those who dropped out or died were more likely to be men (58.0% vs. 42.0%; p < 0.0001) and older (76.2 ± 7.1 vs. 72.1 ± 5.7; p < 0.0001). They were also more likely to be diagnosed with diabetes (20.4% vs. 13.3%, p = 0.001), CVD (32.5% vs. 15.3%), COPD (14.3% vs. 7.6%), and cancer (13.4% vs. 5.8%) (p < 0.0001 for all comparisons), while no significant difference emerged for OAD (56.7% vs. 53.1%, p = 0.14). Hb concentrations did not differ between the study sample and the group of dropouts and deceased (13.6 ± 1.5 vs. 13.7 ± 1.3 g/dL, p = 0.82), but the latter had significantly lower MMSE scores (27.1 ± 1.4 vs. 27.5 ± 1.5; p < 0.0001) than those forming our sample.
Baseline characteristics
The sample consisted of 1227 community-dwelling elderly subjects with no cognitive impairment at baseline.
Considering the final sample included in our study, we found that mean age was 72.1 ± 5.7 years [range: 65–96], 58.4% were women, and the mean BMI was 27.9 ± 4.3 kg/m2. The mean baseline Hb was significantly higher in men than in women (14.3 ± 1.3 vs. 13.2 ± 1.1 g/dL; p < 0.0001) and 12.1% of the whole sample was anemic. Among the participants with anemia, 32.2% had a microcytic and 51.7% a hypochromic pattern, using the cutoffs proposed by the World Health Organization. 30,31
Considering the gender-related differences in the Hb trend and the factors influencing the onset of cognitive impairment, we separately analyzed the characteristics of the men (Table 1) and women (Table 2). For both genders, participants with the lowest Hb concentrations had a lower BMI and a lesser prevalence of CVD and diabetes. Among the men, participants in the lowest Hb tertile were significantly older and had a worse educational level (after adjusting for age) than those in the other tertiles (Table 1). Women with higher Hb levels more frequently had smoking and alcohol drinking habits, and presented a higher prevalence of hypertension (Table 2).
Numbers are mean values ± SDs or percentages (%), as appropriate.
Unless otherwise specified, p-values are adjusted for age using a general linear model or logistic regression, as appropriate.
Univariate ANOVA, not adjusted for age.
ADL, Activities of Daily Living; ANOVA, analysis of variance; BMI, body mass index; COPD, chronic obstructive pulmonary diseases; CVD, cardiovascular diseases; GDS, Geriatric Depression Scale; Hb, serum hemoglobin concentration; IADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; OAD, osteoarticular diseases; PRO.V.A., Progetto Veneto Anziani; SD, standard deviation; SPPB, Short Physical Performance Battery.
Numbers are mean values ± SD or percentages (%), as appropriate.
Unless otherwise specified, p-values are adjusted for age using a general linear model or logistic regression, as appropriate.
Univariate ANOVA, not adjusted for age.
ADL, Activities of Daily Living; ANOVA, analysis of variance; BMI, body mass index; COPD, chronic obstructive pulmonary diseases; CVD, cardiovascular diseases; GDS, Geriatric Depression Scale; Hb, serum hemoglobin concentration; IADL, Instrumental Activities of Daily Living; MMSE, Mini-Mental State Examination; OAD, osteoarticular diseases; PRO.V.A., Progetto Veneto Anziani; SD, standard deviation; SPPB, Short Physical Performance Battery.
For the sample as a whole, functional status and mobility scores (as assessed with the ADL, IADL, and SPPB) were close to the maximum values for independency and physical performance, with no significant differences across Hb tertiles (Tables 1 and 2). Depressed mood did not differ by baseline Hb concentration, and the mean scores in the GDS suggested a low presence of depressive symptoms in our cohort. As for comorbidities, no significant differences emerged among the Hb tertiles for vision and hearing loss and oncological or pulmonary diseases (Tables 1 and 2).
Finally, the mean MMSE score in our cohort at baseline was 27.5 ± 1.5, with no significant differences across the Hb tertiles (p for trend = 0.94 for men, 0.15 for women).
Follow-up data
Serum Hb concentrations did not change substantially during the follow-up in the cohort as a whole (p = 0.26, paired t-test), but when the genders were considered separately, they dropped significantly in men (p = 0.001, paired t-test), but not in women (p = 0.11, paired t-test). The mean Hb variation of the sample as a whole was 0.03 ± 1.01 g/L (95% CI: −1.40 to 1.70 g/L), for men 0.16 ± 1.07 g/L (95% CI: −1.40 to 1.94 g/L), and for women −0.06 ± 0.96 g/L (95% CI: −1.40 to 1.50 g/L).
We identified 403 new cases of cognitive impairment (147 M and 256 F) developing during the 4.4 years of follow-up, with a global incidence rate of 80 per 1000 person-years (95% CI: 0–34). Comparing subjects developing and not developing cognitive impairment at follow-up, those with cognitive impairment had significantly higher age (p < 0.0001) and number of women (p = 0.006), and had a higher baseline prevalence of OAD (p = 0.003), but lower ADL (p = 0.01), IADL (p = 0.002), MMSE (p < 0.0001), and total SPPB (p = 0.03) scores.
In the sample as a whole, the incidence of cognitive impairment differed significantly across Hb tertiles, being higher in those with the lowest baseline Hb concentrations (Fig. 2). This finding was confirmed in men, with a higher cognitive impairment incidence rate in the bottom Hb tertile than in the top Hb tertile (70; 95% CI: 0–45 vs. 60; 95% CI: 0–42 per 1000 person-years), but not in women, whose cognitive impairment incidence rate was similar across Hb tertiles (70 per 1000 person-years), as shown in Figure 2.
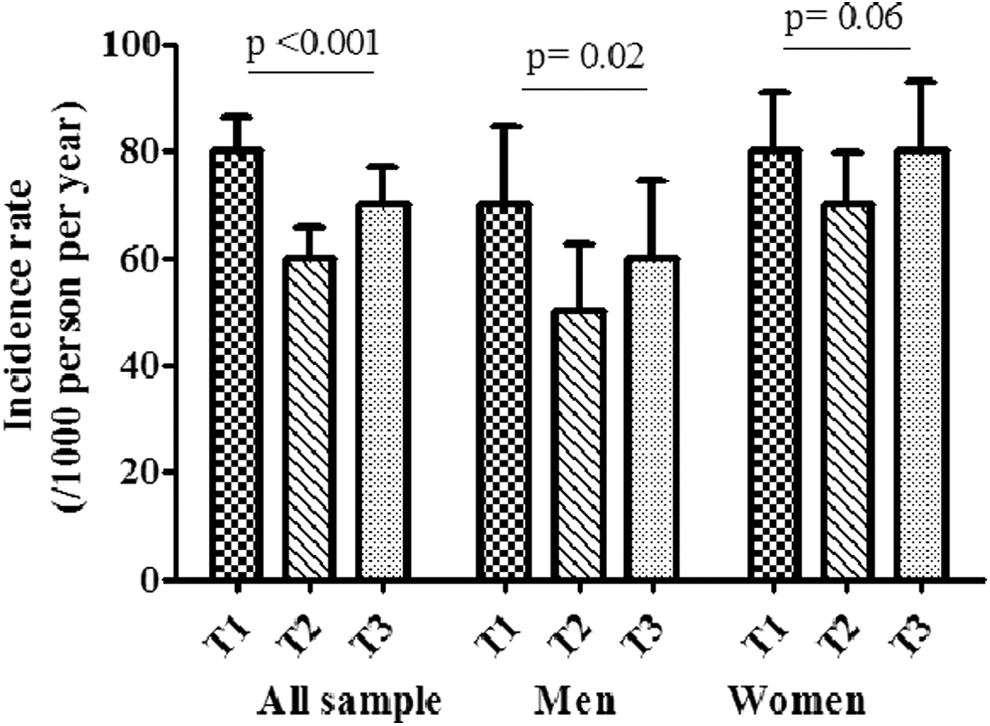
Incidence rate of cognitive impairment with standard error of the mean (SEM) in the sample as a whole and by gender, divided into baseline Hb tertiles. Age-adjusted p-values for trends were calculated using a general linear model across gender-specific Hb tertiles at baseline. Hb, hemoglobin.
Using Cox regression analysis and taking the participants with the highest Hb levels for reference, we observed a significantly greater risk of cognitive impairment developing in subjects with lower Hb concentrations in the sample as a whole (p = 0.01, Table 3), with no differences between genders (p = 0.02 in men and = 0.03 in women). Those in the lowest tertile carried a significant 37% higher risk (95% CI: 1.08–1.75; p = 0.01) of being diagnosed with cognitive impairment during the follow-up. When the genders were considered separately, the significance of this association was apparent for men (HR = 1.60; 95% CI: 1.06–2.41; p = 0.02), but not for women (HR = 1.32; 95% CI: 0.97–1.79; p = 0.08). Figure 3 represents the Cox proportional model for the incident cognitive impairment by Hb tertiles in men (Fig. 3a) and women (Fig. 3b), respectively. When Hb was modeled as a continuous variable, increases of 1 mg/dL in baseline Hb concentrations were associated with a significantly lower risk of the onset of cognitive impairment during the follow-up, but only in the sample as a whole (HR = 0.92; 95% CI: 0.86–0.99; p = 0.02) (Table 3). Finally, considering Hb changes, we found that each 1 mg/dL decrease in Hb levels over the study period reduced the incident impairment of 10% in the sample as a whole, only after adjusting for potential confounders (HR:0.90; 95% CI: 0.82–0.99; p = 0.03) (Table 3).

Cumulative incidence of cognitive impairment divided into baseline Hb tertiles in men
Unless otherwise specified, data are presented as hazard ratios and 95% CIs.
Tertile 1: serum Hb <13.9 g/dL (men), <12.8 g/dL (women). Tertile 2: Hb 13.9–14.9 mg/dL (men), 12.8–13.7 mg/dL (women). Tertile 3: >14.9 mg/dL (men), >13.7 mg/dL (women) (reference group).
Fully adjusted model, including: age, body–mass index (both continuous variables); gender (only for the sample as a whole); diabetes mellitus, CVD, OAD, COPD, cancer, alcohol drinking, hearing loss, living alone (all yes vs. no); smoking status (current vs. previous vs. never); education (≤5 years vs. >5 years); income (≤500 euro vs. 500 euro monthly); physical activity (<4 hours vs. ≥4 hours daily); ADL, IADL, GDS, MMSE, SPPB, and serum hemoglobin concentrations at follow-up (all as continuous variables).
Each p-value was based on a Wald χ 2 test with df = 1.
HR, hazard ratio; CI, confidence interval; SD, standard deviation.
Discussion
In the present study, we found a significant association between baseline Hb concentrations and the onset of cognitive impairment over a 4.4-year follow-up in a cohort of older men and women who were cognitively intact at baseline.
Considering the sample as a whole, participants with the lowest serum Hb levels were generally less exposed to several potential risk factors for cognitive decline, such as smoking or alcohol drinking, poor education, and they had lower rates of hypertension, diabetes, and CVD. Nonetheless, the incidence of cognitive impairment during the follow-up in this group was higher than in the other two tertiles, although baseline MMSE score did not significantly differ among Hb tertiles. This result was in agreement with other studies on the potential predictive role of anemia for the development of cognitive decline. 13 –16
The most convincing hypothesis proposed to explain these findings concerns the more limited oxygenation of peripheral tissues due to lower Hb concentrations. 19 Our findings strongly support this hypothesis since, as mentioned earlier, participants with the lowest baseline Hb values had a significantly lower prevalence of conditions that might lead to small vessel damage, 32,33 thus reinforcing the impression that low Hb levels are per se a potential risk factor of poor cognitive status. Low Hb concentrations might also be a consequence of other pathological conditions, however, such as erythropoietin deficiency or iron homeostasis imbalance, which could enhance oxidative stress and accelerate brain aging. 12,34,35
A significant relationship between baseline Hb concentrations and the incidence of cognitive decline was found in both genders, but this association was stronger in men than in women. This result partially contrasts with other works that reported a stronger association between low Hb levels and poor cognitive status in women than in men, although with some acknowledged biases. 14,17 Analyzing the presence of cognitive decline in older people, two longitudinal studies found a greater prevalence of cognitive impairment and a higher cumulative risk of Alzheimer's disease in women than men. 36,37
The greater weight of low Hb concentrations as a risk factor for cognitive impairment in men may be justified if we consider the time of life when Hb levels tend to drop. As seen in the third National Health and Nutrition Examination Survey, inadequate Hb levels are more common in women of reproductive age until menopause, when the prevalence of anemia falls by half. Conversely, among subjects older than 75 years of age, the prevalence of anemia rises linearly in men and exceeds the prevalence in women. 38
We surmise that, while women's low Hb concentrations for over 50 years might give rise to compensatory pathways to guarantee an adequate peripheral oxygenation, the same would not apply to men. In other words, for the same drop in Hb levels, the fact that it occurs more rapidly in older men than in older women might make it responsible for a more severe neuronal impairment and cognitive dysfunction. In accordance with this hypothesis, we identified a greater decline in Hb levels in men than in women during a 4.4-year follow-up, coinciding with a higher incidence of cognitive impairment in the former.
Nonetheless, considering Hb changes over the study period, we found a weak but significant association between greater decreases in Hb levels and lower incidence of cognitive impairment in the sample as a whole, only after adjusting for potential confounders. However, we supposed that both the short duration of our study and the poor variability of Hb change among participants, as well as a likely Type II error when genders were considered separately, may represent potential biases for the evaluation of the proper role of Hb variations on the development of cognitive impairment. Moreover, our finding may reflect the influence of higher Hb concentrations too, on cognitive status. In fact, a reverse J-shaped curve has been yet demonstrated for the relationship between Hb levels and mortality, 11,39 as well as in the latest years for cognitive decline, 40 likely due to the cardiovascular disorders related to high Hb concentrations and polycythemia.
This study has some limitations that need to be taken into account.
First, since no neuroimaging examinations were performed, it was impossible to precisely establish the cause of any cognitive impairment. Second, we did not consider different etiologies of low Hb levels, but vitamin B12 or folate deficiency, for instance, could be considered as independent risk factors for cognitive impairment. 41 The fact that we had no information on whether any of our participants were treated for anemia during the follow-up may also represent a bias of the study. Moreover, the exclusion of participants died before the follow-up assessment may underestimate the risk of cognitive impairment according by Hb concentrations, since low Hb levels seem to be associated with higher mortality in the elderly. 42 Finally, the timing of the PRO.V.A. study, started between 1995 and 1997, may represent a potential bias due to the latest tools for the identification and treatment of anemia and cognitive impairment.
Nonetheless, since the biological constructs of anemia and cognitive impairment have not essentially modified, we supposed that this bias may not affect the relevance of our study for current practice. In contrast, the fact that we also measured Hb concentrations at the follow-up, as a variable with unpredictable changes, strengthens our results and could reduce the bias existing in other studies on the same topic. Another strength of our work lies in having included both genders in the sample, taking into account the differences between men and women in terms of their Hb concentrations and any onset of cognitive impairment. The considerable number of covariates included in our analyses may also contribute to reducing some of the potential biases.
In conclusion, lower baseline Hb concentrations were found associated with a higher incidence of cognitive impairment over a 4.4-year follow-up in a sample of people older than 65 years of age. This relationship seems to be stronger in men than in women. Since low Hb levels are very common in the elderly, further research is needed to see whether preventing or correcting anemia could delay the progression to cognitive impairment in older people.
Footnotes
Acknowledgments
We are grateful to all interviewers, nurses, and physicians who collaborated in this study. The data collection phase of the PRO.V.A. study was supported by the Fondazione Cassa di Risparmio di Padova e Rovigo; University of Padova; the Azienda Unità Locale Socio Sanitaria 15 and 18 of the Veneto Region; and a grant from the Veneto Regional Authority (Ricerca Sanitaria Finalizzata n.156/03). The data analysis phase was also financed by a grant of the University of Padova (Population aging—economics, health, retirement, and the welfare state—POPA_EHR). The sponsors did not have any role in the design, methods, subject recruitment, data collections, analysis, and preparation of the article.
Author Disclosure Statement
No competing financial interests exist.