
Abstract
High or low thyroid-stimulating hormone (TSH) levels seem to be associated with several negative outcomes in the elderly, but the literature about TSH and frailty is still limited. In this article, we investigated whether TSH is associated with prevalent and incident frailty in a cohort of older community-dwelling subjects. Among 3099 initially screened in the Progetto Veneto Anziani Study, 2571 men and women aged ≥65 years (for cross-sectional analyses) and 1732 (longitudinal, mean follow-up period of 4.4 years) were divided into sex-specific quintiles according to baseline serum TSH concentrations within normal range (0.3 and 4.2 mUI/L). Frailty was defined as the presence of three among five Fried's criteria. At baseline, taking those in the third quintile of serum TSH as reference (Q3) and adjusting for potential confounders, participants in the highest (Q5) quintile had an increased odds ratio (OR) of having frailty (OR = 1.55; 95% confidence interval [CI]: 1.03–2.33 for men; OR = 1.97; 95% CI: 1.59–2.45 for women). Men in Q1 had significant higher odds of having muscle weakness and exhaustion, while those in Q5 had muscle weakness and slow gait speed. Women in Q1 had significantly higher odds of having all the Fried's criteria (except for exhaustion), while those in Q5 reported a significantly higher presence of muscle weakness and slow gait speed. At follow-up, men in Q5 had an increased risk of frailty (OR = 1.37; 95% CI: 1.02–1.91) similar to women in Q1 (OR = 1.47; 95% CI: 1.21–1.78). In conclusion, men with higher and women with lower serum TSH levels are at increased risk of frailty.
Introduction
F
There is a growing evidence base to suggest that frailty is characterized by a “metabolic signature.” 4 Frail subjects are characterized by higher chronic inflammation levels 5 and concomitant downregulation of multiple endocrine factors, 4 suggesting that these markers could be useful for the early identification of frailty.
Unfortunately, very few representative studies have assessed the potential relationship between thyroid function (assessed with thyroid-stimulating hormone [TSH]) and frailty. Two cross-sectional studies 6,7 reported a nonsignificant association between TSH levels and frailty, although one found an association between free thyroxine and frailty. 7 One longitudinal study 8 did not find an association of subclinical hyperthyroidism and hypothyroidism with incident frailty in older men. This longitudinal study, however, included very few participants for both hyperthyroidism (n = 22) and hypothyroidism (n = 85). These findings are somewhat surprising since both subclinical hyperthyroidism and hypothyroidism are associated with a high rate of medical conditions significantly associated with frailty as previously mentioned.
Previous literature has suggested that in the elderly, thyroid function at the extremes of the normal range could be associated with the onset of several medical conditions. 9,10 However, the knowledge of the relationship between TSH and frailty is still limited and worthy of improvement through representative research. We investigated whether TSH is associated with frailty in a cohort of older men and women. We hypothesized that assessing the association between TSH and frailty in both cross-sectional and longitudinal studies of the same population and correcting for potential confounders might provide more definitive evidence about the TSH-frailty relationship.
Methods
Data source and subjects
The data for this analysis were derived from the Progetto Veneto Anziani (Pro.V.A.), an observational cohort study on the Italian population aged ≥65 years. The study population included 3099 age- and sex-stratified Caucasian participants (1854 women and 1245 men) randomly selected between 1995 and 1997 using a multistage stratification method. Sampling procedures and data collection methods have been described elsewhere. 11 This study utilizes information obtained at baseline and at follow-up after 4 years.
The local ethics committees of Padova University and the Local Health Units (ULSS) n. 15 and n. 18 of the Veneto Region approved the study protocol, and participants gave their written informed consent.
Clinical data
Participants were examined at city hospitals by trained physicians and nurses. Information was collected on their smoking, alcohol drinking, education, and monthly income during a face-to-face interview. Smoking status was classified as “current” versus “never/former” (smoking for at least a year in the past). Alcohol drinking was categorized as “yes” versus “no” in the previous month. Education was categorized as ≤ versus >5 years, 5 years being the level of primary education in Italy. Monthly income was categorized as ≥ versus <500 €. Body weight and height were measured by trained physicians and body mass index (BMI; kg/m2) was calculated.
Disability was evaluated with the number of activities of daily living (ADL) preserved using the index proposed by Katz et al., 12 while cognitive status and depressive mood with 30-item minimental state examination (MMSE) 13 and geriatric depression scale (GDS), 14 respectively.
Details of all medical conditions were ascertained by board-certified physicians involved in the study, who examined all of the clinical information collected for each participant, including disease history, symptoms self-reported using standardized questionnaires, medical and hospital records, blood tests, and physical examination. 11 For the aim of this study, validated general health measures of comorbidities were assessed by calculating modified Charlson comorbidity score, with higher scores indicating an increased severity of conditions. 15 Renal function was assessed from the estimated glomerular filtration rate (eGFR) calculated with the Modified Diet in Renal Disease formula.
Definition of exposure and outcome
Blood samples were obtained after an overnight fast for biochemical tests, which were performed at the city hospital's central laboratory using standard, quality-controlled procedures. TSH was measured in serum with a third-generation immunoassay using a range for normality values between 0.3 and 4.2 mUI/L. 16 The coefficients of variation for this test (intra and interassay) were <5%. Since a significant difference between men and women existed (p < 0.0001, t-test independent samples), the population was divided in quintiles using 0.7, 1.0, 1.3, and 2.0 mUI/L for men and 0.8, 1.1, 1.5, and 2.5 mUI/L for women as cutoffs.
Frailty was the primary outcome of interest. Fried defined frailty using five items (unintentional weight loss, low physical activity level, weakness, exhaustion, and slow gait speed).
17
For this research, we used a slightly modified version
18
: - Unintentional weight loss: self-reported unintentional weight loss ≥5 kg over the past year without known reasons. - Self-reported low physical activity level: week physical activity below 383 kcal in males and 270 kcal in females,
17
calculated from the sum of all the leisure-time activities performed during a typical week in the previous month. - Weakness: best handgrip strength value of three attempts of the dominant hand below the sex- and BMI-specific cutoffs suggested by Fried et al.
17
- Exhaustion: a GDS ≥10/30 and a negative answer to the question: “Do you feel full of energy?”
19
- Slow gait speed: the best timed walk over 4 m at usual pace below the sex- and BMI-specific cutoffs.
17
Subjects unable to perform the handgrip strength or walking tests were considered having weakness or slow gait speed, respectively. Participants were classified as (1) frail if they met three or more of the five modified Fried criteria, (2) prefrail if they met one or two criteria, and (3) robust if they met none of the criteria.
Statistical analyses
To generalize the Pro.V.A. sample to the general population of the two geographical areas, a set of weights was defined according to the sex and age distribution of the reference population (Italy, Census 1991) and to the sample fraction.
Since a significant interaction between TSH and gender existed, taking frailty (prevalent or incident) as outcome, the data are reported according to gender. For continuous variables, normal distributions were tested using the Shapiro–Wilk test. Age-adjusted p-values were calculated by TSH quintiles using a generalized linear model with the Bonferroni's correction and taking the third quintile (Q3) (containing the mean of the baseline TSH value) as the reference group. Levene's test was used to test the homoscedasticity of variances and, if its assumption was violated, Welch's analysis of variance was used. Differences in categorical variables were examined using the logistic regression analysis, including age as covariates.
For baseline data, we calculated odds ratios (ORs) and 95% confidence intervals (CIs) to assess the strength of the association between TSH and frailty, taking those in Q3 as reference. In secondary analyses, we also evaluated the association between TSH and each of the single items in Fried's criteria, taking those with any criterion as reference.
For follow-up analyses, we removed the subjects already frail at baseline and those without follow-up data, investigating the incidence of frailty by baseline TSH concentrations. The proportional hazards assumption was checked by plotting the Schoenfeld residuals versus time, 20 but since the p-value was <0.05 for the interaction of TSH by frailty at follow-up, a logistic regression was used instead of Cox's regression analysis.
Known factors associated with frailty were considered for inclusion and all the variables reaching a p ≤ 0.10 in the univariate analyses were finally included in the fully adjusted model. Multicollinearity among the covariates was assessed using the variance inflation factor with a cutoff of 2 as exclusion criterion, but no covariate was excluded for this reason. In preplanned secondary analyses, we tried to evaluate the association between TSH and singular Fried's criteria, but since for three criteria (unintentional weight loss, low physical activity level, and exhaustion) we had less than 50 incident cases, we did not report these elaborations for convergence problems.
All analyses were performed using the SPSS 21.0 for Windows (SPSS, Inc., Chicago, IL). All statistical tests were two tailed and statistical significance was assumed for a p-value ≤0.05.
Results
Baseline characteristics
As shown in Figure 1, among the 3099 participants enrolled in the study, we initially excluded 528 participants (73 subjects were taking thyroid hormones, 187 with inadequate TSH data, 192 with TSH over or below the normality range, and 76 with no data about frailty), retaining a sample of 2571 community-dwelling elderly subjects for the cross-sectional analyses.
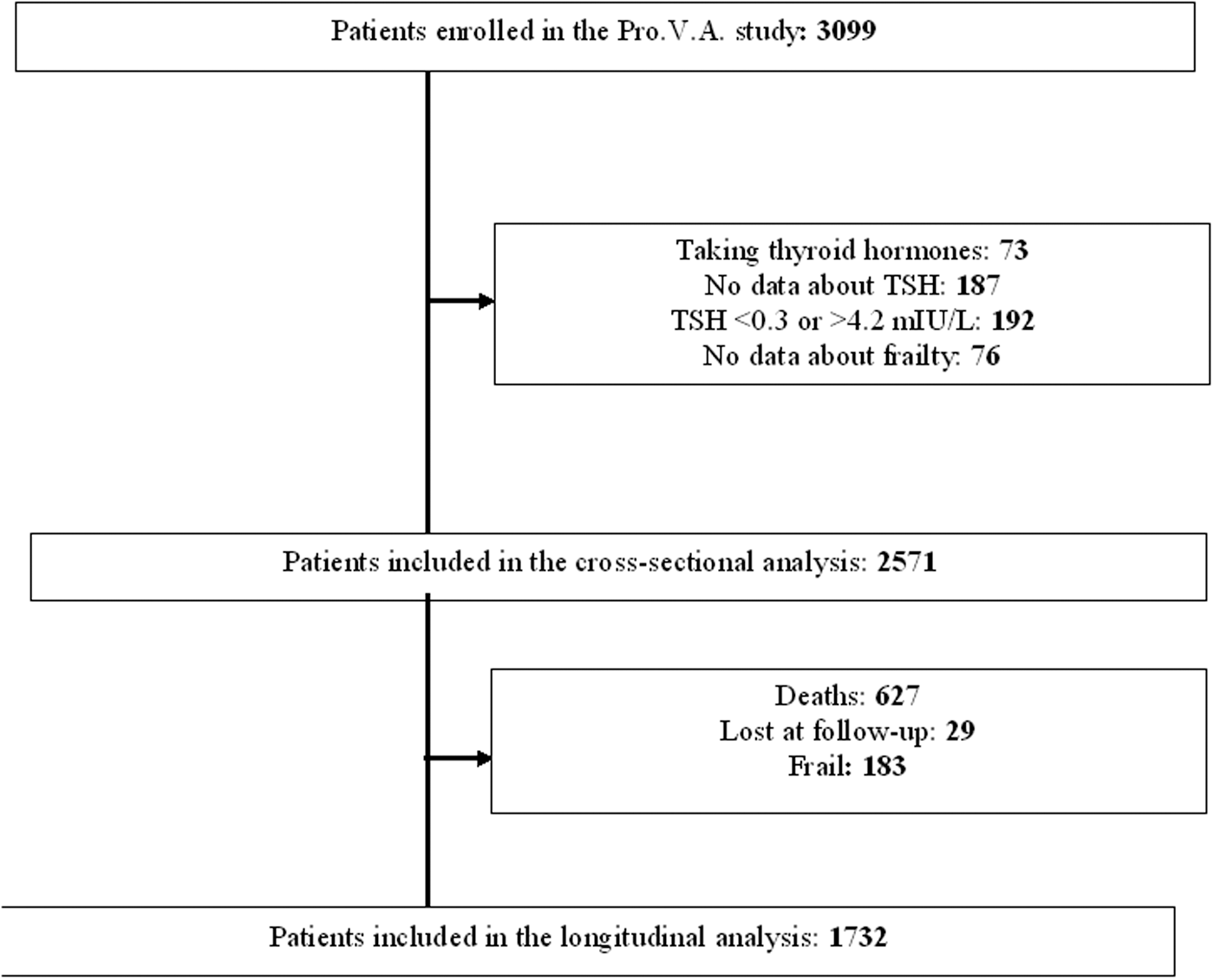
Flow chart of the Progetto Veneto Anziani study. Pro.V.A., Progetto Veneto Anziani.
Cross-sectional results
The mean age of the sample was 74.1 ± 7.0 years (range: 65–99), 60% were females. The mean TSH was 1.5 ± 0.8 mUI/L, with significantly higher levels in women versus men (1.6 ± 0.9 vs. 1.3 ± 0.8 mUI/L, p < 0.0001). At baseline, 183 (8.3%) participants were frail.
Table 1 shows the baseline characteristics by TSH quintiles and gender. Taking men in Q3 as reference, men in Q5 were significantly older, more disabled, and with lower MMSE score, but with a significantly higher Charlson comorbidity score and use of medications and worse renal function (Table 1, upper part). Similarly, men with lower TSH levels (Q1) were significantly less educated, with poorer monthly income, and took a higher number of drugs than men in Q3. Regarding women, those in Q5 were significantly older than women in Q3, while participants in Q1 had a significantly lower BMI, GDS, and MMSE score when compared to the reference group (Table 1, lower part).
Numbers are mean values (and standard deviations) or percentages (%), as appropriate. Age-adjusted p-value was calculated with a generalized linear model for continuous and logistic regression analysis for categorical variables, respectively, using age as covariate (except for age).
TSH quintiles were calculated using gender-specific cutoffs: for men: 0.7, 1.0, 1.3, and 2, while for women 0.8, 1.1, 1.5, and 2.5 mUI/L. Statistical significance: taking Q3 as reference, p-value <0.05 was indicated with b for each quintile.
ADL, activities of daily living; BMI, body mass index; eGFR, estimated glomerular filtration rate; GDS, geriatric depression scale; MMSE, minimental state examination; TSH, thyroid-stimulating hormone.
Figure 2 shows the prevalence of frailty according to baseline serum TSH concentrations by gender. The lowest prevalence of frailty was present in those in Q3 in both genders (6.3%; men = 4.2%, women = 7.6%), while those in Q1 (5.5% in men and 10.4% in women) and Q5 (7.5% in men and 15.3% in women) had the highest prevalence.

Prevalence and incidence of frailty by baseline TSH levels in men and women. TSH, thyroid-stimulating hormone.
Table 2 summarizes the association between baseline serum TSH and the prevalence of frailty in men and women, respectively. Taking those in Q3 as the reference group and after adjusting our analyses for 12 potential confounders (age, BMI, smoking habits, alcohol drinking, education, monthly income, ADL, GDS, MMSE, Charlson comorbidity score, eGFR, and number of drugs), participants in Q5 reported significantly higher odds of prevalent frailty independent of the gender (OR = 1.55; 95% CI: 1.03–2.33 for men and OR = 1.97; 95% CI: 1.59–2.45 for women) (Table 2, upper parts).
Unless otherwise specified, data are presented as odds ratios and 95% confidence intervals.
Fully adjusted model included the following: age and BMI (both as continuous); smoking habits (current vs. former/never); alcohol drinkers (yes vs. no); education (≥ vs. <5 years); monthly income (> vs. ≤500 €); ADL, geriatric depression, MMSE scores (all as continuous); Charlson co-morbidity score; eGFR; and number of drugs (both as continuous). For incident frailty, also the presence of pre-frailty at the baseline was included as covariate.
Table 3 reports the association between baseline serum TSH levels and the presence of individual Fried's criteria. Taking those in Q3 as reference and after adjusting for the same confounders listed for Table 2, men in Q1 had significantly higher odds of having weakness and exhaustion, while those in Q5 had significantly higher odds of having weakness and slow gait speed. Conversely, in women, lower TSH levels (i.e., Q1) had significantly higher odds of having all the Fried's criteria (except for exhaustion), while those in Q5 reported a significantly higher risk of poor physical performance in terms of weakness and slow gait speed
Unless otherwise specified, data are presented as fully adjusted a odds ratios and 95% confidence intervals. The prevalence of each criterion is reported below the odds ratio. In all the analyses, participants without any Fried's criterion are taken as reference.
Fully adjusted model included the following: age and BMI (both as continuous); smoking habits (current vs. former/never); alcohol drinkers (yes vs. no); education (≥ vs. <5 years); monthly income (> vs. ≤500 €); ADL, geriatric depression, MMSE scores (all as continuous); Charlson comorbidity score; eGFR; and number of drugs (both as continuous).
Follow-up data
As shown in Figure 1, the longitudinal analyses considered 1732 individuals (627 were excluded due to mortality, 29 because they did not return at follow-up, and 183 were frail at baseline). During the follow-up period, 93 men and 183 women became frail (13.6% of baseline male population and 17.4% of women).
As reported in Figure 2, the cumulative incidence of new cases of frailty was lowest in participants in the third quintile for women (14.1%) and in Q1 for men (9.0%).
Using a logistic regression analysis adjusted for potential confounders at baseline (including also the presence of pre-frailty) and taking those in the third quintile for reference, men in Q5 had an increased risk of frailty at follow-up (OR = 1.37; 95% CI: 1.02–1.91), similar to women in Q1 (OR = 1.47; 95% CI: 1.21–1.78)
Discussion
This is the first study showing that in a large cohort of community-dwelling older men and women, TSH is associated with prevalent and incident frailty. In men, higher TSH levels are associated with both prevalent and incident frailty, while in women, we observed that higher TSH levels are associated with an increased presence of frailty at baseline, but lower TSH levels were associated with an increased risk of frailty in longitudinal analyses. However, when taking the individual Fried's criteria as outcome, lower TSH levels seem to be more strictly associated with these parameters than higher levels, particularly in women.
TSH is a pituitary hormone that stimulates the thyroid gland to produce hormones (FT3 and FT4). The TSH levels are controlled by FT3 and FT4 concentrations, thanks to a fine mechanism of feedback. The most common endocrine alterations are due to primary thyroid dysfunctions, while a minor part is related to pituitary disorders. Given this background, we assumed that lower TSH levels may correspond to subclinical/clinical hyperthyroidism, while higher TSH levels could be representative of subclinical/clinical hypothyroidism.
Regarding lower TSH levels, it is known that subclinical and clinical hyperthyroidism are associated with several comorbidities (namely osteoporosis, cardiovascular diseases, and cognitive decline) also common in people with frailty. 8 However, after adjusting our analyses for these confounders, our results remained significant for incident frailty in women. Moreover, lower TSH levels were associated with significantly higher odds of having several of the single items of Fried's criteria (particularly in women), suggesting that hyperthyroidism could play a role in the development of frailty. Another hypothesis is that lower TSH levels are associated with low physical performance level 21 and since Fried's criteria are mainly based on physical performance items, it is likely that the effect of low TSH could depend on this factor. Third, low TSH, although in the range of normality, could be associated with weight loss, another characteristic considered in the Fried's definition of frailty. This finding is indirectly confirmed by our analyses since in women, low TSH levels were associated with 65% increased odds of having weight loss, also after considering the effect of potential confounders.
Conversely, regarding higher TSH levels, it is known that this biohumoral condition is associated with other comorbidities highly prevalent in frail subjects such as depression. 8 Hypothyroidism, in fact, can cause a number of symptoms (such as a feeling of tiredness, depression, and fatigability) that are also typical of frailty. Moreover, hypothyroidism has been reported to be associated to low-grade inflammation, a condition strongly related with frailty, also if TSH is within normal ranges. 22 Finally, the subjects with high TSH levels usually have some neuromuscular and musculoskeletal symptoms 23 that are overlapping with those specific of frailty status. Again, our analyses showed that in both genders, high TSH levels are associated with higher presence of weakness and slow gait speed, reinforcing the concept that this condition is important for a good physical performance level.
Indeed, TSH could be useful as a biomarker of frailty since small variations within the normal range from the reference group significantly predicted the onset of frailty. The absence of a univocal operational definition for frailty, however, makes the development of measurable biomarkers tailored to the chosen definition. Thus, verifying whether TSH maintains correlative and predictive properties using different definitions of frailty and in different populations might confirm its potential role as a biomarker. 24
Another important finding of our work is the substantial difference between men and women in the relationship between baseline serum TSH levels and incident frailty. In men, higher TSH levels predicted incident frailty, while in women, we observed that lower TSH levels were associated with an increased risk of frailty. Altogether, these findings confirm the important gender differences as proposed by animal models 25 and confirmed in human beings, 26 showing that TSH is significantly higher in women than in men and TSH is more responsive to thyroid function alterations in men than in women. 26
To date, two cross-sectional studies 6,7 and one longitudinal study have not found a significant association between TSH levels and frailty. 8 Several explanations might account for this discrepancy. First, the longitudinal study by Virgini et al. 8 followed up 22 subjects with subclinical hyperthyroidism and 85 with subclinical hypothyroidism and thus clearly lacks power. Moreover, this study utilized FT4 data and this may offer a potentially more complete assessment of thyroid function. Second, Virgini et al. 8 only considered men. Not only does this reduce generalizability but also frailty and thyroid dysfunctions are less common in men than women. Finally, the different definitions of frailty could play an additional role in interpreting the different results. Given the aforementioned, we consider that our representative cross-sectional and cohort study is the most robust study to date to investigate the relationship between TSH and frailty, building on the previous literature.
Nonetheless, while our study contains novel findings, it is important to consider a number of limitations. The main limitation is that we used TSH as a marker of thyroid function. Although it is likely that low TSH levels correspond to high FT4 levels and vice versa, other more rare conditions could be misinterpreted. Moreover, in the elderly (particularly in the very old, disabled, and with several comorbidities), it is a common condition characterized by low FT3 with increased rT3 and TSH levels, 27 reinforcing the lack of thyroid hormones as the main limitation of our work. In a similar way, the lack of autoantibodies could represent another limitation for our findings. Unfortunately, in the Pro.V.A. study, these parameters of thyroid function were not assessed since this study was primarily designed to explore the association between osteoarticular and cardiovascular diseases and their impact in life of older people. Second, we did not assess the changes in thyroid function over time, while it seems that serum TSH shifts progressively to higher levels with age, also when considering centenarians. 28 Third, some substances that might influence thyroid function (e.g., cortisonic drugs, lithium, and recent investigations with iodinated contrast material) were not considered. Future research should therefore attempt to investigate the impact of these on the development of frailty by TSH levels. Fourth, the Pro.V.A. study was undertaken ∼20 years ago. Although the methods of ascertaining both frailty and TSH remain similar, we cannot exclude a bias in our results. Finally, due to the limited number of cases, we were not able to explore the potential association between serum baseline TSH and the incidence of the individual items of Fried's criteria. Focused research regarding this topic is needed.
In conclusion, men with higher and women with lower serum TSH levels are at increased risk of frailty. These findings suggest important gender differences in the association between thyroid function and frailty. Our study suggests that TSH could be used as marker for frailty since small variations significantly predict the onset of frailty. Future longitudinal studies are, however, needed to confirm our findings.
Footnotes
Acknowledgments
We are thankful to all interviewers, nurses, and physicians who participated in the study. The data collection phase of the Pro.V.A. study was supported by the Fondazione Cassa di Risparmio di Padova e Rovigo; University of Padova; the Azienda Unità Locale Socio Sanitaria 15 and 18 of the Veneto Region; and a grant from the Veneto Regional Authority (Ricerca Sanitaria Finalizzata n.156/03). The data analysis phase was also financed by a grant of the University of Padova (Population aging—economics, health, retirement and the welfare state—POPA_EHR).
Author Disclosure Statement
No competing financial interests exist.