
Abstract
The purpose of this systematic review was to provide a comprehensive analysis of the available clinical trials analyzing, in seniors, the effect of interval aerobic training (IAT) and continuous aerobic training (CAT) on peripheral brain-derived neurotrophic factor (BDNF) concentration. We identified 14 randomized or not-randomized intervention studies published up to January 2017 through a computer-assisted search (PUBMED, Pedro, and Science direct data bases). The five trials considering IAT and the nine considering CAT totalized 988 individuals (age range: 58.1–77 years). The parameters of aerobic training (AT) protocol in terms of frequency and intensity are the primary determinants of the BDNF response to AT. The interpretation of the relationship between AT and BDNF signaling pathway was very challenging when specific health conditions were taken into consideration. This was more particularly true with mild cognitive impairment or depressive symptoms. These findings argue in favor of a generalization of the practice of AT and show that the type of training is not the main determining factor of the increase in BDNF level, which results more from the combination of several factors such as intensity and frequency of sessions, duration of programs, and also some genetic determinant coding for BDNF protein. All these factors have to be carefully addressed in future researches in that field. Thus, further researches are still necessary to better the signaling pathway by which AT contributes to better health outcomes.
Introduction
T
Indeed, while aging must be considered a positive experience, lengthening life span is, however, not necessarily synonymous with extending disability-free life expectancy. 3 The aging process is intrinsically associated with a progressive decline in muscle strength and mass, and aerobic capacity. This contributes to reduced mobility, and impaired independency and quality of life. 2 In addition, the incidence of a plethora of chronic comorbid conditions increases with advancing age. 4 Alzheimer's disease (AD) and related disorders are one of the first causes of dependency and disability in the aging and aged adult population worldwide. 5 As the life expectancy lengthens and the population grows older and older, the number of cases and the associated burden are expected to dramatically increase. 6,7
One of the pathogenic factors related to cognitive impairment is the reduced circulating brain-derived neurotrophic factor (BDNF). 8 Member of the nerve growth factor family, BDNF, is widely expressed in the mammalian brain, especially in the hippocampus, but also in peripheral nervous system, and in the kidney or the prostate gland, for example. 9,10 It plays an important role in memory process learning and is involved in cerebral plasticity, brain health, and improvement of neuron survival. 11 The BDNF signaling pathway positively acts in the central nervous system on neurons of the hippocampus, cortex, and basal forebrain. It supports neuron survival and growth, and modulates the differentiation of new neurons and synapses. 12 Furthermore, the BDNF signaling pathway at the hypothalamus level contributes, in part, to regulate energy homeostasis, body weight control, and feeding behavior. Outside the central nervous system, BDNF is involved in the regulation of fat oxidation in the skeletal muscle. 13,14 In addition, for some authors, the BDNF blood level represents a highly valuable biomarker that can help both the diagnosis and prognosis of neurodegenerative diseases and psychiatric disorders. 15 It could also be considered a predictor of the treatment response, and an increased blood circulating level of BDNF is a biomarker of good mental health. 15
The concentration of blood and brain BDNF eases off when people grow old and has been associated with neuronal loss during the course of neurodegenerative disorders like AD and Parkinson's disease (PD), and frontotemporal and Lewy bodies' dementia. 16,17 Among the nonpharmacological therapies that are able to positively impact the BDNF level is the regular practice of physical activity. In animal studies, aerobic training (AT) increased the BDNF micro-RNA activity in the brain. 18 –21 With respect to good mental health, AT has also been recognized as being beneficial by the induction of neurogenesis and neuroplasticity, the improvement in skeletal muscle ability and spatial learning, the reduction of cardiovascular risk factors, and the enhancement of cognitive functions and mental abilities that help people deal with anxiety and depression. 22 –25
Studies in humans have also investigated the health benefits of different types of AT. More particularly, the impact of continuous aerobic training (CAT—which consists in maintaining a submaximum intensity) and interval aerobic training (IAT—which are combined periods of intense workload with lesser workload or periods of rest) on the blood circulating BDNF level has been analyzed. 26,27 Beyond the direct effect on the brain's functioning, it is the potential role played by the BDNF signaling pathway in the exercise-induced benefits on general health and other specific health conditions that were also more recently risen. 28
Four systematic reviews have already confirmed the booster effects of physical activity (acute or AT) on circulating BDNF concentrations in animal models, in healthy young adults, and individuals with other specific health conditions. 29 –32 One meta-analysis has also addressed the benefits and reliability of exercise training on BDNF expressions in humans. 33
The present systematic review is specifically focused on aged adults who represent the population with the higher risk and incidence of cognitive and degenerative disorders and where a sedentary lifestyle is also the most prevalent. 34 The main aim was to provide an overview of available interventional clinical trials considering the effect of IAT or CAT on the basal peripheral BDNF concentration.
Materials and Methods
Search strategy
A comprehensive systematic search for articles published till January 31, 2017 was performed by a computer-assisted search in PubMED, PEDro, and Science direct databases. The entire search was conducted using the following key words: training, exercise, aerobic, BDNF, and elderly. In addition, all titles were manually searched for potential inclusion in this review; reference lists of articles retrieved, review articles, and position stands were examined for further relevant references.
Criteria for study inclusion/exclusion
Based on the title of the article and available excerpt, the articles were then evaluated for inclusion in the review using the following criteria:
Article type and study design
Original research articles reporting intervention studies (randomized controlled trial—RCT or not randomized trial) published in peer-reviewed journals were considered for inclusion. Full articles limited to the English language were extracted.
Population
Seniors were the targeted population with the selection of trials considering a sample of adults on average aged 60 years or older.
Intervention
The intervention must have been an endurance/AT program (low to high intensity). This included any exercise involving movement of large muscle groups (e.g., treadmill, walking, cycling, and rowing). Studies focusing on AT in multimodal or multicomponent training program were also considered (i.e., AT combined with muscle strengthening, balance exercises, and/or flexibility training and/or coordination training). Both IAT and CAT protocol were included. The studies that have reported physiological parameters such as heart rate (HR) and detailed the intensity, duration, frequency of training sessions, and the total duration of the exercise protocol were considered scientifically serious.
Outcome measures
Studies must have analyzed the impact of AT program on peripheral BDNF level and reported changes (posttraining and baseline measurement) due to the AT program. Only plasma, serum, or platelet BDNF levels obtained from peripheral blood samples were considered. 35
Noninclusion/exclusion criteria
The articles about studies conducted in animal models, considering an acute exercise program, or which did not assess BDNF changes due to AT were not included or secondary excluded.
Quality assessment
Once the articles were collected and had met all inclusion criteria, a more detailed assessment of the study eligibility was conducted as detailed in Figure 1. 36 Subsequently, the quality of RCTs was assessed in terms of random sequence generation, allocation concealment, blinding, and other sources of bias according to the Cochrane Collaboration risk of bias assessment for potential bias (low, unclear, and high). 37
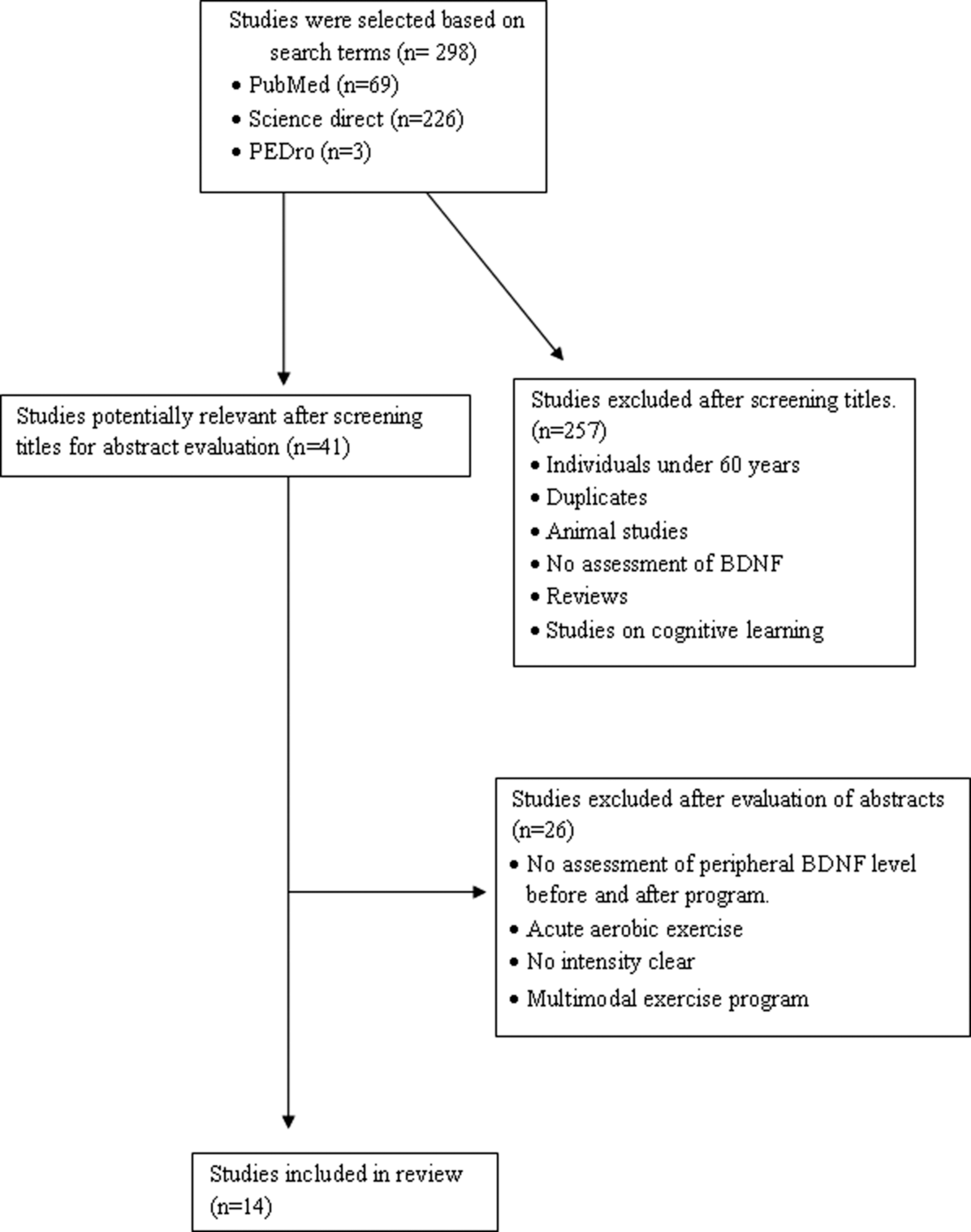
Flowchart of the literature search.
Results
Study inclusion/exclusion
The process of study inclusion/exclusion is detailed in Figure 1. Briefly, the search strategy has identified 298 articles. After screening the titles and abstracts, 257 articles were immediately excluded. Finally, 14 studies were definitely included, of which five considered IAT and 9 considered CAT (Table 1).
BDNF, brain-derived neurotrophic factor; FC, cardiac frequency; HRmax, maximal heart rate; HRR, heart rate reserve; PD, Parkinson's disease; MCI, mild cognitive impairment.
Study population
The 14 studies included in the review totalized 988 individuals (age range: 58.1–77 years). 15,38 IAT protocols were considered in five studies 38 –42 and nine CAT. 15,43 –50 The studies enrolled people with mild cognitive impairment (MCI), 39,41,44,50 depressive symptoms according to the assessment with the Geriatric Depressive Scale (but not formally depressed), 47 PD, 38,40 glucose intolerance, 43 or simply healthy individuals 15,42,45,46,48,49 When 13/14 considered both gender, one study focused on female only. 47
Study quality
Globally, 13/14 studies were RCTs and all specified their inclusion criteria. The RCTs randomly assigned groups, and 14/14 studies reported baseline characteristics of the population and standard deviation or confidence intervals. The percentage of exercise attendance was reported in 4/14 studies and compliance with exercise progression in 14/14. All studies reported power calculations and detailed the strategy and method used to quantify BDNF in serum (nine studies) or plasma (five studies). The occurrence of adverse events during AT programs was reported in 3/14 studies.
AT protocols
As summarized in Table 1, across the five studies that have considered IAT, the training intensity was ranged from 60% to 80% of maximal HR (HRmax) and the total duration of the program was set to an 8–16-week period, with a frequency of three sessions per week (40–60 minutes each). For the nine studies on CAT, the intensity of the exercise was ranged from 50% to 70% of the maximum oxygen uptake (VO2max), 50% to 80% of HRmax, or 50% to 85% of HRmax reserve.
The training protocols either considered walking, Nordic walking, running, cycling, aquatic exercise, or an elliptical trainer.
IAT program on BDNF level
A significant increase was measured in 4/5 studies following the training protocol as showed in Table 1. BDNF serum level was measured in two studies, 38,40 two studies considered plasma concentration, 39,41 and one study analyzed serum and BDNF level. 42
Zoladz et al., 40 in 12 PD patients, reported that 24 sessions of moderate IAT over 8 weeks increased, significantly, the BDNF level (baseline: 10.977 ± 756 pg/mL; posttraining: 14.206 ± 1256 pg/mL; p = 0.03). Marusiak et al. 38 found an increase in the serum BDNF level of 34% (p = 0.035). Nascimento et al., 41 in MCI or healthy individuals, measured a significant increase between pretraining and posttraining values (2.85 ± 1.9–3.43 ± 2.2 pg/dL and 2.81 ± 1.5–3.56 ± 1.8 pg/dL, respectively, all p < 0.001). Nascimento et al., 39 in MCI, reported a similar benefit after 6 months of IAT in the trained group only (2.44 ± 0.98 vs. 3.07 ± 1.06 pg/dL; p = 0.01). Maass et al., 42 in healthy individuals, found an increase in serum or plasma BDNF that did not reach the significant threshold after 4 weeks of walking on a treadmill (17635.9 ± 5754.5–16917.8 ± 6958.6 pg/mL).
CAT program on BDNF level
As shown in Table 1, nine studies considered CAT and have recruited healthy individuals (five studies), two, individuals with MCI (two studies), adults with depressive symptoms (one study), and seniors with glucose intolerance (one study). BDNF serum was measured in six studies, while other studies considered plasma. Two studies reported significant increases in BDNF concentration at rest after the CAT period, 45,48 and 4/9 showed trends toward the improvement of peripheral BDNF secretion (i.e., p-values above the significant threshold), 15,46,49,50 and 3/9 revealed more conflicting results. 43,44,47
In healthy individuals, Erickson et al., 45 after 12 months of training, reported an increase in serum BDNF levels (from 21.32 ± 9.32 to 23.77 ± 8.04 pg/mL posttest), which was correlated with an increment of the hippocampus volume. These results were confirmed after a 52-week CAT program (preintervention: 21,736.91 ± 9768.31 pg/mL; postintervention: 24,067.78 ± 7814.90 pg/mL). 48 The last study showed that individuals trained in aerobic condition increased their BDNF levels, while those in the nonaerobic condition even demonstrated a decrease in serum values. After 6 months of CAT, Ruscheweyh et al. 15 showed a positive relationship, but not significant, in BDNF levels in the training group.
Similar results were reported by Voss et al. 46 after 7 weeks of walking with moderate intensity and Schega et al.'s 49 study in which healthy individuals were trained during 4 weeks in normobaric hypoxia conditions (i.e., simulated altitude conditions). The authors have found increasing values as expected in hematological parameters, but also in the time to exhaustion, and a sustainable improvement in cognitive function among trainees, while the serum BDNF-level did not increase (ratio serum BDNF-level pretest intervention group (IG): 0.91 ± 0.35, posttest IG: 1.07 ± 0.13, pretest control group (CG): 0.88 ± 0.27, and posttest CG: 1.05 ± 0.10.)
In individuals with MCI, Allard et al. 50 reported increases in serum BDNF in stretch (+46.29%) and aerobic (+15.12%) groups, but without reaching the significant threshold. Baker et al. 44 revealed more conflicting results since no significant changes were measured between pretraining and posttraining in aerobic groups.
Pereira et al., 47 in women with depressive symptoms, and Baker et al., 43 in person with glucose intolerance, did not find any significant change after the CAT period.
Discussion
In the past few years, there has been a growing interest in understanding the signaling pathways underlying the beneficial effects of AT on various health conditions and in brain functioning. Neurodegenerative disorders such as Alzheimer's and associated disorders were particularly studied. 51 With advancing age, there is a progressive decline of blood-circulating BDNF concentration, which parallels the decline in cognitive performances, 16,17
To the best of our knowledge, this is the first systematic review that provides a comprehensive overview of the available literature about the impact of CAT and IAT on peripheral BDNF level in seniors. Out of the 14 interventional studies analyzed, 6 have reported a significant increase in peripheral BDNF level with 4/5 considering IAT and 2/9 considering CAT. These results are in line with the available literature reporting benefits of acute exercise on blood-circulating BDNF concentration. 52,53
Interval aerobic training
The high-intensity periods of IAT are typically at, or close to, the anaerobic threshold, while the recovery periods correspond to an activity at a much lower intensity. Thus, with IAT, we could easily expect benefits on brain functioning (i.e., cognitive function, blood flow, and resistance to injury) similar to those measured with acute physical activity. 54,55 One of the major underlying mechanisms that contributes to these changes is thought to be related to brain plasticity and mediated by growth factors such as BDNF. The activation of the BDNF signaling pathway results in the enhancement of learning and memory formation. 56
As presented in Table 1, five studies analyzing IAT have reported a significant improvement of blood-circulating BDNF concentration (i.e., plasma or serum). 33 –36 Furthermore, these studies were conducted in people with specific disorders, in which BDNF expression is physiologically reduced (i.e., PD and cognitive impairment, but also during the ageing process 57 –59 ), particularly in the most recent studies, from Nascimento et al., 39,41 in which the improvement of cognitive functioning and peripheral BDNF production were observed in person with BDNF met allele noncarriers (Val/Val) and met allele carriers (Val/Met). This finding contributes to reinforce the fact that cognitive benefits are more related to the brain plasticity rather than genotype allele carriers, 60 or the indirect effect of physical activity on some psychological components as often reported, such as well-being, concentration, and mood, for example. 61 Thus, according to the training protocols designed in Nascimento et al., IAT was included in multimodal programs conducted at 60%–80% of HRmax, for three sessions a week (1 hour each) over 16 weeks. 39,41 This induced an improvement in cognitive functioning in the trained groups.
Similar results were measured in seniors with PD. On the basis of 2/5 studies, 38,40 the IAT program was conducted on a cycloergometer and resulted in a better control of motor symptoms associated with PD and functional performance. 62 In animal models, it has been demonstrated that increased levels of neurotrophin were measured in the basal ganglia as a consequence of physical exercise and resulted in a cytoprotective effect on dopaminergic structures, and hence improvement in basal ganglia functioning. As a consequence, motor symptoms such as rigidity and bradykinesia were better controlled. 38,63,64
Compared to younger adults, in Zoladz et al., 65 the results measured after IAT program in older counterparts were similar in terms of BDNF production. This may suggest that intensity and workload are important parameters to consider to enhance BDNF expression rather than age effect. 66 In the study conducted by Maass et al., 42 after 3 months of IAT, there was no effect on blood-circulating BDNF concentration, but a significant improvement in blood perfusion in the hippocampus was observed. The last finding suggests that the benefits of IAT on brain functioning result from the improvement of tissue oxygenation and could also contribute to prevent the onset of cognitive impairment as well as dementia.
With respect to the aged population, the BDNF level was described as decreasing in concert with hippocampus atrophy, which all together turn to cognitive impairment and finally dementia. 59 Inversely, recent reports supported that regular practice of physical activity enhanced, among some cognitive functions, learning and memory formation. 2,56 Moreover, the BDNF signaling pathway was the underlying mechanism whereby the cognitive performance was improved or prevented.
CAT, in healthy seniors and individuals with neurodegenerative diseases
Nine studies have analyzed the CAT as training program. The results reported by Erickson et al. 45 and Leckie et al. 48 in healthy individuals after 12 months of walking-type exercise were in the line with those measured after IAT, but over a shorter period of training. This suggests that the exercise intensity is not the main modulating factor of BDN expression to consider. At an equivalent global volume of physical activity (i.e., intensity × session × frequency × duration), a similar impact could be shown in aged people. It was, however, difficult to confirm this hypothesis with these data, in view of the wide heterogeneity between training protocols across the studies. However, Griffin et al. 67 and Seifert et al., 68 in younger subjects, have demonstrated a significant increase in BDNF levels after a CAT program over a period of time shorter or equal to 3 months. Moreover, when other studies included in this systematic review reported similar trends in BDNF concentration after 7–26 weeks of CAT (Baker et al., 43,44 Ruscheweyh et al. 15 and Voss et al. 46 ), they did not all reach the significant threshold. This trend was, however, mirrored by an increase in the hippocampus volume in healthy individuals, 15,46 which confirms the positive correlation initially found by Erickson et al. 69 The studies conducted by Baker et al. 43,44 and Voss et al. 46 did not have enough subjects to reach a significant difference on BDNF level after CAT (e.g., in Baker et al. 43,44 the sample study was <20 individuals).
It is well recognized that in people with psychiatric disorders like schizophrenia or major depression, the BDNF levels were systematically lower than in age-adjusted healthy people. 24,58,59,70 This decrease in BDNF could affect the size of the hippocampus and therefore increase the risk of impaired cognitive function and onset of dementia. 59,71 In the study conducted by Pereira et al. 47 in aged community-dwelling women, while no significant increase in BDNF plasma level was measured after 10 weeks of CAT, participants showed improvement in their depressive symptoms. This reinforces the results reported by Toups et al., 72 that, improvement of depressive symptoms is not necessarily associated with specific changes in the BDNF level. However, with respect to BDNF, in Pereira et al.'s study, 47 women were not formally diagnosed with depression (but declared depressive symptoms) and hence the BDNF concentrations at baseline were not necessarily lowered as physiologically thought. 15 Interestingly, one study conducted in depressed patients reported that antidepressant treatment, in addition to improve mood symptoms, was associated with increasing BDNF levels. 73 This first suggests that the variation of BDNF expression in relationship with depressive symptoms is mediated by a neurotransmitter like serotonin or others implicated in the neurobiological pathway of depression. Afterward, in relationship to depressed patients who engage in AT program, in case of concomitant treatment with an antidepressant drug, the direct effect of physical activity on BDNF level could be concealed.
The study of Schega et al. 49 provided interesting information about the effect of CAT in conditions-simulated altitude. This original study, however, found no improvement in the serum BDNF level in seniors like it was measured in healthy young adults after just a 72-hour exposure to high altitude (∼11,000 feet, alveolar PO2 = 100 mmHg). 74
The recent study of Allard et al., 50 conducted in MCI Afro-American population, emphasizes the importance of the relationship between the apolipoprotein E (APOE) gene ɛ4 and the level of BDNF in the context of AT. This ɛ4 variant of the APOE is the greatest known genetic risk factor for late-onset sporadic AD in a wide variety of ethnic groups, 75 and recent evidence suggests that APOE genotype affects differently the expression of BDNF. Thus, in this study, the authors measured that non-ɛ4 carriers showed a significant upregulation in BDNF levels at the 6-month time point, while ɛ4 carriers did not. These results align with those reported by Ruscheweyh et al. 15 in which the authors, however, showed that CAT conveyed the beneficial effects on memory function independent of its intensity, possibly mediated by local gray matter volume and neurotrophic factors (BDNF-trend only). Altogether, these findings carry significant implications for prevention and particularly support the benefit of CAT, induced, in part, by the BDNF signaling pathway, in the prevention of cognitive decline, 2 but not in the most at-risk group of ɛ4 carriers.
Workload in AT
Exercise intensity is considered an important factor of which the level is frequently debated as being the main underlying regulator, explaining some of the benefits of physical and mental health outcomes. 66,76 Indeed, both the hypothesis of the inverted U-shaped dose–effect curve and the human's drive theory suggest that exercise intensity influences the size of the effect. 51 Thus, the latter states that humans have a drive to assess how they are doing and how they are doing; they seek standards against which to compare themselves. For example, in an investigation on how social influences encourage healthy behaviors such as exercise, so do the perceived attitudes of peers. The individuals were likely to mimic the behavior of those around them. Individuals feel the need to engage in socially acceptable attitudes, such as exercising, when observing others doing the same. 77 Finally, the “drive theory” suggests that the largest benefits will be observed at the highest intensity. With the inverted U-shaped dose–response hypothesis, it appears that moderate intensity induces the greatest benefits, when lowest and highest intensity are considered to induce null or even worse negative effects.
In studies evaluating the effects of acute exercise on blood-circulating BDNF values, it was reported that high-intensity training protocols resulted in a higher upregulation than did those considering lower intensity programs. Hence, there is a direct link between intensity level in acute physical activity and the level of BDNF-related health outcomes like cognitive performance or behavioral outcomes. 78
According to the findings of the present systematic review, the questions about the exact role played by the intensity and workload levels in the BDNF response are raised. In young adults 67,68,79 and sport students, 80 the results of variations in BDNF levels after CAT are heterogeneous. One possible explanation lies in the design of the training programs considered in the different studies. Indeed, in rat brains, the upregulation of BDNF after training programs was observed after incremental exercises that gradually increased the intensity from moderate to high when no changes was measured with either moderate or strenuous training. 28 Thus, acute exercise and IAT or CAT of high intensity facilitates the upregulation of BDNF. 81,82 This was confirmed by Schmolesky et al. 66 (high workload and intensity generated a positive BDNF response to exercise) and Tan et al. 51 (i.e., low workload and intensity were associated with higher risk of dementia). These findings suggest that an increase of basal peripheral BDNF level and higher brain volumes may be additional health benefits of AT among seniors.
The BDNF-mediated effect
Recent evidence suggests that endogenous molecules increased by exercise are able to cross the blood–brain barrier to enhance the expression of BDNF at the cerebral level. 83 As an example, Wrann et al., 84 in an animal study, reported that 30 days of AT (free-wheel running exercise) upregulates the BDNF expression through the induction of the hippocampus expression of Fndc5 (fibronectin type III domain-containing protein 5), a PGC-1α- and ERRα-dependent myokine. Fndc5 was initially discovered as a transcriptional coactivator of mitochondrial biogenesis and oxidative metabolism in muscle brown fat. 84,85 These findings can suggest that the upregulation of BDNF measured at the central nervous system level is a consequence of an increase in the mitochondrial activity and PGC-1 in the hippocampus, but also at the skeletal muscle level. 86 It was also proven that estrogens modulate the BDNF. 87 In that way, the decrease in hormone levels at menopause may result in lower expression of BDNF. This hypothesis is in line with the evidence suggesting that loss of estrogens in both women and men would play a role in the cognitive decline associated with AD. 88,89
Review limitations
While providing interesting and important findings, this systematic review has some limitations. When three electronic databases have been considered for the literature search, it did not include studies not edited in English or thesis dissertations. In addition, BDNF serum or plasma concentrations across the different studies showed considerable variability (concentrations of serum BDNF are ∼200-fold higher relative to those of plasma BDNF), 90 which could be attributed to the heterogeneity of methodological procedures for serum or plasma preparation and storage conditions. 91,92 These technical parameters would have contributed to mask the exact benefit of IAT or CAT on BDNF regulation.
Conclusion
Altogether these findings suggest that CAT and IAT tend to increase the blood-circulating BDNF concentration, although the results did not all reach the significant threshold. This was observed, whatever the senior's health status (MCI, PD, AD, depressive syndrome, or healthy). With respect to cognitive impairment, it appears that carrying ɛ4 genotype considerably limits the effect of AT on BDNF, contributing to explain the highest risk of AD in this population. Despite heterogeneity between studies and sometime a lack of statistical power, these results argue in favor of a generalization of AT among senior. This review also demonstrates that the type of training (IAT or CAT) is not the determining factor and BDNF level is modulated by several additional factors such as frequency of sessions, intensity, duration of programs, and some genetic determinants (possibly epigenetic as well), which drive the BDNF expression. All these factors have to be carefully addressed in future researches in this field.
Footnotes
Author Disclosure Statement
No competing financial interests exist.