
Abstract
The aim of this systematic review and meta-analysis was to summarize and analyze the effects of Nordic Walking on physical fitness, body composition, and quality of life in the elderly. Keyword “Nordic Walking” associated with “elderly” AND/OR “aging” AND/OR “old subjects” AND/OR “aged” AND/OR “older adults” were used in the online database MEDLINE, Embase, PubMed, Scopus, PsycINFO, and SPORTDiscus. Only studies written in English language and published in peer-reviewed journals were considered. A meta-analysis was performed and effect sizes calculated. Fifteen studies were identified; age of participants ranged from 60 to 92 years old. Comparing with a sedentary group, effect sizes showed that Nordic Walking was able to improve dynamic balance (0.30), functional balance (0.62), muscle strength of upper (0.66) and lower limbs (0.43), aerobic capacity (0.92), cardiovascular outcomes (0.23), body composition (0.30), and lipid profile (0.67). It seemed that Nordic Walking had a negative effect on static balance (−0.72). Comparing with a walking (alone) training, effect sizes showed that Nordic Walking improved the dynamic balance (0.30), flexibility of the lower body (0.47), and quality of life (0.53). Walking training was more effective in improving aerobic capacity (−0.21). Comparing Nordic Walking with resistance training, effect sizes showed that Nordic Walking improved dynamic balance (0.33), muscle strength of the lower body (0.39), aerobic capacity (0.75), flexibility of the upper body (0.41), and the quality of life (0.93). Nordic Walking can be considered as a safe and accessible form of aerobic exercise for the elderly population, able to improve cardiovascular outcomes, muscle strength, balance ability, and quality of life.
Introduction
T
In the last decades, different forms of physical activity were proposed and adapted to the elderly population, in alternative to the traditional training. Nevertheless, their effectiveness was not so clear. For this reason, interests among researchers in these activities were growing, to clarify their effectiveness in the physical capacities, but also on mood and quality of life. An example was the Pilates training, which was largely practiced by the population, but only few studies reported its effectiveness in terms of development of physical performance and well-being in the elderly. 4
Walking was considered one of the most common physical activities in the world. 5 It is a natural movement, rarely associated with physical injury and easy to be practiced by people of all ages, including the elderly. 6 Walking can be performed in different environments with no needs of particular equipment, overcoming some common barriers as the lack of time, fitness level, and money. 6 Moreover, the regular practice of walking activity was largely recommended for the overall health, 7 with the reduction in the all-cause mortality and in the risk to develop noncommunicable diseases. 8 A particular type of walking technique is the Nordic Walking (NW). NW is a form of brisk walking, utilizing a walking pole, which actively engages the trunk and upper limbs during walking, maintaining the natural gait, while the hands are performing an open–close cycle in an alternating manner. Due to the high muscle masses involved, NW produces a higher cardiorespiratory workload compared to the normal walking, 9 despite any difference in the perceived exertion. 10 Generally, NW is characterized by a submaximal regular increase of both heart rate (HR) and cardiac output together with a reduction of peripheral vascular resistance, to support the contemporaneous work of a big volume of muscle mass not requiring the expression of high intensity strength. According to the walking speed and the ground characteristics, NW may be a whole-body aerobic or alternated aerobic/anaerobic discipline. For example, interval training NW was used in obese subjects, to increase energy expenditure and weight loss. 11
Since outdoor physical activity seemed to be more effective than indoor activity, and it could therefore increase the adherence to exercise, 12 this systematic review and meta-analysis aimed to summarize and analyze the effectiveness of NW interventions on the physical fitness, the body composition, and the quality of life in the elderly population.
Methods
Study design
This is a systematic qualitative review and meta-analysis of the literature, aimed to analyze the effects of NW programs on the physical fitness, the body composition, and the quality of life in the elderly population. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and flow chart diagram were used as a reporting structure for this systematic review and meta-analysis. 13,14
Literature search
Literature research was conducted from June to July 2017. The keyword “Nordic Walking” associated with “elderly” AND/OR “aging” AND/OR “old subjects” AND/OR “aged” AND/OR “older adults” was used in the online databases MEDLINE, Embase, PubMed, Scopus, PsycINFO, and SPORTDiscus.
Inclusion and exclusion criteria
Only studies published in indexed and peer-reviewed journals, written in English language, were considered for this review. To be included, articles needed to meet the following criteria, formulated on the base of the PICO model 14,15 : (a) including subjects ≥60 years old; (b) delivering a supervised or a not supervised NW training intervention; (c) the presence or not of the control group, with different characteristics (sedentary, other exercise intervention); (d) physical fitness, body composition, and quality of life evaluations; and (e) randomized controlled trials (RCTs), non-RCTs, quasi-experimental design. Both males and females from all races and different states of health were included. Furthermore, only original articles were accepted for the analysis. All studies not evaluating outcomes through pre- and postintervention comparisons, as well as cross-sectional studies and case reports, were excluded. Published abstracts, dissertation materials, or conference presentations were not considered eligible documents.
Study quality assessment
The quality of the studies was assessed applying an adapted nine criteria checklist provided by the Cochrane Collaboration Back review Group. 16 As in previous reviews, 4,17 the checklist had to be marginally adapted to rate the strength of the evidence. Each study in the review was scored based on the following nine criteria: (1) “Was the method of randomization adequate?”; (2) “Were the groups similar at baseline regarding the outcome measures?”; (3) “Were inclusion and exclusion criteria adequately specified?”; (4) “Was the dropout rate described adequately?”; (5) “Were all randomized participants analyzed in the group to which they were allocated?”; (6) “Was the compliance reported for all groups?”; (7) “Was Intention-to-treat analysis performed?”; (8) “Was the timing of the outcome assessment similar in all groups?”; and (9) “Was a follow-up performed?”. When the study provided a satisfactory description, a positive value was assigned (+). If the criterion description was considered absent, unclear, or lacked the specified content, a negative value was assigned (−). A study was qualitatively judged as high quality if it showed a positive score on 5 to 9 of the criteria; otherwise, it was considered a low quality study.
Data extraction and synthesis
Two researchers independently examined all abstracts of the sourced studies from the literature. Suitable studies were analyzed with major detail for meeting eligibility criteria. Additional articles were sourced by reviewing the reference sections. A final quality eligibility check of each study was performed by the two researchers. The individual searches were combined, compared, and reviewed for applicability, where a consensus was made regarding study inclusion. In case of discrepancies, the review process was repeated, and a third researcher was consulted. A K-Cohen's coefficient of 0.98 indicated a perfect agreement between researchers; one study was excluded because subjects were aged lower than 60 years. 18 Quality assessment using the modified Cochrane methodological quality criteria was then independently applied and discussed before final quality scores were assigned (Table 1). The same researchers who screened titles, abstracts, full texts, and references performed quality assessment. Several domains were identified for categorization of the study results. In particular, studies were analyzed in regard to static and dynamic balance, muscle strength, flexibility, aerobic capacity, cardiorespiratory parameters, body composition, lipid profile and glucose sensitivity, and quality of life.
Data analysis
Meta-analyses were performed using random-effect models, with confidence intervals set at 95%; effect size (ES) was calculated through Review Manager 5.3 software (Copenhagen, The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The ES was calculated as standardized mean difference ΔMean/SDpooled, where ΔMean is the difference between the postintervention mean of the NW and Control Group, and SDpooled is the mean of the post intervention standard deviation, summarizing the different tests evaluating the same parameter. Overall ES consisted on NW group compared with all the different control groups, including sedentary group (SG), walking training (WT) group, and resistance exercise (RE). Also ES of NW with specific control groups (SG or WT or RE) was calculated (Table 4). The ES is a measure of the effectiveness of a treatment, and it helps to determine whether a statistically significant difference is a difference of practical concern. Interpretation was performed according to Cohen's guideline where an ES value of 0.20 indicates a small effect, ES of 0.50 indicates a medium effect, and ES higher than 0.80 indicates a large effect. 19
Studies Description and Results
A total of 353 studies resulted from the literature search. Applying inclusion and exclusion criteria, 15 studies were considered eligible for this review (Fig. 1). Sample sizes ranged from 18 to 95 subjects, with age ≥60 years old. Interventions lasted from 6 to 35 weeks, with a frequency of two or three times per week. Table 2 summarized the characteristics of the studies. Finally, Table 3 reported all results of the included studies.
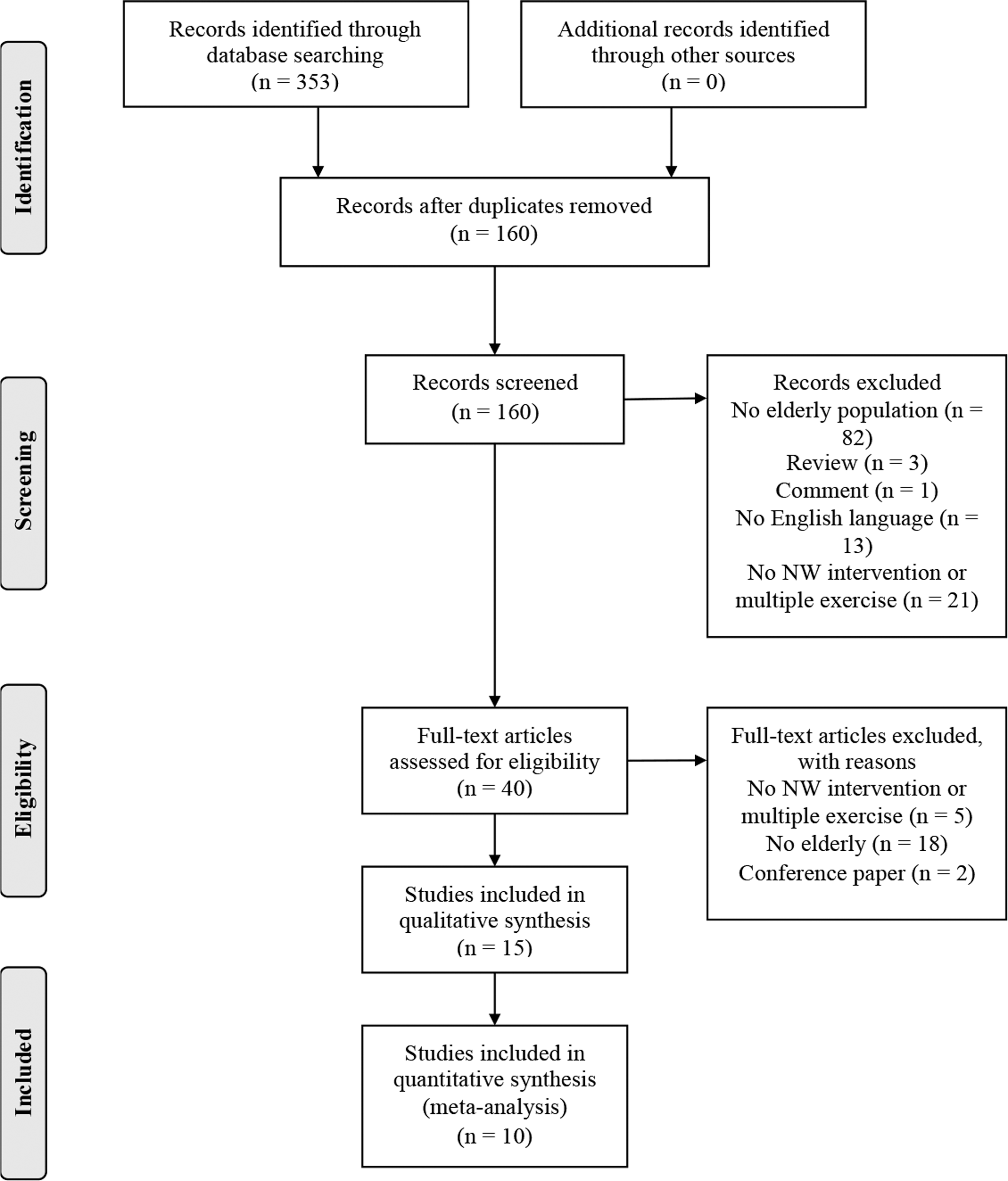
Flow chart of the literature research. In the edification section, there is the number of total articles found during the literature research. During the screening, first were removed double articles. Second were removed abstracts that did not meet inclusion criteria. Eligibility reported the number of full text read. Articles that did not meet the inclusion criteria were removed. Included studies were analyzed in the review.
CG, control group; d/w, day/week; F, female; HE, home exercise; HO, hip osteoarthritis; HR, heart rate; LVD, vitamin D concentration less than 20 ng/mL; M, male; MVC, maximal voluntary contraction; MVD, vitamin D concentration more than 20 ng/mL; noRCT, no-completely randomized controlled trial; NoSup, unsupervised; NW, Nordic Walking; Q-E, quasi-experimental; RCT, randomized controlled trial; RE, resistance exercise; RPE, rate of perceived exertion; Sup, supervised; WT, walking training.
Data are expressed as mean ± standard deviation; Δ (observed change mean) ± standard deviation; mean ± (CI).
p < 0.05, *within group comparison, **between groups comparison.
T0, test at baseline; T10, test after 10 weeks; T35, test after 35 weeks; T4, test after 4 weeks; T8, test after 8 weeks; T2m, test after 2 months; T4m, test after 4 months; T12 m, test after 12 months.
ag/ant, agonist/antagonist; AI75, Augmentation Index corrected at heart rate 75 per minute; AP, anaerobic point; ASAS, The Arthritis Self-Efficacy Scale; AT, anaerobic threshold; BBS, Berg Balance Scale; BDI, Back Depression Inventory; BF, body fat; BMI, body mass index; COP, center of pressure; CRP, C-reactive protein; DBP, diastolic blood pressure; EC, eyes closed; EO, eyes open; EPEcomp, end point excursion; FAS, Fullerton Advanced Balance Scale; FFM, fat-free mass; FRT, Functional Reach Test; FwRT, Forward Reach Test; GDS, Geriatric Depression Scale; HDL, high density lipoprotein; HG, handgrip test; HOMA-IR, Homeostasis of Model Assessment of Insulin Resistance; HR/24 h, heart rate of 24 hour; k-ext, knee extension; k-felx, knee flexion; KHCFAT, Korean Health Compliance Frailty Assessment Tool for the Elderly; LDL, low density lipoprotein; LEFS, Lower Extremity Functional Scale; MAP, mean arterial pressure; MOS, 15 s marching on the spot; MXEcomp, maximum excursion; n.d., not displayed; PK, peak; PKTQ, peak torque; PSQI-K, Korean version of Pittsburgh Sleep Quality Index; SBP, systolic blood pressure; SBP1, first peak radial systolic blood pressure; SBP2, second peak diastolic blood pressure; SF-36, Medical Outcomes Study Short Form; SL, single left; SMI, Skeletal Muscle Mass Index; SMM, skeletal muscle mass; SR, single right; SVcomp, mean of the four conditions of Clinical Test of Sensory Interaction for Balance; TBW, total body water; TC, total cholesterol; TG, triglyceride; TSC, time 10-step climbing test; TUG, time up and go; UwRT, upward reach test; WC, waist circumference.
Four studies were classified as high quality 20 –23 and 11 as low quality. 24 –34 Moreover, 5 studies reported the timing of outcome assessment, 24,25,27,28,31 9 studies executed randomization procedures, 20 –23,26,29,31,32,34 4 reported the compliance of the intervention, 20,23,25,28 10 the dropout rate, 20 –24,28,30,31,34 2 used the intention-to-treat analysis, 20,23 3 a blinding evaluator, 21 –23 and 1 executed a follow-up evaluation. 23
Static and dynamic balance
Four studies evaluated static balance with field and laboratory tests. After 12 weeks of NW training were recorded an improvement in the static balance (One-leg Stance test 133.9% 29 ; Functional Reach Test (FRT) 6.3% 28 ; Forward Reach Test 0.9%, 22 and Upward Reach Test 2.2% 22 ). Only one study found statistical difference with the laboratory evaluation with a force platform in open eyes condition (3%). 24 Comparing NW and SG, ES suggested that NW had a negative effect on static balance (ES = −0.72), while NW seemed to produce similar effects than WT (ES = −0.08) and RE (ES = −0.07).
In seven studies dynamic balance was evaluated by 8-foot up and go 20,23,24,27,28 and Time Up and Go test. 26,30 Significant improvements after 8 weeks (16.9% 23 ), 12 weeks (4.7% 28 ; 9.3% 26 ), 16 weeks (15.3% 23 ), 35 weeks (7.6% 30 ), and 1 year (20.3% 23 ) of NW training were recorded, whereas laboratory evaluation reported no significant changes after 9 weeks. 20 In comparison with the different control groups, ES suggested a small-to-medium effect on dynamic balance (SG = 0.30; WT = 0.30; RE = 0.33).
Functional balance was evaluated in two studies with the Fullerton Advanced Balance Scale and the Berg Balance Scale (BBS). In both, significant improvements of 6.2% 30 and 4.5% 21 after 35 and 6 weeks of NW were found. ES showed a medium to large effect of NW in the functional balance compared with SG (0.62), while NW seemed to carry out comparable effects of WT (ES = 0).
Muscle strength
Eight studies analyzed muscle strength changes after a NW program. Lower limb strength evaluated by the sit-to-stand test recorded a significant improvement of 25.9%, 29 22.4%, 31 12.6%, 28 9.5%, 27 and 10% 24 after 12 weeks of NW, an increase of 10.7% 23 after 8 weeks, 15.3% 20 after 9 weeks, 13.6% 23 after 16 weeks, and 17.9% 23 after 1-year follow up. Ossowski et al. 26 measured isometric knee extension and flexion strength. Twelve weeks of NW induce an improvement of 11% and 22.1% in peak torque knee isometric extension and flexion. 26 No significant changes were found after 35 weeks of NW, evaluated by the five-times sit-to-stand test. 30 Analyzing NW effects on lower limb strength with the different control groups, ES showed a small-to-medium effect (0.43, NW vs. SG), such as compared with RE (0.39). Whereas NW and WT seemed to indicate similar effects.
Upper limb strength evaluated by the Arm Curl 30s test showed an improvement of 19.7% 20 after 9 weeks of NW, and an improvement of 19.7% 31 and 11.6% 28 was found after 12 weeks, whereas no statistical difference was found in Lee's 12-week NW intervention. 29 Song et al. evaluated the upper limb strength also by Handgrip test, recording an increase of 11.8% after 12 weeks of NW. 31 In comparison with a SG, ES analysis showed that NW had a medium-to-large effect on muscle strength (0.74). On the contrary, WT and RE seemed to have the same effects.
Flexibility
Four studies examined muscular flexibility. After 12 weeks of NW, back scratch recorded a significant improvement in upper limb flexibility (44.6% 28 ), such as sit-and-reach test in lower limb flexibility (75.4%, 28 175% 27 ), whereas after 9 weeks, an improvement of 92.5% only in Sit-and-reach test was found. 20 Comparing NW with WT and RE, NW was more efficient than WT to enhance the lower limb flexibility (0.47), 28 and it was also more efficient than RE to improve the upper limb flexibility (0.41). 28 Compared with SG, NW did not produce any effects on upper limbs and lower limbs.
Aerobic capacity and cardiovascular outcomes
Nine studies analyzed aerobic capacity with field and clinical laboratory test. Only one study found no significant increases with field test. After 6 weeks of NW training, 6’ walk test improved by 22.3% 21 and by 13.9%, 34 such as after 8 weeks (7.5% 23 ), 12 weeks (10.1% 26 ), 16 weeks (13.3% 23 ), and 1-year follow-up (14.3% 23 ). 12’ walk test increased by 10.9% 28 and 5-m walk test increased by 14.3%, 21 both after 6 weeks of NW. Furthermore, 2-minute step test recorded an improvement of 14.2%, 20 9%, 27 and 9.4% 30 after 9, 12, and 35 weeks of NW intervention. In addition, 15-second marching on the spot test recorded significant improvement after 8 weeks, 16 weeks, and 1-year follow-up. 23 ES of 0.92 showed a large effect of NW compared with SG, as well as in comparison with RE (ES = 0.75). On the contrary, WT was more effective than NW in improving this specific capacity, with a small effect in favor of WT (ES = −0.21).
Three studies evaluated NW effects on cardiovascular outcomes. On one hand, significant improvements in duration of effort (14.1%), maximum effort load (13.4%), VO2max (13.6%), and systolic blood pressure (SBP) (3.6%) were recorded after 6 weeks. On the other hand, no significant changes were found in time at Anaerobic threshold, O2-pulse, diastolic blood pressure (DBP), and daily HR. 34 In addition, 12 weeks of NW proved to produce a significant decrease in SBP (4.4%), DBP (3.9%), average value of arterial blood pressure (4.1%), first and second peak of SBP (3.6% and 4.5%), and in augmentation index corrected at HR 75 per minute (2.5%). 33 Kortas et al. found significant improvement in VO2max after 35 weeks of NW (2.4%). 25 An ES of 0.23 indicates a small effect on cardiovascular outcomes.
Body composition
Six studies analyzed NW effects on body composition. Right 8 weeks of NW did not produce any significant changes in the body composition evaluated through bioelectrical impedance analysis, 32 while 12 weeks of NW produced a decrease in body weight (1.6%, 26 1.7%, 31 4.1% 33 ), in body mass index (BMI) (1.5%, 26 2%, 31 3.7% 33 ), in percentage of body fat (3.8%, 31 5.3% 26 ), and in waist circumference (2.4%), 33 such as an increase in muscle mass (3.9%, 31 2.1% 26 ). Kortas et al. found significant reduction in body weight (0.9%), percentage of body fat (4.8%) and total body water (0.9%), and increase in muscle mass (1.1%) after 35 weeks of NW. 25 Only two studies compared NW with a SG, and an ES of 0.30 suggested that 12 weeks of NW produces a small effect on body composition variation. 26,31 Comparing NW with WT, ES indicated that the two types of training were similarly able to modify the body composition outcomes (0.07).
Lipid profile and glucose sensitivity
In three studies lipid profile was evaluated. Twelve weeks of NW produced a significant reduction of total cholesterol (5.8% 31 ) and triglyceride levels (7.1% 31 ). In particular, high density lipoprotein (HDL) increased in two studies (15.4%, 31 6.4% 27 ) and decreased in another one (3% 33 ), but no significant changes in low density lipoprotein (LDL) were found. In detail, NW had a medium-to-large effect compared with SG (ES = 0.67), while after a WT and a NW training lipid profile was modified. 31
Glucose sensitivity showed significant modification with a concurrent reduction in C-reactive protein (20% 33 ) and Homeostasis of Model Assessment of Insulin Resistance (10.1% 33 ).
Quality of life
Four researches focused on depression, fragility, sleep quality, pain, and lower limb functional capacity. Six weeks of NW training did not produce significant improvements in pain score and lower limb functional capacity, 21 while longer intervention proved significant improvement in pain, 23 depression scale, 29,32 fragility index, 29 and sleep quality. 32 In particular, depression symptoms showed significant changes after NW training, with an improvement of 53.5% 32 and by 56.5% 29 after 8 and 12 weeks of training. Moreover, a large ES classified NW as a physical activity more effective than WT (1.132) and RE (1.0729) to reduce depression symptoms.
In addition, improvements in sleep quality (63.5% 32 ) and frailty index (34.4% 29 ) were found. In detail, large ES in sleep quality comparing with WT (1.09), 32 and in frailty index comparing NW with RE (0.81), 29 was found (Table 4).
AP, anaerobic point; AT, anaerobic threshold; BBS, Berg Balance Scale; BDI, Back Depression Inventory; BF, body fat; BMI, body mass index; CI, confidence interval; COP, center of pressure; DBP, diastolic blood pressure; EPEcomp, end point excursion; FAS, Fullerton Advanced Balance Scale; FFM, fat free mass; FRT, Functional Reach Test; FwRT, Forward Reach Test; GDS, Geriatric Depression Scale; HG, handgrip test; HR/24h, heart rate of 24 hour; LEFS, Lower Extremity Functional Scale; HDL, high density lipoprotein; k-ext: knee extension; k-felx, knee flexion; KHCFAT, Korean Health Compliance Frailty Assessment Tool for the Elderly; LDL, low density lipoprotein; MXEcomp, maximum excursion; NW, Nordic Walking; PK, peak; PKTQ, peak torque; PSQI-K, Korean version of Pittsburgh Sleep Quality Index; RE, resistance exercise; SBP, systolic blood pressure; SG, sedentary group; SMI, Skeletal Muscle Mass Index; SMM, skeletal muscle mass; SVcomp, mean of the four conditions of Clinical Test of Sensory Interaction for Balance; TBW, total body water; TC, total cholesterol; TUG, time up and go; UwRT, Upward Reach Test; WT, walking training.
Discussion
The aim of this systematic review was to summarize and analyze the effects of NW training on physical capacity, body composition, and quality of life in elderly people. The results showed that NW was capable to produce improvements on strength, balance, flexibility, body composition, aerobic capacity and cardiopulmonary outcomes, lipid profile, glucose sensitivity, and quality of life in elderly. Nevertheless, the low quality and the heterogeneity of the studies suggested the needs of larger high-quality clinical trials to increase evidence about the effectiveness of NW.
In this research analysis, 16 studies compared NW training to other type of exercise programs (n = 7) 21 –23,28,29,31,32 or to sedentary groups (n = 6), 20,26,28,30,31,34 while four studies had not the control group. 24,25,27,33 However, NW for elderly population indicatively followed the American College of Sport Medicine (ACSM) training recommendations for aerobic activity 2 with the advantage in the use of poles to ensuring the safety in frail elderly.
Static and dynamic balance
Balance ability is an important physical capacity since it is related to fall risk. Indeed, all year people who fall are about 30% over 65, with higher rates over 75 years old. 35 The largely used definition of body balance was related to the bodily capacity in the contrast of external forces, to maintain body stability and postural control. Four studies evaluated the static balance, showing significant and clinically meaningful improvements after 12 weeks of NW. Comparing NW with WT, RE, and SG, RE intervention induced the higher improvement on the static balance (+10.6%), similarly to the WT (+9.7%), while NW showed a lower increase (+6.3%). According to ES analysis, WT and RE interventions seemed to be more effective than NW alone to improve the static balance. Unexpected results were the ES of NW compared with the SG. In fact, NW seemed to have a negative effect on the static balance (FRT), despite the significant improvement. We speculated that there was a baseline difference between NW and SG that finally affected the computing of the ES (which resulted as negative), despite the improvement on NW and the concurrent decrease on SG. 28 In contrast, Lee and Park found NW more effective than RE to improve static balance, 29 as initially expected by the same authors and confirming their hypothesis.
NW showed improvements in dynamic balance, but with diverse results. Differently from the static, which these effects appeared as not completely definite, dynamic balance has been clearly influenced showing a general positive outcome after the training protocols. In particular, after 1-year follow-up evaluation of NW, a higher improvement was reported. 23 Analogously, 35 weeks induce 7.6% increase in dynamic balance, 30 such as 4.7% improvement after 12 weeks, 28 even if in a lower extent. The duration of the protocols seemed to have a role in the magnitude of change, in this case, with higher changes in longer duration protocol. Finally, static and dynamic balance, simulating activity of daily life, were quantified using FAS and BBS. In both studies, 21,30 significant improvements were detected. NW has medium-to-large effect after 35 weeks intervention, 30 while NW and WT influenced functional balance in the same manner. 21
Muscle strength
NW is characterized by an active involvement of lower and upper limbs, guaranteeing potential benefits for both upper- and lower body. Among the five studies aimed to analyze NW effects on strength, one was defined as a high quality study comparing the intervention group with a sedentary group, 20 and one high quality compared with resistance group, 23 reporting a significant improvement in lower 20,23 and upper limb strength, 20 according to the other two studies found significant improvement after 12 weeks of NW. 28,31
Data analysis showed a general improvement of strength in both conditions of NW and WT. Comparing the two modalities, upper- and lower limb strength were changed with similar effects, lightly differently from upper- and lower body. As expected, participants who underwent WT showed a positive trend in developing higher lower limb strength (0.36). 31 On the other side, upper limb strength was improved in NW participants (0.3631). These results are corroborated if comparing muscular activation, in fact EMG signals showed a higher percentage of activation of upper limbs in NW, with an inferior activation of lower limbs. 10 From a different perspective, comparing NW versus RE, both studies after 12 weeks had different findings. 28,29 Lee and Park study showed significant improvement in the overall strength with larger effects on lower limb and medium effect on upper limbs in favor of NW 29 ; contrarily, Takeshima et al. showed significant improvements with small effects on lower limbs and medium effect in the upper ones in favor to the RE. 28 These results could be due to the difference in the walking surface used in the two studies. In Takeshima et al. protocol, NW was performed on an asphalt track, 28 while Lee performed two sessions indoor with treadmill and one session outdoor in hilly park or mountain with a broad increase in the muscular commitment. 29
Flexibility
Flexibility, and also the range of motion, plays a key role in the development of the activities of daily living. In this article, limited findings were reported for the flexibility. Indeed, only four studies focused on upper and lower limb flexibility, and only two compared it with different groups, and baseline evaluations were largely different among them. 20,28 Lower limb flexibility has been found to be significantly improved in two studies, but Parkatti et al. found a larger improvement despite the shorter training period. Probably, the introduction of specific stretching exercise and postures in the warm-up and cooldown program had a pivotal explanation in the progress of this capacity. 20 Despite no significant variations recorded for the upper limb flexibility, ES showed a small-to-medium effect on shoulders. In this case, it is likely that the significance in the lower limb and not in upper flexibility could be ascribed again to the stretching specific intervention that was more focused on the lower bodily region than in the upper one. 20 This hypothesis agreed with Kortas et al. that found a significant improvement only in upper limb flexibility due to the specific exercise of mobility performed for shoulder, and not for the lower limb. 27
NW seemed to induce the higher percentage of improvement after 12 weeks of intervention, compared with WT and RE, 28 while upper limb flexibility improved only in one study. Takeshima et al. showed significant changes in NW, WT, and RE with the higher percentage in RE. 28
Aerobic capacity and cardiovascular parameters
Aerobic capacity was largely analyzed in the included studies, comparing NW effects with SG, WT, and RE. In general, the involvement of upper- and lower limb determined improvements in the aerobic capacity after NW programs. With more details, NW produces a small-to-medium effect (0.4620), a medium-to-large effect (0.6230), and three large effects (1.11, 34 1.62, 28 1.0526). One hypothesis for this difference could be endorsed to the weekly frequency of the training, with larger ES when NW was performed thrice per week. 26,28,34 Comparing NW and RE interventions, improvements were found in the aerobic capacity for both modalities. As expected, NW intervention showed a medium-to-large effect on aerobic capacity compared to RE. 28 Figueiredo et al. include NW and a WT into a rehabilitation program to analyze its effect and feasibility. In this way, the upper limb activity was compared in terms of benefit for the aerobic component. Twenty minutes of NW in two weekly sessions, for 6 weeks, significantly increased the distance scored in the 6-minute walking test, with a 22.3% improvement in favor of the NW group. 21 Takeshima et al. found similar improvements on the aerobic capacity comparing NW with WT (10.6%, 10.9%). Although ES showed a small-to-medium effect in favor of the WT (−0.45), 28 this result appeared as unexpected and in contrast with the literature. The activity (muscular) of the upper body during NW increased the energy expenditure with higher oxygen consumption and HR between NW and WT performed at the same walking speed. 10 In Takeshima et al. study, both interventions were performed for all participants with a HR range of 100–120 bpm. This standardized intensity could have affected the results, because investigators did not consider the subject variability, with a different exercise stimulus leading to potential different effects of training in each subject. 28 Moreover, in that protocol, the optimal economical individual speed was not considered. This speed could be different from that of walk, belonging in turn to different training intensities. 10
Only one study analyzed cardiovascular parameters. NW intervention determined a positive impact in the OMNI scale, which was similar to the Borg Rate of Perceived Exertion (RPE) scale, indicating the bodily adaptive response to the physical effort; this improvement (0.80) took place with a concurrent improvement in the VO2max (0.70). 34 O-2 pulse, predictive to assess the efficacy of cardiovascular parameters, was examined by Vaitkevicius et al.; their study included participants aged ≥80 years old, finding a significant improvement in this parameter after 6 months of exercise. 36 Chomiuk et al. did not find a significant improvement in the O-2 pulse after 6 weeks of NW. It is likely that adaptation needs longer periods to be revealed, even if a small-to-medium effect was found (0.31). 34
Body composition
NW and WT are two aerobic activities able to ameliorate the body composition in elderly people. Twelve weeks of NW induced meaningful change in terms of weight loss, BMI, and waist circumference. 26,31,33 Compared with a SG, the effects were quantified as small to medium, in the reduction of weight (0.34), BMI (0.33), and body fat percentage (0.43). 26,31 The comparison with the walking alone protocol should be interpreted considering that two studies administered the same intervention (three-time per week, 50–60 minutes with progressive intensities monitored through HR and/or RPE), the only difference was the duration of training which was 832 or 12 weeks. 31 Fat-free mass (FFM) and basal metabolism were significantly improved in both NW and WT, with greater changes in the NW group. Effect on FFM was influenced in medium-to-large effect (0.53), while basal metabolism in small-to-medium effect (0.23). BMI, skeletal muscle mass, and body fat percentage showed contrasting findings, despite the two similar exercise protocols. Probably, the uncontrolled diet could have influenced these results; more concretely, in one article all improvements were in favor of the NW group, 32 in the other in favor of the WT. 31
Lipid profile and glucose sensitivity
In obese menopausal women, 6 weeks of NW induced a significant reduction of glucose sensitivity. 37 Also in the Kawamoto et al. study, glucose tolerance was significantly improved after their 12-week NW protocol, while no significant changes were recorded on the lipid profile. 33 Despite data appearing as clear, these clinical outcomes need deeper analyses and a control group to compare the results. With similar trend also the interpretation for the lipid profile should be performed since only two studies analyzed the effects of NW; the first one comparing it with SG and WT. Significant changes after 12 weeks of NW were found in the total cholesterol (0.98), HDL (0.55), and triglycerides (0.43). Conversely, LDL change was not statistically significant, despite the medium-to-large effect on NW (0.75). 31 Comparing NW with WT, TC, and LDL resulted as modified with the same degree of influence, while WT generated a small-to-medium effect on triglyceride and HDL. 31 In the light of these results, it is not possible to quantify the minimal dose, in terms of frequency and quantity, as well as intensity of NW, to determine a meaningful improvement in lipid profile.
Quality of life
Cognitive decline, depression, and decrease of sleep quality are common age-related conditions due to the aging. About 40%–70% of elderly suffer from chronic sleep disturbances, with related physical, social, and psychological weakness affecting the activity of daily living. It has been demonstrated that regular physical activity is associated with better sleep quality. 38 Park and Yu found significant improvement after 8 weeks of WT and NW in the quality of life and sleep quality, both performed from 40% to 75% of HR. 32 According to data reported in another study, regular moderate-intensity exercise, performed at 60%–75% of HR, improved the sleep quality in elderly with moderate sleep complaints, increasing also sleep duration. 39 Compared with RE, 12 weeks of NW have larger effects in quality of life and depression. This large effect could be influenced by the outdoor sessions of NW, which were potentially implicated as beneficial in the depressive symptomatology than indoor activities. 40 Bieler et al. analyzed the short and long effects of NW, RE, and home exercise (HE) in the quality of life of elderly with hip osteoarthritis. The main findings were that NW had the major improvement in quality of life than RE and HE in short and long term. 23
Limitations
There are some limitations that should be considered in the application of our findings. First, the majority of participants are women. Future studies need to recruit more gender-balanced group, with specific intervention effects, including compliance and dropout ratio. Second, the low quality and number of studies limited the reliability of our consideration. Indeed, only six studies reported a randomization and specified the homogeneity of groups at baseline, and the range of compliance was explicated only in three studies. The scientific evidences of NW training take advantage from relevant elements such as intensity and compliance, to quantify the dose–response of outcomes analyzed in this review. Moreover, the environment of the intervention is an important determinant for the analysis. Indeed, indoor and outdoor exercise can result in different outcomes, such as the ground (plane or hilly). Finally, the comparison between different types of training programs potentially limits the analysis of the effects on NW intervention. Future studies should also better identify intensity and progression targets of the training, investigating the potential to incorporate NW programs with other exercise modalities to promote overall wellness in elderly populations, especially for the muscular strength and balance.
Conclusions
NW can be considered as a safe and accessible form of aerobic exercise for the elderly population, able to improve aerobic capacity, muscle strength, balance performance, and quality of life. Only one study reported some adverse effects (low back pain, hip pain, and one fall); thus, it can be considered as a safe and advisable activity for elderly. Although further research is needed, our results indicate that clinicians who consider NW for exercise prescription are suggested to recommend NW at least twice per week at moderate to vigorous RPE (from 13–14 to 15–16) depending on current conditioning. Moreover, NW could be incorporated with supplemental strength exercises, especially for the lower limb and balance exercise, such as Pilates training.
Footnotes
Author Disclosure Statement
No competing financial interests exist.