
Abstract
Comprehensive geriatric assessment (CGA) is a multidimensional and multidisciplinary diagnostic process focused on determining the clinical profile, pathological risk, residual skills, short- and long-term prognosis, and personalized therapeutic and care plan of the functionally compromised and frail older subjects. Previous evidence suggested that the effectiveness of CGA programs may be influenced by settings where the CGA is performed [i.e., hospital, posthospital discharge/long-term care facilities (LTCFs), or community/home] as well as the specific clinical conditions of older frail individuals. In this scenario, CGA and quality of care in LTCFs have been a challenge for decades. In the present article, we systematically reviewed evidence from the last three decades of clinical research devoted to systematic implementation of CGA programs in LTCFs, that is, nursing homes, care homes, residential homes, and rehabilitation facilities. In the United States, all LTC residents must undergo a CGA on a regular basis on admission to a facility, prompting the development of the Resident Assessment Instrument (RAI) Minimum Data Set, a specific CGA-based assessment tool in this population. In the LTCF setting, the present reviewed evidence suggested that most complex older subjects may benefit from a CGA in terms of improved quality of care and reduced hospitalization events and that CGA must be standardized across healthcare settings to promote greater health system integration and coordination. In the LTCF setting, particularly in nursing homes, other new and promising CGA programs have also been proposed to develop rapid screening CGA-based tools to enhance in the future the ability of primary care physicians to recognize and treat geriatric syndromes in this setting. However, at present, the interRAI suite of instruments represented an integrated health information system that has the potential to provide person-centered information transcending healthcare settings.
Introduction
T
CGA and the Interdisciplinary Approach to the Older Subject
CGA is sometimes termed geriatric evaluation and management (GEM), particularly when geriatric assessment programs combine geriatric evaluation with management. 5 Although there is no universal agreement on specific criteria used by CGA programs to evaluate patients, the main components of the CGA are functional status, mobility, gait speed, cognition, mood and emotional status, financial concerns, nutritional status, comorbidities and polypharmacy, geriatric syndromes (all risk, delirium, urinary incontinence, dentition, and visual or hearing impairments), disease-specific rating scales (gait dysfunction, parkinsonism, and dementia), goals of care, and advanced care planning. 2,3 A patient's social and environmental situations also are evaluated, with focus on the social interactions network, social support needs and resources, and environmental adequacy and safety. The CGA uses validated geriatric scales and tests to produce an inventory of health problems, which can then serve to develop an individualized geriatric intervention plan. An interdisciplinary team approach is employed in most CGA programs to assess patients, interpret results, and pool expertise in working toward common goals. The range of healthcare professionals working in the assessment team varies based on the services provided by individual CGA programs, usually organized around a core team whose members see every patient. In many settings, the CGA process relies on a core team consisting of a physician (usually a geriatrician), a nurse, and a social worker. When appropriate, specialists in several other disciplines either take part in the basic assessment or act as consultants with an extended team of physical and occupational therapists, nutritionists, pharmacists, psychiatrists, psychologists, dentists, audiologists, podiatrists, and opticians. These professionals are usually on staff in the LTC and nursing homes and are also available in the community. Access to and reimbursement for these services, however, have limited the availability of CGA programs. At present, CGA programs are moving toward a virtual team concept, in which members are included as needed, assessments are conducted at different locations, and team communication is completed through telephone or electronically. 6
CGA and Progressive Geriatric Care
Different models of CGA have been proposed in different healthcare settings to meet differing needs of older subjects. According to the concept of progressive geriatric care, 7 CGA is performed at varying levels of intensity in different settings and its content may vary with the healthcare setting. At the most intensive level, many older patients requiring acute hospital care are first admitted to an acute-care GEM unit, where they receive CGA from an interdisciplinary team in addition to treatment for their acute problems. 2,3 An inpatient approach would be to refer older patients admitted for a specific medical or surgical reason or to have all patients above a certain age receive preliminary screening to determine whether a full multidisciplinary evaluation is needed. An LTC approach would be to refer patients for CGA who are found to have problems in multiple areas during geriatric assessment screens. Major illnesses should also prompt referral for CGA, particularly for impaired functional status, increased fall risk, and cognitive and mood disorders.
In 1993, a seminal meta-analysis on different service-based interventions for older people provided a framework for the definition of inpatient and LTC models of CGA showing a benefit on short-term mortality, reduced institutionalization and readmission, improved cognitive functioning, and, for some models, improved physical functioning. 8 Since this meta-analysis, a number of studies have reported RCTs of hospital-based CGA programs. 9 –13 Moreover, there have been a number of systematic reviews and meta-analyses of various hospital-based subgroups of CGA demonstrating that patients who received CGA were more likely to be alive and in their own homes at the end of the scheduled follow-up and less likely to be living in residential care, compared with usual care. 14 –17 Furthermore, there was a reduction in the combined outcome of death or functional decline and an improved cognitive functioning, with wards that appeared to be more effective than mobile units. 18,19 In the present article, we systematically reviewed the body of evidence from the last three decades of clinical research devoted to the implementation of CGA programs in LTCFs, that is, nursing homes, care homes, residential homes, and rehabilitation facilities, analyzing the benefits arising from the application in these scenarios of CGA-based tools.
Methods
In the present systematic review article, we followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, adhering to the PRISMA 27-item checklist. 20 A literature database search was performed electronically through the U.S. National Library of Medicine (PubMed), Ovid MEDLINE, EMBASE, Google Scholar, Web of Science, and Scopus databases, combining the term “comprehensive geriatric assessment” with the following keywords: “mortality” OR “death” OR “outcome” OR “long-term care” OR “nursing home” OR “rehabilitation facility” OR “long-term care hospital” AND the following types of articles: “randomized controlled trial” OR “observational study” OR “systematic review” OR “meta-analysis.” The search was restricted to articles published in the English language from the beginning of the various databases used until April, 2017. In addition, a manual check on the reference lists in the articles and reviews identified was also conducted to seek any additional sources of information. The criteria for including the articles in this systematic review were RCTs, observational clinical studies, and systematic reviews/meta-analyses on the use of CGA in older people, including only reports conducted in LTCFs (i.e., nursing homes, care homes, residential homes, and rehabilitation facilities), independently from specific clinical conditions. The exclusion criteria were certain types of publications (letters to editors or single case reports) and patients with a mean age below 60 years.
Figure 1 shows the stages in obtaining studies for inclusion in the present report (PRISMA four-phase flow diagram). From 4965 articles identified with multiple electronic searches, we screened titles and abstracts of citations downloaded from the searches, identifying 1768 potential relevant articles chosen for a closer review. Excluding other 1722 articles not meeting inclusion criteria, we obtained full copies of the 46 potentially suitable reports for further assessment. After inclusion of 6 articles of interest from the reference lists of the selected articles and exclusion of other 37 articles, 15 studies met study eligibility criteria and were finally included in the overall systematic review (Tables 1 and 2). 6 –20 We did not use formal methods of assessment of the quality of the studies included in the present systematic review, but we described in depth the study design and sample together with principal results of the included studies in Tables 1 and 2. 21 –35
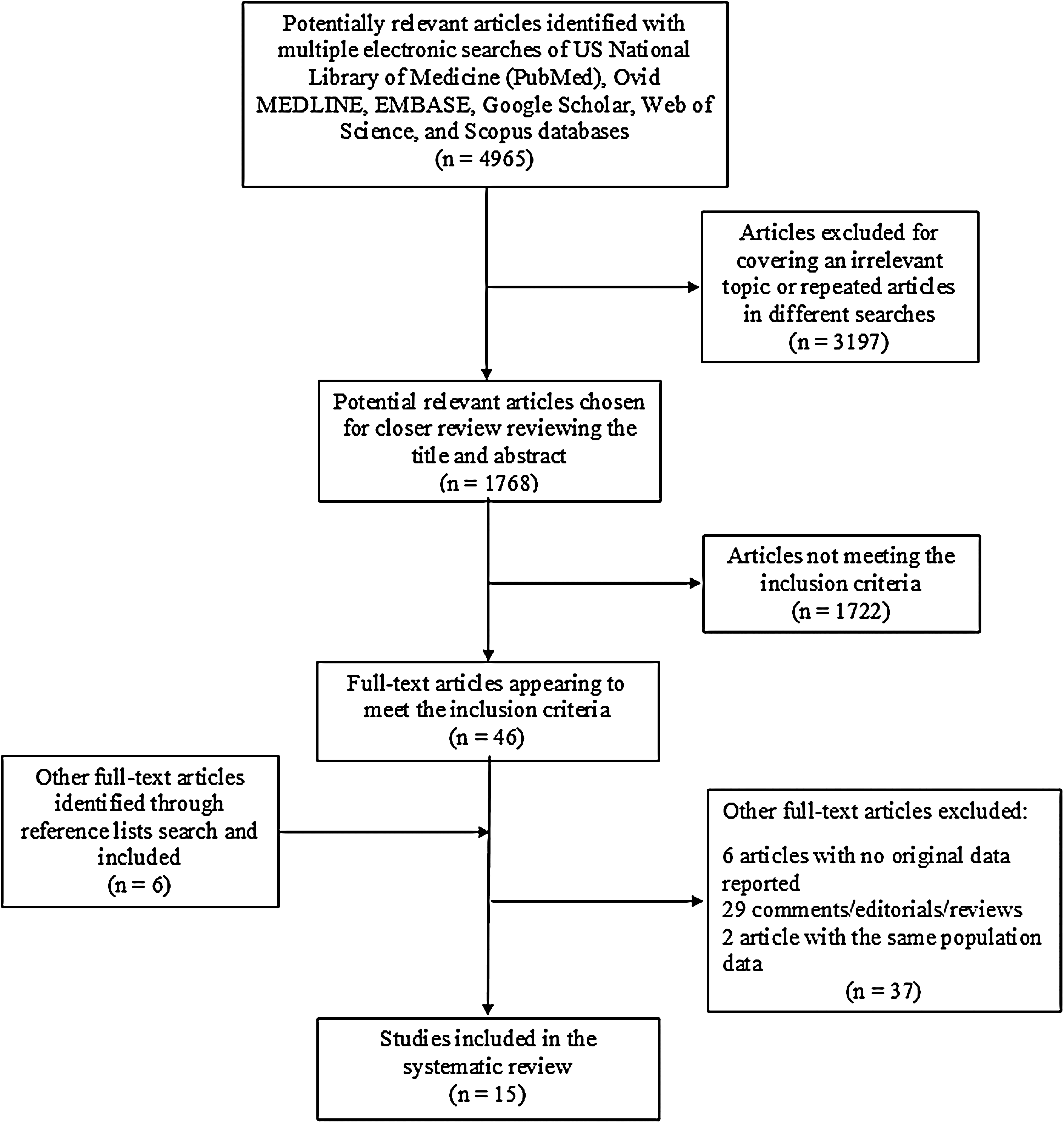
PRISMA four-phase flow diagram of retrieved and selected articles on systematic implementation of CGA programs in long-term care facilities, that is, nursing homes, care homes, residential homes, and rehabilitation facilities, analyzing the benefits that come from the application in these scenarios of CGA-based tools considering the results of randomized controlled trials, observational clinical studies, and systematic reviews/meta-analyses. CGA, comprehensive geriatric assessment.
MedPAR, Medicare provider analysis and review file; MAX, Medicaid analytical extract; LTCF, long-term care facility; RAI-HC, RAI-home care; CAP, client assessment protocol; QI, quality indicator; ADL, activities of daily living; IADL, instrumental activities of daily living.
CGA, comprehensive geriatric assessment; RACIP, Residential Aged Care Integration Program; interRAI PC, inter-Resident Assessment Instrument Palliative Care.
CGA in LTC Facilities
Specific assessment of InterRAI
The development of the Resident Assessment Instrument (RAI) Minimum Data Set (MDS) 36 in 1987 and its introduction in 1991 were prompted by LTC reforms endorsed by the United States (U.S.) government, requiring that all LTC residents undergo a CGA on a regular basis, on admission to a facility. InterRAI is a collaborative not-for-profit network of researchers and clinicians in over 30 countries committed to improving care for persons who are disabled or medically complex through the development, evaluation, and implementation of instruments for comprehensive assessment. The interRAI network was formed to promote and guide the use of the RAI-MDS instrument. Each interRAI instrument was developed for a particular population; however, they are all designed to form an integrated health information system, sharing a common language, and thus addressing clinical concepts consistently across instruments. In different care settings, the use of common measures enables clinicians and providers to improve care continuity, thus integrating care for individuals. Each interRAI instrument consists of items, outcome measures, assessment protocols, case-mix algorithms, and quality indicators (QIs) rigorously tested to establish their reliability and validity. A fully realized interRAI instrument includes a clinical data set, a training manual, and algorithms that generate Clinical Assessment Protocols (CAPs), scales (including screeners and severity measures), case-mix measures, and QIs. In 1995, a revised version of the RAI-MDS, the RAI-MDS 2.0, was developed, resulting in over 400 data elements, with improved reliability. 37 In 2005, the multinational consortium interRAI released the interRAI suite of instruments tailored to a specific healthcare setting. The interRAI suite of instruments contains CGA-based instruments developed for different healthcare settings (interRAI Home Care, interRAI Acute Care, interRAI LTC, interRAI Palliative Care, etc.). 38 In addition, a more recent version of the LTC assessment instrument, the interRAI LTCF, and an adaption of RAI-MDS 2.0, the MDS 3.0, have been released. At present, the interRAI LTCF instrument has not been widely implemented and MDS 3.0 has been implemented in the U.S. only.
The interRAI instruments enable detection of residents' strengths, needs, and potential risks to inform individualized care planning and monitoring. Data collected from residents in LTC are aggregated to produce indicators of the quality of care provided (i.e., QIs). One study examined 38 chronic care QIs, of which strong evidence for the validity of 12 of the QIs was found. 39 A systematic review on observational studies conducted in real-world conditions tested the validity and/or reliability of individual QIs (falls, depression, depression without treatment, urinary incontinence, urinary tract infections, weight loss, bedfast, restraint, pressure ulcer, and pain) with mixed results. This systematic review revealed the potential for systematic bias in reporting, with under-reporting of some QIs [pain, falls, and depression] and over-reporting of others (urinary tract infections). 40 In 30 urban Canadian nursing homes with a total of 94 care units, an observational study showed the necessity of facility-level and unit-level measurements when calculating QIs derived from RAI-MDS 2.0 data for pressure ulcer, antipsychotic with no diagnosis of psychosis, and pain. 41 Furthermore, RAI-MDS can be a valuable tool in targeting residents for a transition program from LTC to community.
Table 1 shows selected studies on CGA conducted in LTCFs using the RAI-MDS assessment tools. 8 –12,17,18 Secondary data from RAI-MDS assessments for an annual cohort of first-time admissions to nursing homes suggested that at 90 days, the majority of residents showed a preference or support for community discharge and many had health and functional conditions predictive of community discharge or low-care requirements (Table 1). 9 However, a validation study of the RAI-MDS conducted in four U.S. states suggested that the accuracy for identifying hospitalization events and payment sources in LTC with this CGA-based tool varied across the study states and should be evaluated carefully with regard to the intended uses of the data (Table 1). 10 In a longitudinal cohort study on newly admitted Icelandic nursing home residents, among RAI-MDS 2.0 variables and scales, significant predictors of mortality were age, gender, place admitted from, functional status, health stability, and social engagement (Table 1). 11 Recently, given the lack of findings on a psychometrically evaluated CGA for nursing home residents with palliative care needs, with outcomes that can be used for care planning, a protocol based on the Medical Research Council framework has been implemented to examine the effect of using the interRAI Palliative Care on the quality of palliative care in nursing homes. 42 In the future, the results of this study will provide CAPs (i.e., indications of problems that need addressing) and scales (i.e., Palliative Index for Mortality, PIM), which can be used to design, evaluate, and adjust care plans in this particular population. In a cluster RCT on 340 Dutch care home residents, in which the assessment included the LTCF version of the RAI, the intervention care homes had a significantly higher sum score of the 32 quality-of-care indicators, with significantly higher scores for indicators of good care in the areas of communication, delirium, behavior, continence, pain, and use of antipsychotic agents (Table 1). 12 In another cluster RCT conducted in Germany, home care residents working intensively with RAI-Home Care (using all tools of RAI, e.g., MDS, CAPs, and QIs, and including all home care residents) were significantly less hospitalized and fared slightly better according to ADL, instrumental ADL, cognitive skills, and quality of life compared with the control group (Table 1). 17 Comparing these two European RCTs (with the comparator usual care practice), in the Dutch study, 12 the primary care physicians were responsible for medical care and offered it on request without coordination or structured planning of care, while in the German study, 17 some care homes had limited implementation of the RAI-Home Care (using only some tools and not including all residents). Finally, given that oral health in nursing home residents is poorly addressed, an assessment tool such as the RAI-MDS 2.0 appeared to be key to monitoring and improving quality of oral healthcare. However, using data on 13,118 residents collected in a stratified random sample of 30 urban nursing homes in western Canada, RAI-MDS 2.0 oral/dental items likely significantly underdetected oral/dental problems and were not associated with well-proven predictors for oral health, indicating poor validity (Table 1). 18 At present, the potential effect on this issue of the interRAI LTCF with its modified oral/dental items and more frequent collection is unknown.
Other CGA programs for LTC facilities
Table 2 shows selected studies on CGA conducted in LTCFs not using the RAI-MDS assessment tools. 6 –8,13 –16 In 1990, a seminal RCT conducted in a GEM unit in a private U.S. rehabilitation hospital showed (in patients with a CGA intervention) less institutionalization in nursing homes, but no difference between the two groups in the mean number of days spent in healthcare facilities (acute care hospital, nursing home, or rehabilitation hospital) (Table 2). 6 These findings were confirmed in a 1-year follow-up of this RCT in which mortality and nursing home institutionalization decreased in subjects with a rehabilitation classification and CGA intervention. For subjects with a medical–surgical classification, the CGA intervention was associated with decreased cumulative use of nursing homes (Table 2). 8 In this RCT and its follow-up, 6,8 comparing usual care practice, neither the staff members of the GEM unit nor the investigators in the study were involved in the care of patients of the control group. In an observational study, CGA nursing home residents had a significantly greater number of diagnoses and ancillary services, showing also nonsignificant trends toward decreased mortality, fewer emergency department visits, and fewer drugs prescribed (Table 2). 7
In the LTCF setting, particularly in nursing homes, other CGA programs different from those of the interRAI have also been proposed. 43 In fact, the paucity of geriatricians and certified medical directors in the U.S. led to development of rapid screening CGA-based tools to enhance the ability of primary care physicians in nursing homes to recognize and treat geriatric syndromes. In Japan, to overcome this problem, the Kihon Index has been developed, 44 while in France, there was the Gerontopole screening tool. 45 In the U.S., Rapid Geriatric Assessment (RGA) has been developed to this aim as part of the Medicare Wellness Visit. 46 RGA consisted of simple screening tools for major geriatric syndromes as well as checking that the individual had an advanced directive. 47 All the screening tools have been extensively validated and were copyright free. These tools were the FRAIL for frailty, 48 the SARC-F for sarcopenia, 49 the Simplified Nutritional Appetite Questionnaire (SNAQ) for anorexia of aging, 50 and the Rapid Cognitive Screen for cognitive dysfunction. 51 The total screen takes 3–4 minutes to complete and can be done by office personnel in the physician's office. At present, RGA was successfully used on more than 1500 older persons and some recent RCTs, showing that simple exercise programs and nutritional intervention can reverse frailty and sarcopenia and slow cognitive deterioration, 52,53 may support the use of these rapid screens also in LTCFs, although the current evidence comes from a different setting.
In an RCT, the Residential Aged Care Integration Program (RACIP) intervention, including care coordination provided by gerontology nurse specialists, reduced the hospitalization rate in LTCF residents (Table 2). 13 In a recent systematic review on CGA used to assess palliative care needs in LTCF settings and validated for nursing home residents receiving palliative care, the interRAI Palliative Care and the McMaster Quality of Life Scale 54 were considered to be the most comprehensive tools to evaluate the needs and preferences of this particular population (Table 2). 14 This was a systematic review focused on psychometric properties of various CGA programs, while future research should aim to examine the effectiveness of the identified tools. Furthermore, recently, other classical CGA tools have also been modified for use in LTCFs (Table 2). 15,16 In fact, an adapted CGA, the LTC-CGA, has been modified and validated for use in LTCFs to better suit the LTC setting, including documentation of behavioral disturbances common in dementia, foot and dental care requirements, skin integrity, whether a legal next of kin has been appointed, and goals of care (e.g., whether resuscitation is to be attempted or hospital transfer for acute illness). 15 The LTC-CGA also includes a frailty measure that is a focused version of the CSHA Clinical Frailty Scale. 55,56 A mixed methods study on this tool has been conducted in 10 LTCFs in Halifax, Nova Scotia, Canada, reviewing 598 resident charts from pre- and postimplementation of the LTC-CGA, and qualitative findings suggested that the LTC-CGA may describe a clinical baseline health status that enabled timely and informed clinical decision-making (Table 2). 15 Another recent study explored the ability of nursing home residents to use two different mobile devices for a self-CGA with a modified MDS 3.0 converted to a format for use with a 6-inch mobile pad and a 3.7-inch mobile smartphone (Table 2). 16 All participants were able to use a 6-inch pad (average completion rate: 92.9%) and only 20% of the participants could complete the assessment with the 3.7-inch smartphone (Table 2). 16 This exploratory study suggested that nursing home residents may be able to use a mobile device to perform a self-CGA for assessment of their health status.
CGA programs for patients admitted to LTC facilities after acute hospitalization
CGA programs may also be useful to evaluate the recovery and outcome of older community-dwelling patients admitted to intermediate care (IC) in nursing homes after acute hospitalization. In a prospective observational study, the trajectory of recovery was divided into three groups: rapid recovery (able to return home after median 14 days in IC), slow recovery (requiring additional transfer to another nursing home after IC, but still able to return home within 2 months), and poor recovery (requiring transfer to another nursing home after IC and still in a nursing home or dead at 2 months) (Table 2). 19 Among CGA-based tools, slow or poor recovery was significantly associated with low scores on the Barthel Index and orthopedic admission, suggesting that CGA at admission may help to select appropriate caring pathways for different patient groups also in this setting (Table 2). 19 However, in older age, institutionalization following acute hospital admission is common and yet poorly described and CGA may help to characterize this particular population. In a retrospective cohort study of 100 people admitted to a single large Scottish teaching hospital and discharged to a care home, these individuals were predominantly female, widowed older adults who lived alone, with a diagnosed cognitive disorder or evidence of cognitive impairment (Table 2). 20 Family request, dementia, mobility, fall risk, and behavioral concerns were the commonest reasons for the decision to admit to a care home (Table 2). 20
Future Research Programs for CGA and Quality of Care in LTC Facilities
However, notwithstanding all these CGA-based tools, quality of care in LTCFs, particularly nursing homes, has been a challenge for decades and evidence to support consistent quality improvement strategies is still lacking. 57,58 Multiple international reports described suboptimal quality of care in nursing homes. 59,60 Therefore, a large, longitudinal, and focused research program called TREC (Translating Research in Elder Care) has been designed to collect comprehensive data from care providers and residents in Canadian nursing homes to improve quality of care and life of residents and quality of work life of caregivers. 61 Within the TREC research program, INFORM (Improving Nursing Home Care through Feedback On PerfoRMance Data) is a 3.5-year, three-arm, parallel cluster RCT that will be conducted on 67 western Canadian nursing homes with 203 care units in the three study arms, a standard feedback strategy and two assisted and goal-directed feedback strategies. 54 Interventions will target care unit managerial teams based on theory and evidence related to audit and feedback, goal setting, complex adaptive systems, and empirical work on feeding back research results. The primary outcome is the increased number of formal interactions (e.g., resident rounds or family conferences) involving care aides. Secondary outcomes are (1) other modifiable features of care unit context (improved feedback, social capital, and slack time), (2) care aides' quality of work life (improved psychological empowerment and job satisfaction), (3) more use of best practices, and (4) resident outcomes based on the RAI-MDS 2.0. 61 Outcomes will be assessed at baseline, immediately after the 12-month intervention period, and 18 months postintervention. INFORM is the first study to systematically assess the effectiveness of different strategies that feed back research data to nursing home care units to improve their performance. Results of this study will enable development of a practical, sustainable, effective, and cost-effective feedback strategy for routine use by managers, policy-makers, and researchers.
Conclusions
CGA is based on the premise that a systematic evaluation of frail older adults by a team of health professionals may identify a variety of treatable health problems and lead to better health outcomes. At present, no standard criteria are available to readily identify patients who are likely to benefit from CGA. Previous evidence from RCTs and large systematic reviews and meta-analyses suggested that the healthcare setting (i.e., hospital, posthospital discharge/LTCF, or community/home) as well as specific clinical conditions (older frail patients evaluated for preoperative assessment, admitted or discharged from emergency departments and orthogeriatric units, or with cancer and cognitive impairment) may modify the effectiveness of CGA programs. 2,3 In general, transcending healthcare settings, for frail and high-risk older patients, especially those recently hospitalized and those being considered for LTC, a CGA and follow-up program tailored on specific strengths and weaknesses is appropriate. 7 For older patients at medium risk, or subjects aged 75 years and older without severe chronic illness, a preventive home visit CGA and follow-up program may be appropriate. 7 For older patients at low risk, a program of periodic health risk appraisals, conducted through primary care or in tandem with primary care, could be appropriate in the frame of prevention programs of healthy aging. 7
In the LTCF setting, CGA and quality of care have been a challenge for decades. In this setting, the evidence from the present systematic review suggested that most complex older subjects may benefit from a CGA in terms of improved quality of care and reduced hospitalization events. In the LTCF setting, usual care practice provided by primary care physicians was the comparator in several of the reviewed RCTs; however, it is always difficult to separate the beneficial effect on the different outcomes of the expert input of geriatricians and specialized teams in CGA programs, as opposed to the technical aspects of CGA itself. However, some limitations should be reported for this systematic review article. Heterogeneity exists in the outcomes (community discharge, hospitalization events, quality of life, functional and cognitive status, number of drugs prescribed, or mortality) and the CGA tools of the different studies reviewed (diagnostic or for care planning tools such as the interRAI suite of instruments or for screening such as some novel rapid CGA-based tools). Heterogeneity also exists in the study types included in the present review (RCTs, observational clinical studies, and systematic reviews/meta-analyses). Nevertheless, the present data may represent a brick in the construction of the building demonstrating the usefulness of CGA also in the LTCF setting.
Furthermore, CGA must be standardized across healthcare settings to promote greater health system integration and coordination in the LTCF setting. InterRAI instruments provide such functionality, which not only supports more efficient and comprehensive care planning but also leads to multiple useful derivative applications for clinicians, health administrators, and policy-makers, such as screeners, risk stratification algorithms, outcome scales, QIs, and case-mixed indices. In the LTCF setting, particularly in nursing homes, other new and promising CGA programs have also been proposed. In the future, these rapid screening CGA-based tools could enhance the ability of primary care physicians to recognize and treat geriatric syndromes also in this setting. However, at present, the interRAI RAI suite of instruments appeared to be an integrated health information system with the potential to provide person-centered information transcending healthcare settings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.