
Abstract
Health behaviors and risk factors are independently related with cognitive function in older adults. This study aimed at examining the prevalence and relationship between cognitive function and a number of ideal cardiovascular health (CVH) metrics in older adults from the 2009 to 2010 Chilean National Health Survey. Data from 460 older adults (mean age 73.5 years old, 59.3% women) from the 2009 to 2010 Chilean Health Survey were analyzed. Ideal CVH was defined as meeting the ideal levels of the following components: four behaviors (smoking, body mass index, physical activity, and diet adherence) and three factors (total cholesterol, blood pressure, and fasting glucose). Older adults were grouped into three categories according to their number of ideal CVH metrics: ideal (5–7 metrics), intermediate (3–4 metrics), and poor (0–2 metrics). Cognitive function was assessed by using the modified Mini-Mental Status Examination (mMMSE). Of the 460 participants, 2% had 0 ideal metrics, 11.3% had 1, 23.9% had 2, 32.2% had 3, 20.7% had 4, 9.6% had 5, 0.4% had 6, and 0% had 7. Cognitive function was greater in older adults who met the ideal smoking, physical activity, and fasting blood glucose criteria. Logistic regression analysis suggested that ideal physical activity (Odds Ratio [OR] = 0.411 95% confidence interval [95% CI], 0.209–0.807) and smoking (OR = 0.429 95% CI, 0.095–0.941) behaviors reduced the likelihood of cognitive impairment. Moreover, compared with a poor profile (0–2 metrics), an intermediate (3–4 metrics) (OR = 0.221 95% CI, 0.024–0.911) and ideal CVH profile (5–7 metrics) (OR = 0.106 95% CI, 0.013–0.864) reduced the likelihood of cognitive impairment. We found that intermediate and ideal profiles were associated with a similarly low prevalence of cognitive impairment in Chilean older adults.
Introduction
C
Although evidence of the beneficial effects of physical activity on cognitive function has been clearly provided in the results of animal, epidemiological, and cross-sectional studies, the results and conclusions of randomized controlled trials have been less consistent. 9 Further, reducing the risk of several major noncommunicable diseases such as Alzheimer's, dementia and Parkinson's disease may significantly contribute to a reduction in cognitive decline and the development of brain disorders. 10 For example, in terms of brain function, inactivity and poor dietary habits can disrupt cognition, as studies have reported deficits in learning, memory, and executive functioning in obese compared with healthy individuals. 11 Other studies of young and middle-aged healthy adults have confirmed the association of obesity with behavioral decline in executive function. 12,13
In response to the increasing burden of noncommunicable diseases, the American Heart Association (AHA) established the 2020 Strategic Impact Goals to define the concept of ideal cardiovascular health (CVH) and the metrics needed to monitor it across populations. 14 The seven metrics for ideal CVH in adults (age ≥20 years) comprise four health behaviors (current smoking, body mass index [BMI], physical activity, and healthy diet score) and three health physiological health factors (total cholesterol, BP, and fasting plasma glucose levels).
Nevertheless, it is not clear whether the relationship between cognitive functioning and the cardiovascular disease process is a consequence of shared established risk factors (e.g., obesity, dyslipidemia, physical inactivity, and dysglycemia), and there is a need to better understand how to prevent cognitive impairment; this need has increased as the population ages and the Latin American demographic profile shifts. 15
Given the negative association between cognitive function and mortality, 16 identifying the correlates of cognitive function among older adults is critical. To our knowledge, only one study has analyzed the relationship between ideal CVH and cognition function, assessing older American adults in the Northern Manhattan Study and showing that ideal CVH metrics benefit brain health and cognitive aging. 17 Other studies in young adults and adults show similar results. 18 –20 Poor diet, obesity, and physical inactivity have been shown to be the leading cardiovascular disease risk factors in Chilean adults, raising concerns about whether an increased risk of these conditions also affects cognitive function. 21,22 In addition, the prevalence of ideal CVH has not been examined in an older adult population in Chile.
Therefore, to address these issues, we analyzed data from the 2009 to 2010 Chilean National Health Survey to examine the prevalence of ideal CVH and its relationship with cognitive function in older adults. It was hypothesized that higher scores on seven metrics for ideal CVH, indicating better CVH, are associated with lower prevalence of cognitive impairment in Chilean older adults.
Methods
Study population
The 2009–10 Chilean National Health Survey was a representative household survey with a stratified multistage probability sample of 5,416 noninstitutionalized participants older than 14 years from the 15 regions in Chile, both urban and rural. The sample size was calculated with a 20% relative sampling error to estimate a national representation higher than 4%. One participant was randomly selected per household, and pregnant women were excluded. The response rate was 85%, with no replacements. Detailed information about the survey has been described elsewhere. 23 In this study, 1,013 older adults (>65 years) were evaluated. Of these respondents, 460 had recorded values for all ideal CVH metrics. The study protocol and ethical consent forms were approved by the ethics committee of the Pontificia Universidad Católica de Chile and the Ministry of Health.
Measurements
Standardized protocols were used, and all investigators (nurses and research technicians) underwent joint training sessions before implementation of the survey.
Cognitive function
The modified Mini-Mental State Examination (mMMSE) instrument, which assesses orientation, attention, recent memory, and language, was administered. 24 The mMMSE comprises six questions with a maximum total score of 19 points. Respondents with scores 13 or less were considered cognitively impaired. 25
Ideal CVH
The AHA guidelines 14 were used to construct an ideal CVH index based on the seven metrics by using the cut-off points for adults, with the participants receiving one point for the presence of each ideal metric. The ideal behaviors defined by the AHA were as follows: BMI <25 kg/m2, ≥600 metabolic-equivalent per week, nonsmoking status (either never having smoked or having quit smoking >12 months ago), and consumption of a dietary pattern that promotes ideal CVH. 14 The factors were classified as an untreated systolic BP <120 mmHg and diastolic BP <80 mmHg, untreated total cholesterol ≤200 mg/dL, and untreated fasting blood glucose <100 mg/dL.
Finally, the participants were categorized into one of three health levels based on the number of CVH metrics in the ideal range that they exhibited: The healthiest level (favorable ideal CVH score) was defined as having between 5 and 7 metrics in the ideal range; the intermediate level, 3 to 4 metrics; and the unfavorable level, 0 to 2 metrics. These cut-off points have been used in prior international studies. 26,27
Anthropometrics assessment
Height was measured to the nearest 0.1 cm by using a portable stadiometer, and weight was measured to the nearest 0.1 kg by using a digital scale (Tanita HD-313®) with participants without shoes and in light clothing in their home. Waist circumference was measured at the mid-axillary line at the midpoint between the costal margin and the iliac crest. BMI was calculated as [weight/height 2 ] and was classified by using the World Health Organization (WHO) criteria (normal: 18.5–24.9 kg/m2; overweight: 25.0–29.9 kg/m2; and obese: ≥30 kg/m2). 28
Resting BP
Systolic BP and diastolic BP were measured three times within a 5-minute interval by using a validated HEM-742® sphygmomanometer (Bannockburn, IL) at the subject's home.
Physical activity
The Global Physical Activity Questionnaire (GPAQ) (version 2) was used to measure physical activity. The physically active category was defined as ≥150 minutes of moderate activity per week or >20 minutes of intense physical activity at least three times a week. 29
Healthy diet score
The frequency of consuming fish, shellfish, or other seafood (≥ 1 servings per week), whole grains (≥ 1 serving/day), fruits (≥ 2 servings per day), vegetables (≥ 3 servings per day), and sodium (<15 g/d) was analyzed by using a healthy diet score (4–5 scores) obtained from a questionnaire designed ad hoc 23 while taking into account the guidelines for the Chilean population. 30 Adults with a healthy diet score of 4 were considered to have an ideal diet. 14
Smoking status
Ideal smoking status was determined as nonsmoker or quit smoking ≥12 months.
Covariates
Socio-demographic data were collected for all participants, including age, sex, education level (primary, secondary, or beyond secondary), alcohol intake as assessed by the Alcohol Use Disorders Identification Test (AUDIT), 31 area of residence (urban or rural), and depression in the past year. Past smokers were those who reported that they had smoked >100 cigarettes in their lifetime but did not currently smoke cigarettes. The AUDIT test identifies dangerous drinking behaviors through a summary score constructed from questions on drinking behavior, including drinking frequency, quantity, and inability to stop drinking. Finally, the Composite International Diagnostic Interview, Short Form (CIDI-SF), was applied to establish a diagnosis of major depressive episode by using the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria. 32
Statistical analysis
Statistical normality was tested by using both statistical (Kolmogorov–Smirnov test) and graphical procedures (normal probability plots). Due to the skewed distribution, the mMMSE score was log-transformed. To facilitate interpretation, data were back-transformed from the log scale for presentation in the results. Since no significant interaction was observed between sexes (i.e., sex and ideal CVH categories), all statistical analyses were performed with both sexes together to increase statistical power. The mean mMMSE scores were calculated for each ideal CVH metric and compared by using one-way ANOVA. Finally, logistic regression models were employed to compare the prevalence of cognitive impairment across individual and number of ideal CVH metrics (poor [0–2 metrics], intermediate [3–4 metrics], and ideal [5–7 metrics]). All models were adjusted for age, sex, educational level, area of residence, depression, and alcohol use. Also, each ideal CVH metric was adjusted by the variables mentioned earlier and the rest of ideal CVH metrics. Data were analyzed by using SPSS-IBM (Software; v.22.0 SPSS, Inc., Chicago, IL), and a value of p < 0.05 was considered statistically significant.
Results
Descriptive characteristics and the prevalence of ideal CVH metrics stratified by sex are presented in Table 1. The cohort comprised 460 older adults (mean age 73.5 years old), and 59.3% were women. The prevalence of ideal healthy physical activity and total cholesterol level were higher in men than in women (p < 0.05). Prevalence of cognitive impairment was 15.1% without differences by sex. Overall, none of the older adults met all seven ideal CVH metrics, and nine (2%) did not meet any ideal metric.
CIDI-SF, composite international diagnostic interview, short form; mMMSE, modified mini-mental status examination.
Figure 1 describes the mMMSE scores in Chilean older adults for the individual ideal and nonideal CVH behaviors and factors. Cognitive function (mMMSE score) was lower in older adults who did not meet the smoking (p < 0.001), physical activity (p < 0.05), or nonideal fasting blood glucose (p < 0.05) factors than in participants who did meet the ideal criteria for these behaviors and factors.
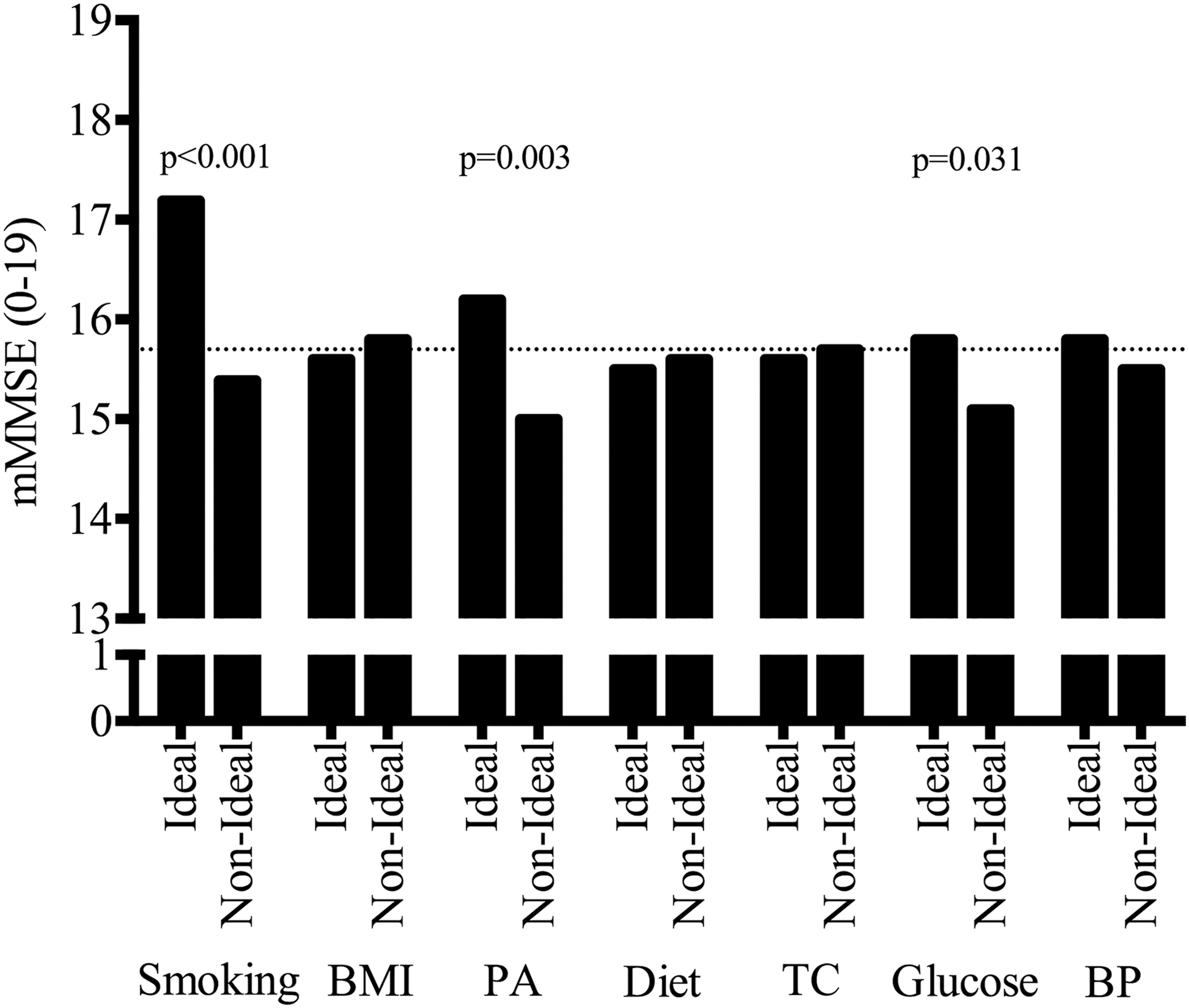
Mean differences of cognitive function according to ideal cardiovascular health metrics in Chilean older adults. BMI, body mass index; BP, blood pressure; PA, physical activity; TC, total cholesterol.
Table 2 shows the odds ratios (ORs) for the prevalence of cognitive impairment for each CVH metric and number of ideal CVH metrics. The adjusted analysis suggested that older adults with ideal levels of physical activity were less likely to have cognitive impairment (OR = 0.411 95% confidence interval [95% CI], 0.209–0.807, p = 0.010) than participants with nonideal physical activity levels. In addition, older adults with ideal smoking behavior were less likely to have cognitive impairment (OR = 0.429 95% CI, 0.095–0.941, p = 0.022) than participants with nonideal smoking habits. Regarding the number of ideal CVH metrics met, the ideal (5–7 metrics) (OR = 0.106 95% CI, 0.013–0.864, p = 0.006) and intermediate profiles (3–4) (OR = 0.221 95% CI, 0.024–0.911, p = 0.008) than the poor profile (0–2 metrics) were associated with a lower likelihood of cognitive impairment.
Each health metric was adjusted by the variables mentioned earlier and the rest of the health metrics.
Analysis adjusted by age, sex, educational level, area of residence, depression, and alcohol use.
Discussion
A unique finding of this study was the greater prevalence of ideal healthy physical activity and total cholesterol levels in men than in women from the 2009 to 2010 Chilean National Health Survey. None of the older adults met all Life's Simple 7. Cognitive function was greater in older adults with ideal smoking, physical activity, and fasting blood glucose variables. Logistic regression analysis suggested that ideal physical activity and ideal smoking behaviors reduced the likelihood of having cognitive impairment. Moreover, compared with a poor profile (0–2 metrics), an intermediate (3–4 metrics) and ideal CVH profile (5–7 metrics) reduced the likelihood of cognitive impairment, independent of age, sex, educational level, area of residence, depression, and alcohol use. However, due to design of the study, the findings should be interpreted with caution.
To our knowledge, this is the first study to report the prevalence of ideal CVH and its components among Chilean older adults. Of the 460 older adults, none met the 7 ideal CVH metrics and 9 (2%) did not meet any of the ideal metrics. Similar results have previously been described in older adults, 17 including in studies conducted in another Latin American country. 33 A healthy diet was the most difficult to achieve in this study, and only 2.4% of the participants met the criteria for an ideal healthy diet. This finding is consistent with other Latin American studies in Brazilian adults (3.2%) 33 and with another study on older adults (<1%). 17 Moreover, older men showed a greater prevalence of ideal physical activity and total cholesterol levels than women. These results may help guide efforts, in both clinical practice and public health, to promote better ideal CVH among Chilean older adults.
Although the cognitive function of older adults with ideal and nonideal BMI, diet, total cholesterol, and BP was similar, a novel finding of this study was the greater cognitive function (mMMSE score) in older adults with ideal smoking and physical activity behavior and with ideal fasting blood glucose levels. In line with these results, a previous meta-analysis showed that elderly smokers had an increased risk of dementia and cognitive decline. 34 Similarly, scientific evidence has suggested that participants with altered glucose metabolism have greater cognitive dysfunction. 35 Regarding physical activity (the parameter most strongly related to cognition function), several studies 36,37 have shown that physical activity might prevent cognitive decline and neurodegenerative diseases in older adults, even when accounting for potential confounders such as age, sex, educational level, alcohol consumption, smoking status, depression score, and cardiovascular disease. 38
Supporting evidence exists for the relationship between individual ideal CVH components and cognition. In our study, when the prevalence of cognitive impairment was assessed according to mMMSE (≤13), the adjusted logistic regression analysis suggested that older adults with ideal smoking and physical activity behavior were less likely to experience cognitive impairment than participants with nonideal levels. Researchers have proposed different hypotheses that suggest that physical activity may indirectly improve cognition by improving health conditions (for example, sleep) and, therefore, reducing the chronic diseases that affect neurocognitive function 39 or by increasing brain perfusion. 40 These effects seems to depend on the type of physical activity performed, although both aerobic 39 and resistance training 41,42 have been found to induce positive effects, either isolated or in combination (i.e., concurrent training). 43
As with ideal physical activity levels, older adults with an ideal smoking habit were less likely to have cognitive impairment than participants with nonideal smoking habits. Although both ideal physical activity and smoking seem to protect cognition in Chilean older adults and although both are associated with a similar mortality risk, 44 the volume of total smokers (n = 394) seems greater than the volume of physically inactive participants (n = 230). Although the results add to a growing body of literature that demonstrates the effects of smoking and physical activity on cognitive health, these novel findings for the Chilean population may help government bodies develop effective and efficient strategies for promoting ideal CVH among older adults.
The analysis of combined ideal CVH metrics showed that an ideal (i.e., 5–7 metrics) and intermediate CVH profile (i.e., 3–4 metrics) reduced the likelihood of cognitive impairment compared with a poor profile (i.e., 0–2 metrics). These results extend and refine the findings of the Coronary Artery Risk Development in Young Adults (CARDIA) study 18 and the Maine-Syracuse Longitudinal Study 19 in young adults (18–30 years old) and adults, which showed that a higher number of ideal metrics was associated with greater cognitive performance. The Reasons for Geographic And Racial Differences in Stroke (REGARDS) study, a prospective study in a cohort younger than ours that included 17,761 participants (>45 years), showed that people with intermediate and high levels of ideal CVH had a similar prevalence of cognitive impairment. 20
Similar to our study, the REGARDS study showed that even an intermediate profile (i.e., 3–4 ideal metrics) may be associated with cognitive benefits. 20 Another previous study, 17 the Northern Manhattan Study of 1,033 older adults also reported that a combined number of ideal CVH factors was associated with improved cognition in a multiethnic older adult population that was mainly composed of Hispanic individuals. Of note, a large number of Chilean older adults had <3 ideal CVH metrics (37.2%), especially in women (42.1 vs 29.9% in men and women, respectively), and thus exhibited a poor CVH profile. In addition, Chile has experienced an 85% increase in people >60 years old in recent decades, and this pattern is expected to continue (INE 1995).
The increased number of older adults and the low prevalence of ideal CVH metrics may pose an enormous burden on the Chilean health system; therefore, multidisciplinary intervention approaches may help improve the rates of combined ideal CVH metrics in older adults and, hence, their cognitive function.
The important strengths of our study include the population-based sampling method and the extensive data on potential confounders.
However, this study has some limitations. First, the cross-sectional design did not allow for cause–effect inferences between cognition function and ideal CVH metrics to be made, and we were unable to determine whether ideal CVH was associated with delays in aging-related cognitive decline in the long term. Second, although the MMSE questionnaire is the most widely used test for determining an individual's cognitive health, it is considered to have an insufficient scope to identify mild forms of cognitive decline. 45 Third, the physical activity questionnaires utilized in our article often fail to provide sufficient detail on activity type, frequency, duration, and intensity, especially in older adults. 46 Finally, another limitation was the lack of a caloric measure of total energy, fat, and sugar intake, which could not be obtained from the questionnaire used.
Conclusion
In summary, none of the older adults met all seven ideal CVH metrics and 37.2% of this population had three or less ideal metrics. We observed that the intermediate and ideal profiles were associated with a similarly low prevalence of cognitive impairment, highlighting the importance of early life health behaviors and health factors in Chilean older adults. Although cross-sectional, this study could provide valuable information regarding the importance of public health initiatives that aim at better controlling these seven metrics and improving CVH profiles from poor to intermediate or higher, which could lead to reductions in cognitive decline.
Footnotes
Acknowledgments
The authors thank all participants for their co-operation and the Chilean Health Ministry and Department of Public Health, The Pontificia Universidad Católica de Chile for designing and conducting the second National Health Survey, 2009–2010. AGH was funded by Proyectos Basales (Proyectos Basal USA 1555 - Vridei 021787GH_MOV) y Vicerrectoría de Investigación, Desarrollo e Innovación (Universidad de Santiago de Chile, USACH).
Author Disclosure Statement
No competing financial interests exist.