
Abstract
Atherosclerotic cardiovascular disease, including peripheral artery disease (PAD), is more common and severe in diabetic patients compared with nondiabetic individuals. Indeed, diabetes is associated with the increased risk of limb amputation and all-cause mortality in patients with symptomatic PAD. Proteins and lipids are nonenzymatically modified by sugars, resulting in the formation and accumulation of advanced glycation end products (AGEs), whose process is accelerated under diabetic conditions, especially patients with a long duration of diabetes. Accumulating evidence shows that nonenzymatic modification by sugars alters the structural integrity of collagens and lipoproteins in large vessels, thereby being involved in vascular stiffness and atherosclerotic plaque instability. Furthermore, engagement of receptor for AGEs (RAGE) with its ligands, such as AGEs, high mobility group box 1, and S100A proteins evokes inflammatory and thrombotic reactions, thus playing a central role in the development and progression of atherosclerotic cardiovascular disease. In this article, we review the pathophysiological role of RAGE ligands in PAD and discuss the clinical utility of measurement of plasma, serum, or tissue RAGE ligands for assessment of the severity and prognosis of PAD. This review suggests that RAGE ligands may be a novel biomarker and also a therapeutic target of PAD, especially in patients with diabetes.
Introduction
P
Nonenzymatic glycation of amino groups of proteins, lipids, and nucleic acids progresses under diabetes, resulting in the formation and accumulation of advanced glycation end products (AGEs), the extent of which is increased in parallel with cumulative hyperglycemic exposure. 10 –12 AGEs have been shown to contribute to the development and progression of atherosclerotic cardiovascular diseases through several mechanisms; (1) nonenzymatic cross-linked modification of collagen by sugars alters its structural integrity and physiological function, (2) glycation of apolipoprotein B makes low-density lipoprotein more atherogenic, and (3) engagement of receptor for AGEs (RAGE) with its ligands stimulates oxidative stress generation and subsequently evokes inflammatory and thrombogenic reactions in vascular wall cells, platelets, and macrophages, all of which could play a role in vascular stiffness, endothelial dysfunction, and atherosclerotic plaque instability in high-risk patients for cardiovascular disease, especially elderly subjects with diabetes. 13 –18
Therefore, we review in this study the pathophysiological role of RAGE ligands, such as AGEs, high mobility group box 1 (HMGB1), and S100A proteins in PAD, and further discuss the clinical utility of measuring these RAGE ligands in plasma, serum, skin, or vascular tissues for assessment of the severity and prognosis of PAD. In this article, literature searches were undertaken in Medline by the PubMed interface. Non-English language articles were excluded. Key words [(glycation or RAGE or HMGB1 or S100) and (PAD or arteriosclerosis obliterans or limb ischemia)] have been used to select the articles.
Pathophysiological Role of RAGE Ligands in Limb Ischemia: Lessons from Animal Studies
Advanced glycation end products
In streptozotocin-induced diabetic mice, platelet-derived growth factor-B (PDGF-B) gene expression was reduced in the tight muscles at baseline and after surgically induced limb ischemia, whereas supplementation of PDGF-B gene or inhibition of protein kinase C-α (PKC-α) significantly increased the blood flow in ischemic limb and completely prevented the autoamputation, which was associated with restoration of PDGF-B expression. 19 Furthermore, aminoguanidine, an inhibitor of AGE formation, inhibited the phosphorylation of PKC-α and restored the reduced PDGF-B levels in ischemic tight muscles. These observations suggest that AGEs may contribute to the reduced tolerance against surgically induced limb ischemia through the suppression of PDGF-B expression using PKC-α activation.
Suppression of mitochondrial reactive oxygen species (ROS) generation by a lipid-soluble thiamine derivative benfotiamine has been shown to prevent high glucose-induced formation of AGEs and activation of PKC, NF-κB, and sorbitol pathway. 20,21 Benfotiamine also inhibited the AGE accumulation and restored the activity of protein kinase B/Akt (PKB/Akt) and blood flow in ischemic limb, leading to the prevention of ischemia-induced toe necrosis in type 1 diabetic mice, which were associated with improvement of reparative angiogenesis. 22 These protective effects of benfotiamine on limb ischemia were inhibited by intramuscular overexpression of dominant-negative PKB/Akt. In addition, benfotiamine stimulated the proliferation of endothelial progenitor cells (EPCs) in vitro and restored the reduced number of circulating EPCs in diabetic mice. 22 AGE-RAGE interaction not only induced apoptotic cell death but also suppressed migration and tube formation of EPCs by inhibiting the Akt. 23 AGEs also impaired the migration of EPCs through shedding of cell surface syndecan 4, while homing of EPCs to the site of ischemic limb was impaired in syndecan 4-deficient mice, and syndecan 4 expression on EPCs was decreased in type 2 diabetic patients. 24 Moreover, circulating AGE levels were independently correlated with decreased cell number and impaired migratory activity of EPCs in apparently healthy subjects. 25 These findings suggest the pathological role of AGEs in impaired reparative angiogenesis in ischemic limb.
Expression of AGEs and RAGE was increased in ischemic limb of streptozotocin-induced diabetic mice. 26,27 Decreased blood flow, impaired angiogenesis, and reduced macrophage infiltration in the ischemic limb were significantly ameliorated in RAGE-deficient or glyoxalase-1 transgenic diabetic mice. 26,27 Therefore, activation of the AGE-RAGE axis may be involved in attenuated adaptive inflammatory and angiogenic reactions to limb ischemia in diabetes. Since HMGB1, another RAGE ligand, was significantly increased in ischemic limb compared with nonischemic leg in both wild-type and RAGE-deficient mice, 27 HMGB1-RAGE axis may also contribute to impaired collateral vessel formation after surgically induced limb ischemia. It would be interesting to further examine the role of this elevation of HMGB1 in reparative angiogenesis in RAGE-deficient mice because HMGB1 is able to bind to toll-like receptors 2 and 4 (TLR2 and 4) and work as a cytokine. 18
Neutralizing antibody raised against RAGE improved limb ischemia by ameliorating reparative angiogenesis in type 1 diabetic mice, which was associated with reduction of RAGE levels in the ischemic limb. 28 We have previously reported that AGEs induce RAGE expression through ROS production in various types of cells, which in turn stimulates the generation of AGEs. 29 Therefore, the blockade of positive feedback loop between RAGE ligands and RAGE may be a promising therapeutic strategy for limb ischemia in diabetes. RAGE-directed molecular imaging was developed to evaluate the effect of diabetes on RAGE expression and angiogenesis in a murine model of limb ischemia. 30
High mobility group box 1
HMGB1 was released from ischemic skeletal muscles after femoral artery ligation in mice, whereas intramuscular administration of HMGB1 improved the limb perfusion, which was associated with enhanced angiogenesis. 31 TLR2 and 4 were upregulated in ischemic skeletal muscles of mice, and TLR4 mediated the inflammatory reactions, such as TLR4 and interleukin-6 overexpression in ischemic limbs. 32 Deletion of TLR4 gene augmented the blood flow recovery after limb ischemia, but not in the absence of TLR2 gene. 32,33 Furthermore, collateral vessel maturation after limb ischemia was impaired in TLR2 knockout mice. 34 These observations suggest that TLR2, in the absence of TLR4, could improve limb ischemia. Chloroquine increased skeletal muscle and serum HMGB1 levels and ameliorated the blood perfusion after ischemia in mice. 35 Recovery of perfusion was impaired in ischemic limb of anti-HMGB1 antibody-treated mice or HMGB1-deficient mice. 33,35 Therefore, HMGB1 may play a protective role against limb ischemia in nondiabetic mice, which is mainly mediated through the interaction with TLR2. In addition, HMGB1 also enhanced the recovery of blood flow after limb ischemia in diabetic mice using a vascular endothelial growth factor (VEGF)-dependent manner. 36 However, in a rat model of limb ischemia perfusion, blockade of HMGB1 improved the blood perfusion of ischemic limb by suppressing the inflammatory reactions. 37
S100A1
S100A1, an EF-hand calcium binding protein, is one of the RAGE ligands. 38 S100A1 expression levels were decreased in ischemic skeletal muscles of patients with PAD and mice with critical limb ischemia. 39 In S100A1 knockout mice, recovery of blood perfusion and reparative angiogenesis in ischemic limbs were impaired in association with the high rates of autoamputation. 39 In the ischemic limbs of S100A1-deficient mice, endothelial nitric oxide synthase activity was decreased, whereas VEGF receptor 2-phosphoinositide 3 kinase-Akt signaling pathway was compromised, which was associated with augmented expression of hypoxia-inducible factor 1α and VEGF. These findings suggest that S100A1 may play a protective role against limb ischemia partly through modulation of endothelial nitric oxide synthase function. It would be interesting to clarify the role of other RAGE ligands than S100A1 in postischemic angiogenesis of S100A1-deficient mice.
RAGE Ligands as a Biomarker of PAD: Lessons from Clinical Studies
Circulating levels of AGEs
In 99 consecutive type 2 diabetic patients, although serum levels of AGEs and pentosidine were inversely associated with ankle-brachial index (ABI), pentosidine but not AGE levels were significantly higher in diabetic patients with PAD than those without. 40 The study showed that pentosidine was strongly correlated with PAD in type 2 diabetic patients. 40 Serum levels of pentosidine were independently correlated with reduced ABI values in apparently healthy men as well. 41 In 40 patients with symptomatic PAD, plasma levels of pentosidine and carboxymethyllysine (CML) were independently associated with the presence of critical limb ischemia defined as rest pain and minor or major tissue loss. 42 Pentosidine and CML were also correlated with Rutherford stage, a grading system for describing PAD. 42,43 These observations suggest that circulating levels of pentosidine and CML may be a biomarker that could reflect the severity of PAD. Hemoglobin glycation index (HGI) defined as the measured HbA1c minus predicted HbA1c was associated with prevalence of PAD in drug-native prediabetic or diabetic patients after adjustment for other cardiovascular risk factors. 44 Since high HGI might reflect higher protein glycation and more accumulation of AGEs, correlation between HGI and PAD could be partly explained by the deleterious vascular effects of AGEs. Now the ARTERY study is ongoing to evaluate the role of amount, type, and location of AGEs on PAD in patients with or without diabetes. 45
Tissue accumulation levels of AGEs
Long-term follow-up studies of Diabetes Control and Complications Trial (DCCT) and United Kingdom Prospective Diabetes Study have shown that cumulative hyperglycemic exposure in the past is one of the markers that could predict future cardiovascular events and death in both type 1 and type 2 diabetic patients. 12 Skin collagen AGEs at the end of DCCT have been correlated with the risk of future 10–12-year progression of retinopathy, nephropathy, and carotid intima media thickness in type 1 diabetic patients, which was totally independent on mean HbA1c values. 46,47 These clinical studies have suggested that long-term accumulation of AGEs could partly explain the phenomenon of metabolic memory in vascular complications of diabetes. 12
There is accumulating evidence that skin autofluorescence (SAF) measured by the desktop device (DiagnOptics Technologies, Groningen, The Netherlands) could reflect tissue accumulation levels of both fluorescent and nonfluorescent AGEs in humans, being a novel biomarker that predicts future cardiovascular events in high-risk patients. 48,49
A case–control study (492 patients with PAD and 164 age- and presence of diabetes mellitus-matched controls) revealed that SAF was significantly higher in PAD patients than controls, especially in PAD patients with cardiovascular comorbidity. 50 For each one arbitrary unit increase in SAF, the risk of presence of PAD increased to 2.34-fold, and the significant correlation of SAF with PAD was unaffected after adjustment for traditional coronary risk factors and a history of cardiovascular diseases. 50 Age, smoking, diabetes mellitus, chronic kidney disease, and a history of cerebrovascular disease or abdominal aortic aneurysm (AAA) were independent correlates of SAF in patients with PAD. 50
A cross-sectional study of 96 controls, 67 patients with subclinical atherosclerosis, and 60 patients with PAD showed that SAF in patients with subclinical atherosclerosis or PAD was significantly higher compared with controls, and SAF was also significantly higher in PAD patients compared with subjects with subclinical atherosclerosis. 51 The difference of SAF among three groups was independent of diabetes mellitus, renal function, and Framingham risk score. 51 Patients with carotid artery stenosis and PAD had a significantly higher SAF than those with carotid artery stenosis only, and the presence of PAD was one of the independent determinants of SAF in patients with carotid artery stenosis as well. 52 As the case with carotid artery stenosis, a case–control study of 248 patients with AAA and 124 age-matched controls showed that PAD comorbidity was associated with high SAF values within the AAA patients, and PAD was one of the independent correlates of SAF. 53 SAF was also independently correlated with the presence of PAD in patients with diabetic foot ulcer. 54
In a 5-year follow-up study of 252 PAD patients, SAF has been shown to be an independent marker that predicts amputation due to critical limb ischemia. 55 After adjustment for diabetes mellitus and Fontaine stage, the hazard ratio for amputation per arbitrary unit increase of SAF was 2.72 (p = 0.004); SAF was the only determinant factor that predicted the amputation in PAD patients with Fontaine stage 1 and 2. 55 Multiplication of Fontaine stage by SAF improved the risk prediction for future amputation in patients with PAD. 55 In the same prospective cohort study, SAF was associated with 5-year mortality and fetal and nonfetal major cardiovascular events defined as cardiovascular death, myocardial infarction, and stroke in patients with PAD; hazard ratios per arbitrary unit increase of SAF for mortality and major cardiovascular events were 2.01 and 1.82, respectively, whose values remained significant after adjustment for cardiovascular risk factors and use of lipid-lowering drugs. 56,57
A longitudinal cohort study of 471 PAD patients showed that although baseline SAF was associated with lower estimated glomerular filtration ratio, it did not predict the decline in renal function during a median follow-up of 3 years. 58
High mobility group box 1
HMGB1 is a nonhistone nuclear protein, which is passively released or actively secreted from necrotic cells or inflammatory cells, respectively, and acts as a danger signal to contribute to tissue repair and inflammatory reactions using RAGE, TLR2, or TLR4. 18 HMGB1 expression was significantly increased in the ischemic skeletal muscles of patients with claudication or critical limb ischemia compared with control patients. 35 HMGB1 levels in the vessels of amputated foot were significantly higher in diabetic patients with PAD than those of nondiabetic controls, which were positively correlated with artery stenosis grade, oxidative stress, and inflammatory markers. 59 Plasma concentrations of HMGB1 were significantly higher in 24 patients with PAD than those of 10 age-, sex-, and body weight-matched controls, and plasma fibrinogen was the sole correlate of HMGB1 in PAD patients. 60 As described above, it remains unclear whether HMGB1 is a friend or foe of limb ischemia and collateral vessel formation in patients with PAD. However, circulating levels of HMGB1 may be a biomarker of PAD.
S100 proteins
A 12-year prospective cohort study of 146 diabetic patients without PAD showed that baseline plasma levels of S100A12 and RAGE score defined by averaging Z-standardized values of S100A12, CML, and endogenous secreted form of RAGE were significantly associated with amputation or death; age- and sex-adjusted hazard ratio for amputation or death was 1.29 per 100 ng/mL increase in S100A12 and 1.79 per 1 unit increase (standard deviation) in RAGE score. 61 However, the significant association of S100A12 and RAGE score with amputation or death was lost after adjustment for Framingham cardiovascular risk score. Similar correlations of S100A12 or RAGE score with development of PAD or death were observed. 61 Furthermore, plasma S100A12 levels were higher in PAD patients than those of controls, especially in diabetic patients with PAD. 62 Compared with PAD patients with S100A12 values below 75% (8.6 ng/mL), patients above the value were associated with reduced amputation-free survival in a 3-year prospective cohort study; the risk of death or amputation in the latter group was thrice that of the former one. 62 These observations suggest that plasma S100A12 could play a role in the development and progression of PAD and predict the prognosis of life-threatening disorder.
Hemodialysis patients with PAD had a significantly higher value of S100A12 compared with hemodialysis subjects without PAD. 63 Plasma S100A12 was the independent determinant of the presence of PAD in hemodialysis patients. 63 Type 2 diabetic patients with low-density carotid plaque more likely had PAD and higher serum levels of S100A8/A9. 64
Soluble RAGE and PAD
Soluble RAGE (sRAGE) consisting of the extracellular ligand-binding domain has been identified in human serum or plasma. 65 There is some controversy about the regulation and role of sRAGE in vascular disease in humans. 65 sRAGE levels were decreased in patients with PAD compared with control subjects. 66 Individuals carrying at least one Ala12 allele of peroxisome proliferator-activated receptor-γ2 had the lower levels of sRAGE, irrespective of the presence or absence of PAD, and the Ala12 allele was independently associated with the presence of PAD. 66 Compared with control subjects, sRAGE levels were significantly lower in patients with coronary artery disease, especially in those with concomitant presence of PAD. 67
PAD and Tobacco, an Exogenous Source of AGEs
Tobacco smoking is one of the major environmental sources of exogenously derived AGEs. 68,69 Indeed, we, along with others, have shown that serum levels of AGEs or SAF are significantly higher in smokers than nonsmokers and that SAF is correlated with pack years of smoking. 69,70 Not only current but also former smokers had the increased risk of PAD, thus suggesting that cumulative smoking exposure could play a role in the pathogenesis of PAD. 71 –73 A population study of 2517 community-dwelling Korean men revealed that the odds ratio of PAD after adjustment for other cardiovascular risk factors was 2.31 for former smokers and 4.30 for current smokers. 72 In a 12-year and 7-month prospective follow-up study of 39,825 women without cardiovascular disease, fully adjusted hazard ratios for PAD for smoking abstinence of fewer than 10, 10 to 29, and 30 or more pack-years were 2.52, 6.75, and 11.09, respectively, indicating a significant dose–response relationship between pack-years of former smoking and PAD incidence. 73 The correlation of smoking with PAD has an analogy to the phenomenon of the metabolic memory in vascular complications of diabetes. 12 Therefore, the deleterious effects of smoking on PAD may be partly ascribed to tobacco-derived AGEs.
Limitations
Although PAD is defined as a narrowing of the peripheral arteries to the legs, stomach, arms, and head, it is most commonly observed in the arteries of the legs, which is the leading cause of leg gangrene and amputation. 1 –4 So, in this study, we focused on the role of RAGE ligands in peripheral leg artery disease.
Conclusions
We propose a scheme to summarize the pathophysiological role of RAGE ligands in PAD (Figs. 1 and 2). The formation and accumulation of AGEs and expression of HMGB1 and S100 proteins are accelerated during a physiological aging process, diabetes, hypoxia, or inflammatory conditions. 13,17,18,32,74 Further clinical studies are needed to investigate whether blockade of RAGE ligands could halt the progression of PAD and improve the survival rate in these patients.
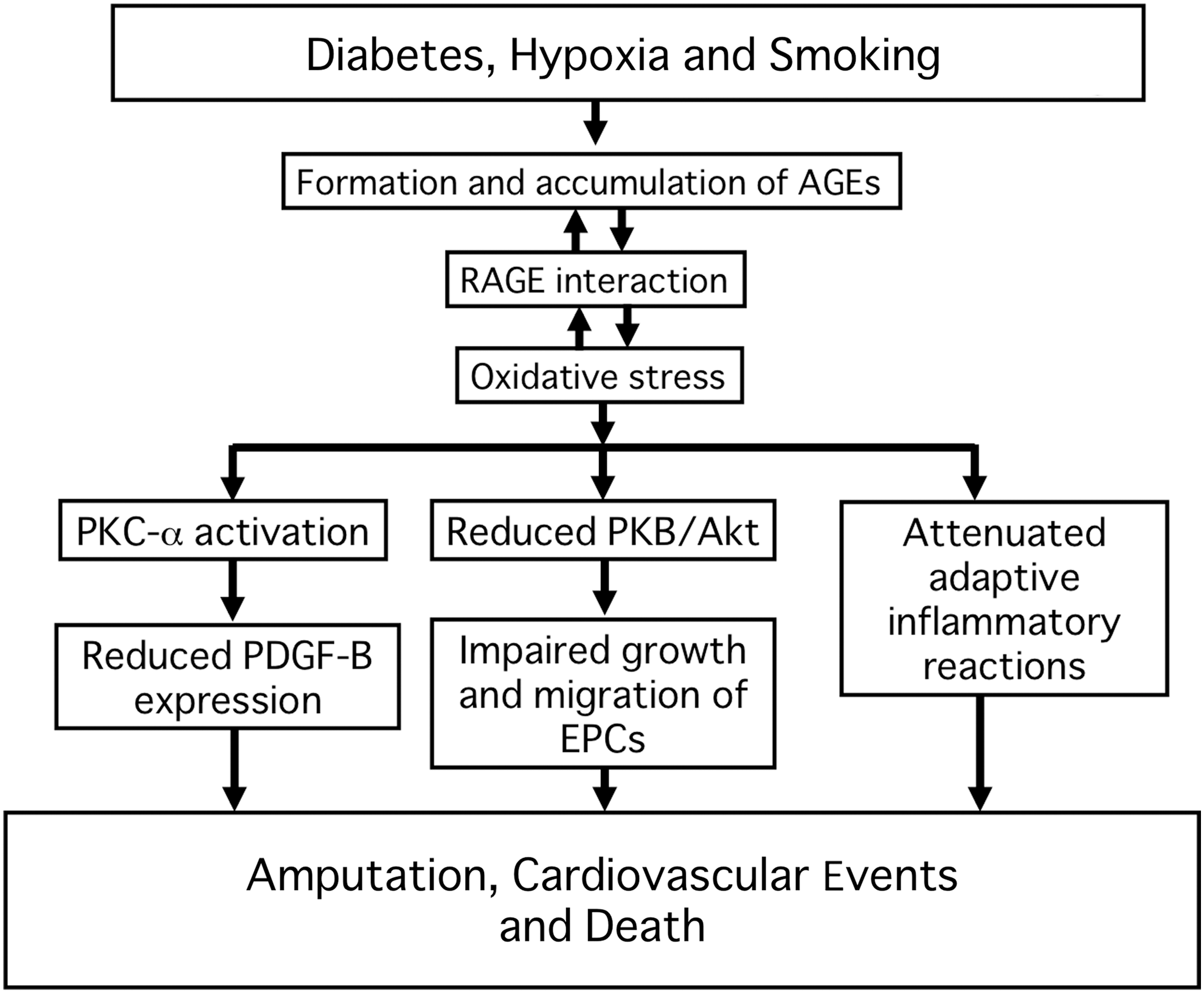
Possible pathological role of AGEs in the development and progression of PAD. AGEs, advanced glycation end products; EPCs, endothelial progenitor cells; PDGF, platelet-derived growth factor; PKB, protein kinase B; PKC-α, protein kinase C-α; RAGE, receptor for AGEs.
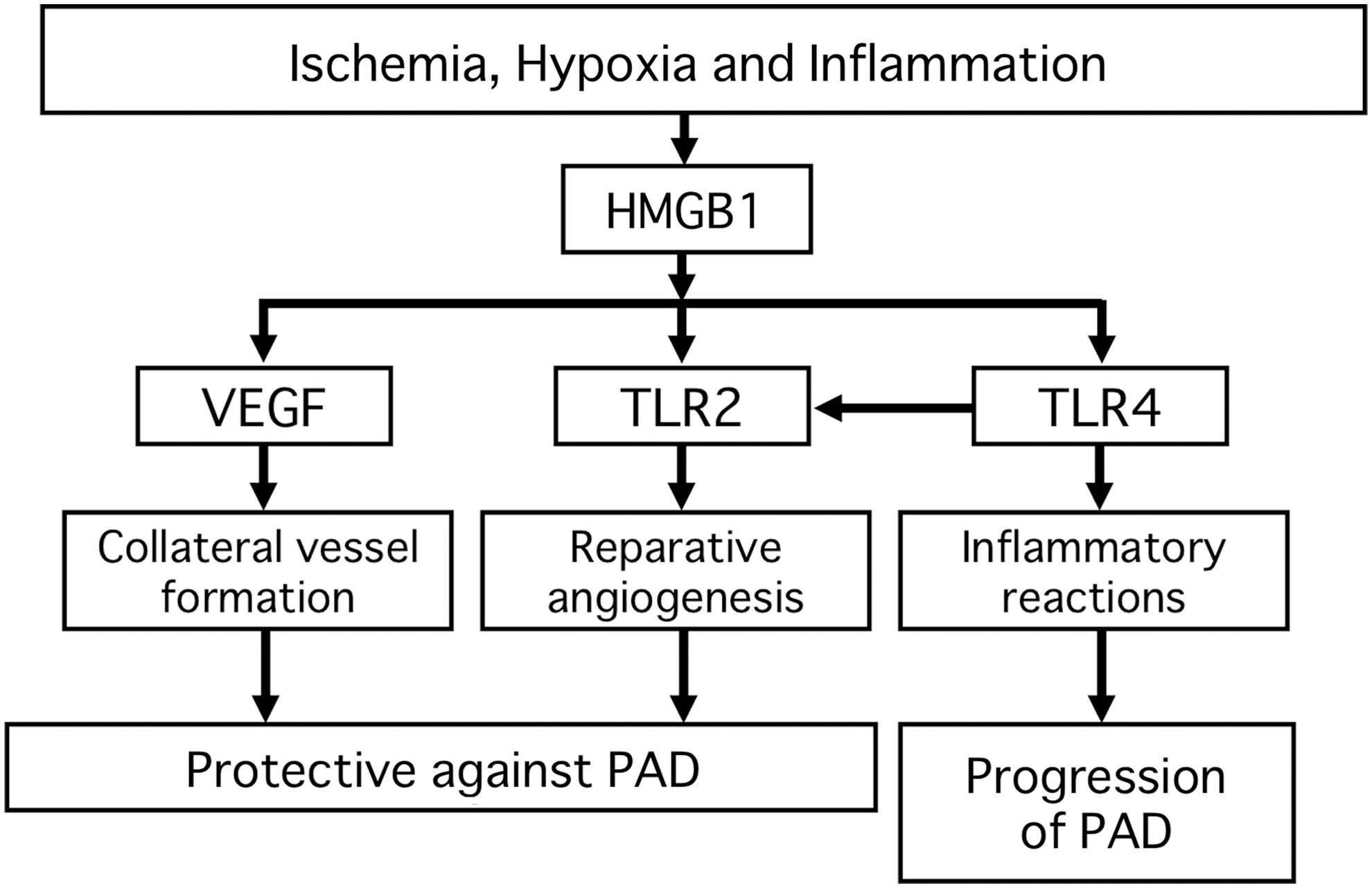
Effects of HMGB1 on PAD. HMGB1, high mobility group box 1; TLR, toll-like receptor; VEGF, vascular endothelial growth factor.
Footnotes
Acknowledgments
This study was supported, in part, by Grants-in-Aid for Scientific Research (Grant Number 17K08968) from the Ministry of Education, Culture, Sports, Science and Technology, Japan (to S.Y.).
Authors' Contributions
S.Y. mainly contributed to the present article, conceptualized and designed the article, drafted the article, and took responsibility for the integrity of the data and the accuracy of the data analysis. T.M. made the critical review for intellectual content. All authors approved the final article.
Author Disclosure Statement
No competing financial interests exist.