
Abstract
The klotho protein is secreted primarily by the kidneys. It is responsible for phosphate homeostasis and has an anti-aging, anti-inflammatory, and anti-oxidative stress role. Obstructive sleep apnea (OSA) is associated with an enhanced systemic inflammation and oxidative stress, but mechanisms that regulate these processes are poorly understood. The aim of the study was to investigate the plasma levels of klotho in OSA. Twenty-one previously untreated patients with OSA (56 ± 13 years, 12 males) and 41 non-OSA control volunteers (48 ± 16 years, 8 males) participated in the study. Medical history has been taken; participants filled out the Epworth Sleepiness Scale. C-reactive protein and renal function, glucose and lipid profile measurements were performed in sera; klotho was determined in citrate-treated plasma samples. Levels of plasma klotho were decreased in OSA (519.1 ± 164.9 pg/mL) versus controls (700.8 ± 431.4 pg/mL, p = 0.02). Reduced klotho concentrations were associated with markers of overnight hypoxemia determined with O2 desaturation index (r = −0.31, p = 0.01), percentage of sleep time spent with saturation <90% (r = −0.41, p < 0.01), and minimal saturation during sleep (r = 0.33, p = 0.01). Interestingly, there was no relationship with apnea-hypopnea index, total sleep time, or arousal index (all p > 0.05). Significant association was also found between low plasma klotho levels and the presence of hypertension (p < 0.05). Our results suggest that chronic intermittent hypoxia reduces the levels of klotho in OSA, which may contribute to the development of hypertension. Decreased klotho levels may play a role in enhanced systemic inflammation in OSA and may be a future target for drug development.
Introduction
Obstructive sleep apnea (OSA) is a common disease that affects more than 10% of the general adult population. 1 It is characterized by recurrent episodes of complete or partial collapse of the upper airways during sleep, subsequent intermittent hypoxia, and disturbance in sleep architecture. Apart from the frequent day and nighttime symptoms, OSA is associated with heightened risk for cardiovascular, metabolic, 2 and cognitive comorbidities. 3
Chronic intermittent hypoxia (CIH) induces the production of reactive oxygen species and the expression of proinflammatory mediators. 4 Accordingly, the levels of markers of oxidative stress and systemic inflammation relate to disease severity 5 and contribute to the development of comorbidities. 6 However, the elements of systemic inflammation, especially immune regulators, 7 are poorly described in OSA.
The klotho protein has been discovered fortuitously in gene-deficient mice, being responsible for an early aging phenotype in association with multiorgan damage and premature death. 8 The klotho family consists of three members (α, β, and γ klotho); for brevity, we refer the α klotho as klotho. Klotho is predominantly synthesized in the distal convoluted tubules of the kidney, but other organs, including parathyroid gland, ovary, testis, and placenta, also express the klotho gene. 9 There is an extensive evidence that klotho plays a crucial role in the aging process. 10
Klotho can be expressed in either membrane-bound or soluble form. 11 The membrane-bound klotho acts as a coreceptor for fibroblast growth factor-23 (FGF-23) receptors, 12 which pathway is responsible for phosphate homeostasis. Thus, the lack of klotho leads to hyperphosphatemia, causing premature aging. 13 Soluble klotho also acts against hyperphosphatemia by inhibiting intestinal and renal phosphate absorption. 11 It suppresses senescence through the blockage of Wnt signaling, 11 regulates aldosterone synthesis, 14 has an anti-inflammatory 11 and anti-oxidative stress effect, 15 and induces the expression of endothelial nitric oxide synthase (eNOS). 16 In line with this, impaired klotho production leads to endothelial dysfunction, and reduced circulating levels were reported in cardiovascular disease. 17
Several lines of evidence suggest altered levels of klotho in OSA. First, systemic inflammation reduces the renal production of klotho. 18,19 Second, the levels of vitamin D, a potential activator of klotho, 20 are decreased in OSA. 21 Third, morbid obesity, the most important etiological factor for sleep apnea, 1 is associated with lower klotho levels. 22 Only one study has investigated klotho in OSA so far. 23 Although the article reported reduced klotho concentration in sleep apnea, the diagnostic tests for OSA were not described, nor were klotho levels correlated with disease severity or variables of sleep characteristics.
In this study, we aimed to analyze plasma klotho levels in OSA. To understand its role, we correlated its levels with sleep architecture, markers of overnight hypoxia, and OSA-related comorbidities.
Methods
Study design and subjects
Sixty-two adult volunteers (20 males, aged 51 ± 15 [mean ± standard deviation] years) who were referred to the Sleep Unit, Department of Pulmonology, Semmelweis University, due to suspected OSA (i.e., snoring, witnessed apnea, daytime sleepiness, fatigue, etc.) participated in the study. We excluded patients with a known malignancy in the last 5 years, history of autoimmune disease, uncontrolled chronic disease (i.e., acute heart failure, poorly controlled diabetes), known moderate-to-severe renal failure, and those with infection within 4 weeks before the study. None of the participants have previously been diagnosed with OSA, nor they received any treatment, including continuous positive airway pressure (CPAP) or oral appliance therapy.
Polysomnography has been performed in 44 participants, and cardiorespiratory polygraphy in 18 cases. Following the diagnostic tests, venous blood was taken into citrate tubes for plasma klotho assessment and for serum glucose, creatinine, cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), triglyceride, and C-reactive protein (CRP) measurements. Glomerular filtration rate (GFR) was estimated using the Modification of Diet in Renal Disease equation:
Medical history was taken, blood pressure was measured, and the participants filled out the Epworth Sleepiness Scale (ESS) questionnaire. The study was approved by the Semmelweis University Ethics Committee (TUKEB 30/2014) and was conducted according to the Declaration of Helsinki. Patients provided written consent to the study.
Plasma klotho measurements
Blood samples were centrifuged at 4°C for 10 minutes at 1500 rpm, and the plasma was stored at −80°C until further analysis. Plasma klotho levels were measured using a commercially available ELISA kit (Immuno-Biological Laboratories Ltd.) as described previously. 24,25
Sleep studies
In-patient polysomnography and cardiorespiratory polygraphy were performed as described previously 26 using Somnoscreen Plus Tele PSG (Somnomedics GMBH, Germany). Briefly, body position, thoracic and abdominal respiratory excursions, breath sounds, nasal pressure, electrocardiogram, and O2 saturation were registered for polygraphy, while polysomnography had additional measures of electroencephalogram, electro-oculogram, and electromyogram.
Sleep stages, movements, and cardiopulmonary events were scored manually according to the American Academy of Sleep Medicine 27 guidelines. Total sleep time (TST), sleep period time (SPT), percentage of TST spent with saturation <90% (TST90%), and minimal O2 saturation (minSatO2) were recorded; apnea-hypopnea index (AHI), O2 desaturation index (ODI), and arousal index (AI) were calculated. OSA was defined as having an AHI ≥5/h.
Statistical analysis
GraphPad Prism 5.0 (GraphPad Software, San Diego, CA) was used for statistical analysis. Normality of the data was assessed with the Shapiro–Wilk test. OSA and control groups were compared with t-test, Mann–Whitney U test, chi-square test, and Fisher's exact test. Plasma klotho levels were compared with clinical characteristics and markers of sleep architecture with the Spearman test. Analyses were performed also after excluding the eight obese (body mass index [BMI] ≥30 kg/m2) participants (n = 5 OSA and n = 3 controls). A p-value <0.05 was considered significant.
The minimal sample size was estimated to analyze the relationship between plasma klotho and markers of overnight hypoxia (i.e., ODI and TST90%) with an effect size of 0.35, power of 0.80, and alpha of 0.05. This was based on plasma klotho level distribution in the control group of our previous study. 24
Results
Comparison of OSA and non-OSA groups
Of the 62 participants, 21 were diagnosed with OSA. Twelve of them had mild (AHI between 5 and 14.9/h), six moderate (AHI between 15 and 29.9/h), and three severe (AHI ≥30/h) disease. Subjects' characteristics are shown in Table 1. The OSA group comprised a higher proportion of males and patients with hypertension and dyslipidemia. Patients with OSA had higher BMI, serum triglyceride levels, AHI, TST90%, and ODI, while minSatO2 was significantly lower (all p < 0.05). Plasma klotho levels were lower in OSA (519.1 ± 164.9 pg/mL) versus controls (700.8 ± 431.4 pg/mL, p = 0.02; Fig. 1).

Plasma klotho concentration among OSA patients versus non-OSA subjects. Individual data and median values are presented. OSA, obstructive sleep apnea.
Patient Characteristics
AHI, apnea-hypopnea index; AI, arousal index; BMI, body mass index; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; ESS, Epworth Sleepiness Scale; GFR, glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; minSatO2, minimal O2 saturation; n.a., not applicable; n.s., nonsignificant; ODI, O2 desaturation index; OSA, obstructive sleep apnea; SPT, sleep period time; TST90%, percentage of total sleep time spent with saturation <90%; SD, standard deviation.
We noticed five outlier data in the control group. These subjects did not differ in general characteristics, medication usage, or comorbidities from other controls. When excluding these participants (i.e., plasma klotho ≥1000 pg/mL), there was only a trend for lower plasma klotho values in OSA (519.1 ± 164.9 vs. 558.3 ± 103.4 pg/mL, p = 0.10). In addition, when analyzing only the nonobese volunteers, klotho levels in OSA (529.1 ± 186.7 pg/mL) tended to be lower than in controls (712.8 ± 446.2 pg/mL, p = 0.08).
Relationship between plasma klotho levels and sleep parameters
Plasma klotho levels significantly correlated with markers of overnight hypoxia, including ODI (r = −0.31, p = 0.01; Fig. 2), TST90% (r = −0.46, p = 0.03), and minSatO2 (r = 0.33, p = 0.01; Fig. 3). Interestingly, there was no correlation with ESS, TST, SPT, AHI, or AI (all p > 0.05). When obese patients were excluded, the relationships between plasma klotho levels and ODI (r = −0.27, p = 0.04), TST90% (r = −0.45, p < 0.01), and minSatO2 (r = 0.33, p = 0.01) were still significant.

Correlation between O2 desaturation index and plasma klotho concentration.
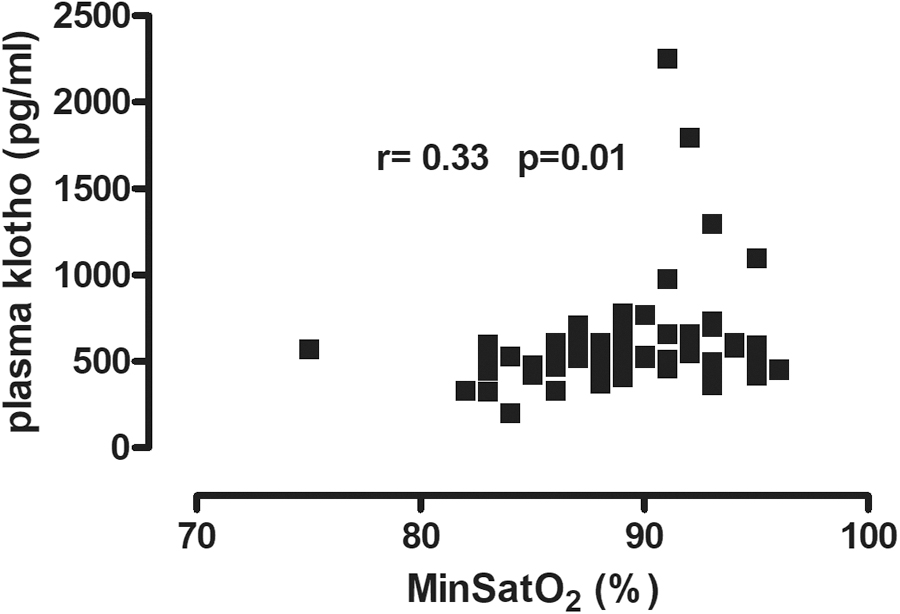
Correlation between minimal O2 saturation and plasma klotho concentration.
When analyzing the patients with OSA separately, only the association between plasma klotho and TST90% remained significant (r = −0.46, p = 0.04). This was also true when only the nonobese participants were analyzed (r = −0.57, p = 0.01).
Relationship between plasma klotho levels and demographics, comorbidities, and laboratory parameters
Analyzing all participants together, patients with hypertension had significantly lower plasma klotho concentration than normotensive subjects (504.7 ± 120.3 vs. 730.2 ± 444.9 pg/mL, p = 0.02). There was a tendency for lower klotho levels in patients with chronic obstructive pulmonary disease (COPD; 439.0 ± 135.3 vs. 656.8 ± 381.6 pg/mL, p = 0.06). There was a significant indirect relationship between plasma klotho and serum triglyceride levels (p = 0.01, r = −0.31). Klotho levels did not correlate with age, BMI, smoking history, CRP, total cholesterol, HDL-C, LDL-C, or glucose levels (all p > 0.05). Notably, there was no correlation with the calculated GFR (p = 0.19, r = −0.17). There was no difference between males and females in plasma klotho levels.
When patients with OSA have been analyzed separately, plasma klotho levels tended to be lower in patients with diabetes (378.7 ± 140.0 vs. 552.1 ± 155.7 pg/mL, p = 0.06). There was a significant relationship between soluble klotho and serum HDL-C concentrations (p = 0.04, r = 0.48) and a tendency for an indirect correlation with triglyceride levels (p = 0.058, r = −0.43). There was no correlation between GFR and klotho levels in OSA patients either (p > 0.05).
Discussion
We reported lower plasma klotho levels in OSA. Reduced klotho concentrations were related to overnight hypoxemia and were also decreased in patients with hypertension. Our results indicated that klotho may play a role in the pathomechanism of OSA.
Only one study has examined klotho in OSA so far. 23 Unfortunately, Saghiv et al. did not give any indication on the diagnostic tests, or if the patients were under any treatment for OSA. Moreover, klotho levels were not compared with clinical or sleep characteristics. Nevertheless, in line with our findings, plasma klotho levels were significantly lower in OSA. 23
CIH is likely to contribute to decreased klotho synthesis in OSA, as there was an indirect correlation between klotho levels and markers of overnight hypoxemia, but not AHI. Of note, patients with OSA had moderate disease in average, and the enrolment of participants with a more severe disease may have resulted in a significant association with AHI.
Hypoxia may lead to increased synthesis of proinflammatory cytokines, 4,5,28 and the elements of resulting inflammation, such as complement factors, 26 tumour necrosis factor-alpha (TNF-α), or interferon-gamma, 29 can decrease the renal production of klotho. The role of hypoxia as a potential inhibitor of klotho synthesis may explain discrepancies reported in COPD, 25,30 as the magnitude of hypoxia in COPD patients participating in these two studies may have been different. In the current study, we found a trend of lower plasma klotho levels in COPD. However, this has to be interpreted carefully due to the very limited number of patients with COPD (n = 5).
Another potential reason for lower klotho may be vitamin D deficiency in OSA 21 as it is known that vitamin D induces renal klotho synthesis. 20 However, it is not likely that disturbed sleep, another important phenomenon in OSA, is strongly associated with klotho expression, as no correlation was found between klotho levels and markers of sleep architecture (i.e., TST, AI) or daytime sleepiness (i.e., ESS).
Reduced klotho levels may contribute to the pathomechanisms of OSA. Klotho suppresses the expression and secretions of inflammatory molecules such as the intercellular adhesion molecule-1, 31 interleukin (IL)-6, 32 and IL-8 33 that are all elevated in OSA. 34 Klotho can also prevent oxidative stress. 15 Thus, a reduction in klotho expression can contribute to accelerated systemic inflammation and oxidative stress. Although we did not find a significant relationship between CRP and klotho levels, analyzing inflammatory mediators that are directly associated with klotho may aid in understanding the potential anti-inflammatory role of klotho in OSA.
In line with a previous study, 35 we found decreased klotho levels in patients with hypertension. It was reported that klotho blocking resulted in increased aldosterone production and subsequent hypertension in mice. 14 Hyperaldosteronism has been observed in OSA and plays a role in OSA-related hypertension. 36 Klotho has also been shown to induce eNOS synthesis. 16 Hence, reduced klotho in OSA may contribute to endothelial dysfunction frequently reported in OSA. 37
Klotho deficiency leads to renal structure damage (glomerulus collapse, tubule fibrosis) and functional decline. 14 An increased prevalence of renal failure has been acknowledged in OSA, 38 which may also contribute to hypertension. Of note, we excluded patients with known renal failure, as klotho production may per se be influenced by renal function. Hence, we did not find any difference in GFR between patients and control volunteers. This may explain the lack of expected correlation between GFR and klotho.
Around 50% of obese people suffer from OSA, 1 and ∼70% of patients with OSA are obese. 39 Patients with morbid obesity had lower klotho levels in a previous study 22 ; however, the authors did not consider OSA as a covariate. 22 Obesity may itself trigger systemic inflammation, 40 which could lead to reduced klotho levels. Although the BMI of the OSA group in our study was significantly higher, there was no correlation between BMI and klotho values, which is in line with our former report. 25 However, most of the volunteers in our study had normal BMI.
To investigate the potential bias due to obesity, we did a subgroup analysis only in nonobese participants. Most notably, the relationship between plasma klotho levels and markers of overnight hypoxemia remained significant in nonobese population. However, to analyze the effect of obesity in OSA, further studies comparing obese controls with obese patients with OSA are warranted. It is acknowledged that waist-to-hip ratio may be a better predictor of metabolic syndrome compared with BMI. 41 However, this has not been registered in our study.
The study was powered to find a significant correlation between markers of overnight hypoxemia and plasma klotho levels. Although all patients were referred due to suspected OSA, partly because of relatively strict inclusion criteria, the analyzed population became inhomogeneous in terms of the ratio of patients and controls. This is a potential limitation, which needs to be addressed in further studies. In addition, patients in our study had relatively mild disease; consequently, the magnitude of overnight hypoxia was moderate.
Despite this limitation, we found a significant indirect relationship between overnight hypoxemia and plasma klotho levels even in mild disease, suggesting that this association would be more robust if analyzing more severe patients. Therefore, to understand the role of klotho in disease pathomechanism and related comorbidities, inclusion of patients with more severe disease is warranted. Of note, more severe OSA is related to an increased likelihood of comorbid obesity and cardiovascular disease, which are associated with reduced klotho levels. 17,22 These comorbidities may be potential biases when evaluating klotho in severe OSA.
In addition, obese OSA patients with more severe overnight hypoxemia are prone to developing overnight hypoventilation and subsequent night and daytime hypercapnia. Hypercapnia may itself alter systemic inflammation. For instance, it may blunt the TNF-α response, 42 theoretically leading to higher klotho levels. 18 Therefore, it would be worthy to investigate patients with more severe OSA with a high burden of overnight hypoxemia (i.e., TST90% ≥ 10%) with and without hypercapnia.
Moreover, similar to our previous report, 24 we found unexpectedly high plasma klotho levels in some control participants. These subjects did not differ in terms of demographics or comorbid profile from other controls, and the reason for high klotho levels needs to be explored as these may potentially explain protective mechanisms against aging, inflammatory, and oxidative stress-related events.
None of the subjects have previously been treated for OSA. The effect of treatment, such as CPAP, on klotho levels should be investigated to reveal the interrelation between klotho and overnight hypoxia. Our study may serve a potential basis for sample size estimation when designing future studies.
Recently, promising animal studies have investigated the effect of klotho supplementation in chronic kidney disease, cognitive impairment, or muscle function. 43 –45 It would be valuable to elucidate whether klotho might serve as a biomarker of increased likelihood for comorbidities in OSA, or whether the molecule holds any therapeutic potential in preventing complications.
In summary, we demonstrated that the levels of soluble klotho are reduced in OSA. Decreased klotho levels are likely to be a consequence of CIH and may also play a role in accelerating systemic inflammation, endothelial dysfunction, and development of comorbidities.
Footnotes
Acknowledgments
The study was supported by Hungarian Respiratory Society grants to A.B. and D.L.T., as well as Semmelweis University grant to L.K. This publication was supported by the Janos Bolyai Research Scholarship of the Hungarian Academy of Sciences to A.B. The authors are also grateful to Elektro-Oxigén Inc. for providing polysomnographic devices, and Mrs. Monika Banlaky for her assistance in polysomnographic measurements. A.B. is supported by the NIHR Manchester BRC.
Author Disclosure Statement
No competing financial interests exist.