
Abstract
Research highlights the benefits of regular traditional multicomponent training in older adults. The potential effect of exergames on perceptive–cognitive and physical function in prefrail older adults is still little explored. The study aimed to compare the effects of two physical exercise training programs (exergaming vs. traditional multicomponent) on perceptive–cognitive and physical functions of prefrail older adults. This study was a randomized controlled trial having 66 prefrail older adults assigned to two groups (exergame group [EG]: n = 32, 70.84 ± 4.53 years; multicomponent group [MG]: n = 34, 70.76 ± 5.60 years). Frailty phenotype, fall history, basic and advanced cognition, perceptual, physical (mobility, gait speed, and balance), and muscle (strength and power) functions were evaluated. Intervention was conducted during 12 weeks. The EG and MG performed similar exercise routines involving the main lower limb muscle groups required in daily activities. A mixed model analysis of variance (ANOVA) and effect size (d) revealed that both programs were effective in postponing frailty status, reducing the fear of falling (EG: d = 1.65; MG: d = 1.40), increasing fall risk awareness (EG: d = 2.14; MG: d = 1.60), improving cognitive status (EG: d = 0.83–2.61; MG: d = 0.86–1.43), muscle (EG: d = 0.54; MG: d = 0.51–0.73), and physical function (EG: d = 0.97–1.55; MG: d = 1.01–2.23). The exergame training might be a better alternative to improve cognition, whereas the multicomponent program may be a better option to provide physical function gains.
Introduction
Regular physical activity has been considered as a relevant countermeasure as it impacts on physical capacity, 1 perceptive–cognitive functioning, 2 and other aspects that are severely influenced by aging and frailty status. Multicomponent exercise training (i.e., routines combining strength, aerobics, and balance) is recommended to frail 3 as it has positive effects on strength, power, and balance, 4 which bear relevance concerning critical aspects of functional independence of improvements in prefrail older adults. 5 Physical exercise also benefits perceptive–cognitive functioning with increases in attention, processing speed, executive function, and memory. 6 Besides, regular physical activity is known to contribute to perceptive–cognitive modifications that increase fall risk awareness and risk of falling. 7
Despite the general benefits associated with regular physical activity, the actual nature of these activities vis-à-vis their complexity has gone underreported in the literature. For instance, it is likely that exercises involving low complexity demand (i.e., activities that require minimal skill involving repetitive and/or negligible central control) may produce important physiological and physical function responses but less pronounced effects on perceptive–cognitive aspects. 8
Although training protocols focusing on specific components such as aerobic, balance, and strength in isolation or in combination (i.e., multicomponent training) have been shown to influence perceptive–cognitive aspects, training protocols, including physical and cognitive components, have failed to show more pronounced gains than the “traditional” programs (i.e., designed to primarily promote changes in the physical domain). 9 It has been speculated that physical exercise intervention that naturally involves simultaneous perceptive and cognitive stimulation would produce broader effects on both domains. 6
For instance, including virtual reality perceptive–cognitive challenges to stationary cycling have been proposed as a more effective approach for improving executive functions than traditional physical exercise in older adults. 10,11 It is reasonable to assume that high complexity activities (i.e., involving mental engagement related to skill learning, strategy development, exergames, and so on) may elicit more prominent changes in perceptive–cognitive domains than those of low complexity, predominantly designed to improve physical or physiological domains. 12
Exergaming has thus been indicated as an attractive way to provide simultaneous physical function and perceptive–cognitive stimuli 13 and is considered as more motivating than traditional repetitive exercise routines. During exergame practice, instantaneous feedback is provided, and physical demands can be increased by adjusting the game level complexity. 11,14 There is compelling evidence regarding the effects of exergames on static and dynamic balance, functional mobility, 13 cognition, 15 and fall rate reduction. 14 In contrast, there is still a lack of evidence that exergaming produces similar benefits (perceptive–cognitive and physical function) in comparison to traditional multicomponent exercises, which are deemed as effective in promoting substantial physical function changes.
This study aimed to compare the effects of two physical exercise training programs (exergaming vs. traditional multicomponent) on perceptive–cognitive and physical functions of prefrail older adults. Moreover, it aimed to determine which training program benefits most prefrail older adults as they are more prone to falls and present reduced performance in several domains (perceptive–cognitive and physical functions).
Materials and Methods
Participants and sample size
The inclusion criteria were as follows: (1) over 60 years of age and (2) classified as prefrail. 16 The exclusion criteria were as follows: (1) reduced cognitive capacity assessed by Mini-Mental State Examination (MMSE) adjusted by the educational profile. The exclusion cutoff score for MMSE was 20 points for illiterates, 25 for 1–4 years, 26.5 for 5–8 years, 28 for 9–11 years, and 29 for higher levels 17 ; (2) neurologic disease; (3) arrhythmia; (4) use of orthosis; (5) engagement in exercise programs or surgery on the lower limbs during the past 6 months; and (6) attendance rate <75%, as training benefits could be precluded. Initially, 206 older adults from the local community were recruited. After applying the inclusion/exclusion criteria, 99 were randomly allocated by software-generated random numbers (1:1 ratio) into two groups that trained under exergame group (EG) or multicomponent group (MG) stimuli. There were no inclusion/exclusion criteria about gender, but the sample was unintentionally composed only for women. Frailty incidence 18 and adherence to physical activity practice 19 are higher in women than in men, which may turn our sample suitable for the scope of the study.
Thirty-three participants discontinued the intervention due to the following reasons: personal issues (n = 31), injury unrelated to the intervention (n = 1), and illness (n = 1). Consequently, 66 participants completed all procedures (EG: n = 32, 70.84 ± 4.53 years; MG: n = 34, 70.76 ± 5.60 years), except for the muscle function in which some participants failed to attend the respective assessment for personal reasons (EG, n = 23; MG, n = 22). Figure 1 shows the group allocation and the experimental design. The ethics committee of the University approved all experimental procedures, which were registered in the Brazilian Clinical Trials Registry (RBR-97jm74) and adhered to the CONSORT guidelines.
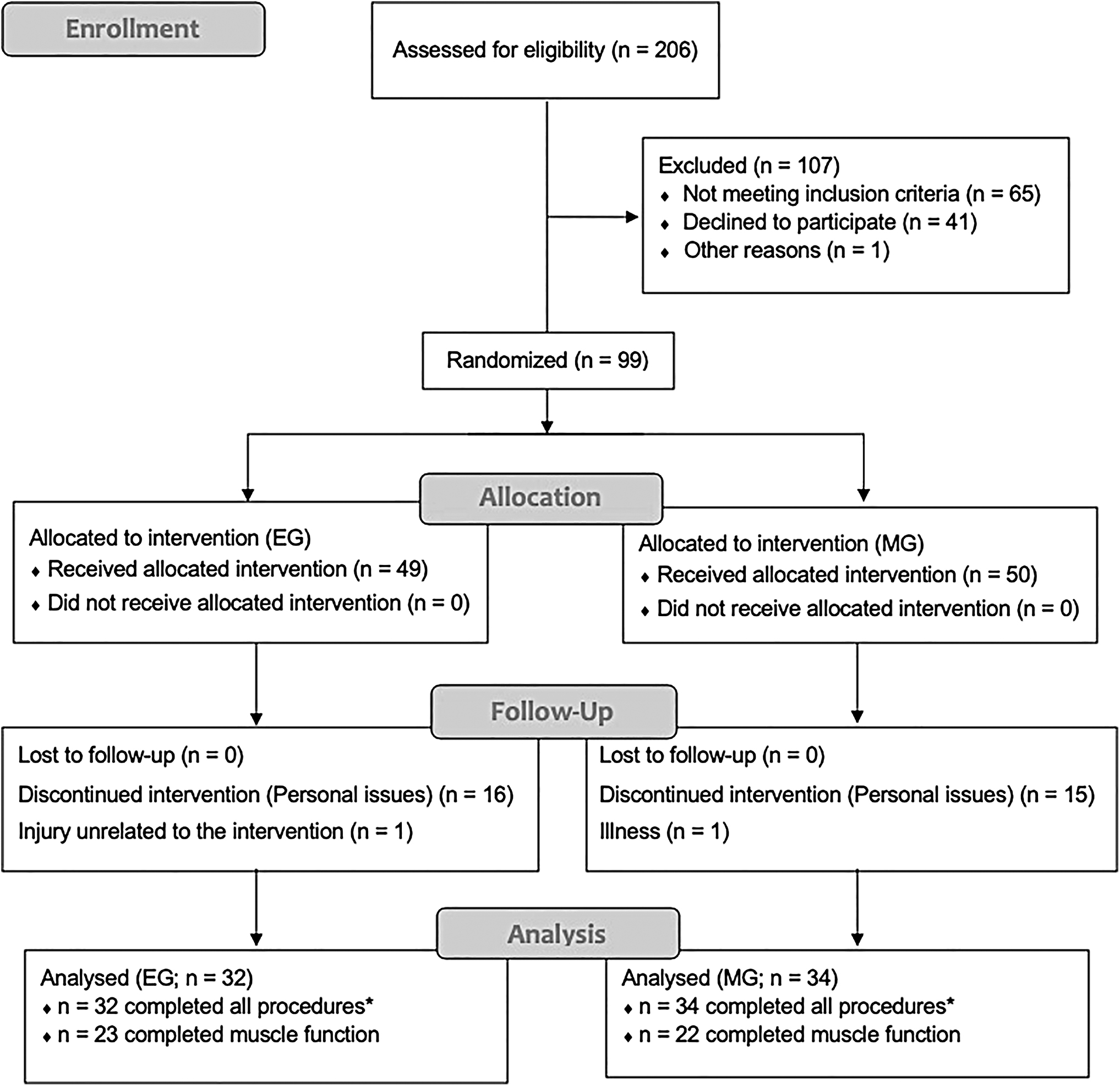
Flow diagram of the study of the EG and MG. EG, exergame group; MG, multicomponent group.
The sample size was calculated by the G*Power program and was based on the indications of Lustosa and colleagues, 20 which showed an effect size of 0.40 in the mobility (timed up and go [TUG] test) after the physical exercise intervention. In addition, the following parameters were considered: (1) F test (analysis of variance [ANOVA]); (2) a 95% confidence level; (3) a sampling error of 3%; (4) power analysis of 80%; (5) number of groups = 2; (6) number of measures = 2 (pre and postexperiment evaluation); and (7) a 10% margin for possible losses and refusals. Therefore, the initial sample estimated 64 older adults, allocated in two groups.
Instruments and procedures
Prefrailty was defined as a clinical syndrome in which one or two of the following criteria proposed by Fried et al. 16 are present: unintentional weight loss (≥10 pounds or ≥5% of body weight in last year), self-reported exhaustion, weakness (handgrip strength), slowness, and low activity. The cutoff points used to classify the individuals were specific of Brazilian older women, as detailed in Table 1.
Cutoff Points of Frailty Phenotype from Brazilian Older Women
BMI, body mass index; HGS, handgrip strength.
Two instruments were applied to the assessment of perceptual aspects related to falls. The Falls Efficacy Scale-International was used to determine the fear of falling using a set of scores (ranging from 16 to 64 points), in which higher scores indicate less fall-related self-efficacy (i.e., increased concern about falling). 21 The Falls Risk Awareness Questionnaire was also applied to determine the risk of fall perception, and higher scores (maximum of 32 points) indicate greater awareness of fall risk. 22
The basic cognition function was assessed by the MMSE, 23 which consists of a 30-point questionnaire in which higher scores denote better cognition. The advanced cognition function was evaluated by the Trail Making Test, in which the subject is instructed to connect a set of 25 dots as quickly as possible, while still maintaining accuracy. 24 The combined score represents the amount of time required to complete the task and the number of mistakes.
Physical function was assessed using six tests performed in a standard order. Participants performed a familiarization trial for the following tests: (1) muscle function (isokinetic dynamic tests of dominant knee flexion and extension in angular velocities of 60°·s−1 and 180°·s−1 (Biodex Medical Systems); testing protocol included two sets of three repetitions of knee concentric flexion/extension movements); (2) handgrip strength of the dominant hand (Jamar® dynamometer according to ASHT recommendations); (3) lower body power (five times sit to stand test); (4) mobility (timed up and go test); (5) gait speed (4 m at comfortable gait speed and 10 m Walk Test at maximum gait speed); and (6) balance (MiniBest Test). The detailed description of the tests can be found elsewhere. 25
Exercise interventions
The exercise interventions were conducted for 12 weeks, with three sessions of 50 minutes per week. The intervention groups (EG and MG) performed similar routines that involved the main muscle groups required to perform daily activities, with special attention to lower limb muscles and according to standard recommendations (American College of Sports Medicine). Training sessions were identical and limited to a maximal of 10 attendants per session. The sessions included 5 minutes of global movements as a warm-up, 25 minutes of strengthening exercises, 15 minutes of balance and cardiorespiratory exercises, and 5 minutes of cooling down. Exercise intensity was monitored using the Borg Rating of Perceived Exertion scale (10–15 on Borg's Scale 6–20).
The EG condition used the Xbox 360 (Microsoft, Inc., Redmond, WA), with Microsoft® Console and Kinect in “Your Shape™: Fitness Evolved” game in all exergame sessions. The strength exercises included squats and lunges (4–6 sets of 8–16 repetitions), while the balance and cardiorespiratory exercises consisted of boxing and lateral and anteroposterior displacements. The cooldown applied Tai Chi Chuan slow-pace exercises. In the EG the participants followed the game instructions to perform the exercises, and exercise progression was determined as proposed within the game (e.g., increasing the number of repetitions).
Participants in the MG performed strength exercise routines of 2–3 sets of 8–12 repetitions involving knee and hip flexion/extension, hip adduction/abduction, hip internal/external rotation, and ankle dorsi/plantar flexion exercises, with 60-second interval between sets. The balance and cardiorespiratory exercises included single-leg stance, semi-tandem and tandem, forward, backward, and lateral displacements, and walking in plantar and dorsiflexion. The strength exercises were performed using ankle cuff weights ranging from 1 to 4 kg. The average weight increment was 3% body mass in the first week, which was followed by gradual increases during the next weeks.
Data analysis
Descriptive statistics (mean and standard deviation) was used to characterize the groups. The Kolmogorov–Smirnov test confirmed data normality. The Chi-square test was used to analyze fall-related aspects. The absolute and relative frequencies were used to analyze the frailty classification. The comparisons before and after the intervention between groups were performed using a Mixed Model ANOVA, followed by the Bonferroni post hoc test. Besides, the delta (Δ) and the effect size (d) were calculated to analyze variations before and after the interventions. The significance level was set at p < 0.05, and all statistical procedures were performed using SPSS (version 25) statistical package.
Results
No differences were observed between groups in all variables before the intervention protocols. The sample was composed only for women without previous experience in exergame technology. Most of the volunteers were using two or more medications (EG: 78.1%; MG: 85.3%), were living with their families (EG: 59.4%; MG: 52.9%), and reported no history of falls in the last year (EG: 53.1%; MG: 55.3%). The physical activity average was 124 and 145 minutes/wk for MG and EG groups, respectively.
Exercise attendance rate was 83.1% for the EG and 81.2% for the MG. After the intervention, there was a significant reduction in the frailty phenotype of both groups (Fig. 2). The exhaustion (EG: n = 31; MG: n = 24) and the physical activity criteria (EG: n = 8; MG: n = 18) were the phenotypes with the highest incidence before intervention. Both training interventions largely influenced these components.
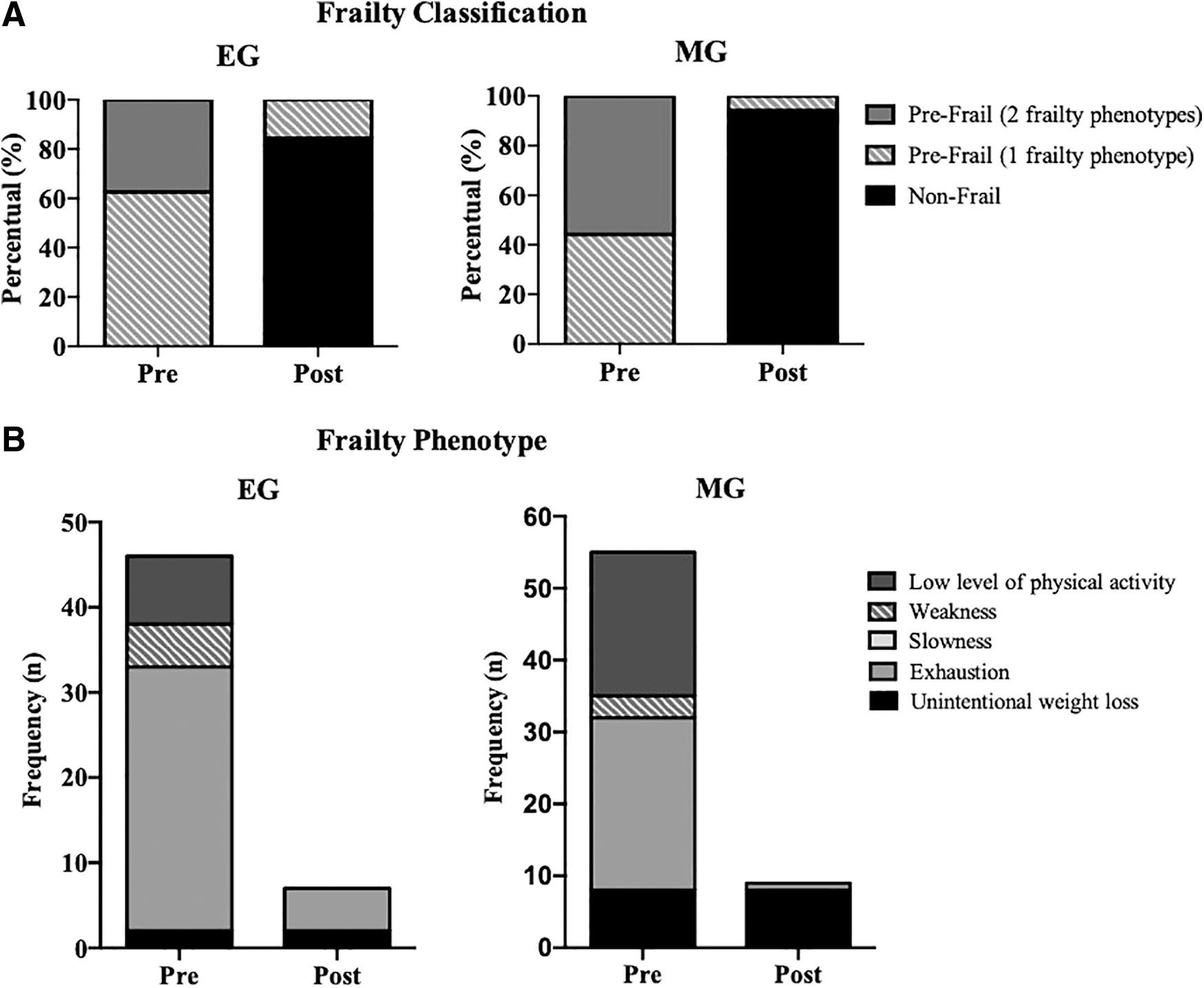
Frailty classification
The EG increased 2.13 points for the basic cognition, F(1,64) = 4.7, p < 0.004, and reduced for the information processing speed (1.03 minutes in part A, F(1,64) = 4.8, p = 0.003; 2.42 minutes in part B, F(1,64) = 4.3, p = 0.006). Both groups decreased the number of errors in part A, F(1,64) = 16.1, p < 0.001; and part B, F(1,64) = 14.1, p < 0.001, with significant differences between groups (postintervention instant). After the intervention, the fear of falling reduced 8.37 points in the EG and 6.82 points in MG, F(1,64) = 11.9, p < 0.001, but did not differ between groups (p = 0.37). In addition, the risk of fall perception increased by 6.07 points in the EG and by 5.27 points in the MG, F(1,64) = 39.2, p < 0.001 (Table 2).
Cognition and Perceptual Aspects at Pre and Postintervention
Data presented as mean (SD).
Significant intragroup difference (from pre to postintervention instants).
Significant intergroup difference (postintervention instant).
d, effect size; EG, exergame group; MG, multicomponent group; SD, standard deviation; Δ, delta.
The power of the knee extensor muscles increased when tested at 60°·s−1 in both groups, F(1,43) = 3.9, p = 0.012. Muscle power [F(1,43) = 3.6, p = 0.015] and total work of knee flexor muscles [F(1,43) = 3.8, p = 0.011] increased in the MG at 60°·s−1. The muscle power [F(1,43) = 4.4, p = 0.007; d = 0.73] and total work [F(1,43) = 3.1, p = 0.017; d = 0.69] increased for the knee flexor muscles of the MG when tested at 180°·s−1 (Table 3).
Data presented as mean (SD).
Significant intragroup difference (from pre to postintervention instants).
Significant intergroup difference (postintervention instant).
EXT, knee extension; FLEX, knee flexion; POw, muscle power; PT, peak torque; PT/BM, peak torque normalized by body mass; TT, total work.
After the intervention, both groups increased static and dynamic balance (EG = 2.41 points; MG = 3.36 points, F(1,64) = 15.8, p < 0.001), muscle power (EG = −4.97 seconds; MG = −4.81 seconds, F(1,64) = 27.7, p < 0.001), and mobility (EG = −2,04 seconds; MG = −2.19 seconds, F(1,64) = 3.9, p = 0.011). The MG also showed an increase of 0.23 m·s−1 in gait speed during the 4 m test, F(1,64) = 7.4, p < 0.001 and 0.21 m·s−1 in the 10 m test, F(1,64) = 5.7, p = 0.007. There was no difference in the handgrip strength postintervention in both groups (Table 4).
Physical Function at Pre and Postintervention in the Exergame and Multicomponent Training Groups
Data presented as mean (SD).
Significant intragroup difference (from pre to postintervention instants).
TUG, timed up and go.
Discussion
This study compared the effects of two physical exercise training programs (EG and MG) in prefrail older adults. The main finding was that both intervention programs were effective in positively influencing the frailty phenotype, fear of falling, fall risk awareness, cognitive functioning, and physical functions. However, exergames were more effective in improving basic and advanced cognition. In contrast, the multicomponent intervention was more effective in improving physical function.
Both physical exercise interventions postponed and/or minimized the frailty status classified by 84% (EG) and 94% (MG). Indeed, the physical exercises are deemed as one of the best interventions to postpone frailty, which was comparable to the findings of other studies that have used exergames 26 and multicomponent exercises. 27 These findings reinforce the relevance of physical exercises for prefrail individuals and their importance to prevent further frailty progression. Sedentarism may expose older adults to the development of accumulating morbidities and aggravate frailty. The physical conditioning improvements derived from both intervention programs may have played a role in reducing fatigue and exhaustion perception and improving the general health status, which are critical aspects for the frailty phenotype assessment. 16
The more substantial gains in the perceptive–cognitive aspects experienced by the EG may be related to the exergames complex nature, as most exercises include dual-task components. For instance, during the exergame practice, participants must interact and focus on the demands required to reproduce movements and provide responses according to different stimuli. 28 These actions involve perceptive, cognitive, and motor functions simultaneously. Exergaming may constitute an interesting approach to stimulate cognitive abilities, working memory, spatial navigation, and representation through the activation of the temporal lobe and parietal structures. 29 These adjustments can improve the reasoning, logic, speed of information processing, and other aspects. 30 Thus, these adjustments may account for the higher rate of perceptive and cognitive improvements in the EG in comparison to the MG.
The fear of falling and the fall risk awareness are essential perceptual components to prevent falls 7 and also improved after both interventions. It may be viewed as a side effect of the perceptive–cognitive improvements, which may have enhanced the participants' capacity to recognize and anticipate possible risk conditions. It may have influenced the “affordance” 31 as the participants were more aware and capable of perceiving the relationship between environmental properties and of its action system properties. The association of these changes may have also increased safety and self-confidence aspects, which may lead to improved physical function, social interaction, reduced fear of falling, and, consequently, diminished fall risk. 1 These associations support our findings and support the relationship between awareness and fear of falling and fall risk in older adults.
The MG stimuli was sufficient to cause changes in all physical function tests. Positive results on physical function derived from multicomponent have been a common finding in a large number of studies that have demonstrated comparable outcomes. 27 The exergaming failed to produce substantial muscle function improvements, but was as effective as the multicomponent program to promote equivalent physical function gains (e.g., balance, sit-to-stand, and TUG increased performances).
Two arguments can be forwarded to explain why strength (as measured by peak torque) failed to account for the increased functional performance. First, physical function is more sensitive to changes in the capacity to produce power than muscle strength itself. 32 Training stimuli using lower loads and fast movement speeds are more suitable to decrease the activation threshold of fast-twitch motor units and increase their initial firing rates to cause expressive power production and rate of torque development. 33 The improved ability to produce a faster torque initiation may help to improve functionality and to prevent falls. 34 The second argument refers to the fact that physical function does not rely exclusively on the ability of the lower limb muscles to generate strength and/or power, but it also depends on other sensorial and neuromuscular aspects that are centrally driven (e.g., balance, solving dual-task demands, perceptive and cognitive aspects, and so on). Training routines, including complex exercises involving sensorial challenges, task constraints (e.g., the reduced base of support), perturbation, and sensory-motor deprivation, may produce increased functional outcomes that cannot be isolated or dissociated from training routines.
These arguments may also explain the marginal improvement in walking speed in the EG. Although TUG is predominantly influenced by the ability of the performer to walk at self-selected (e.g., 4 m walking test) and fast speeds (e.g., 10 m walking test), other aspects may play a more predominant role (e.g., balance and other sensorial, perceptive, and cognitive aspects). The TUG is a complex test that may represent overall physical function changes in response to training. For instance, the fast changes in direction imposed during both training programs are likely to impact on physical functioning (e.g., rising from a chair and ascending/descending stairs) and have also promoted strength gains in the muscles spanning the knee.
Despite the lack of statistically significant changes in the peak torque of the knee extensors and flexor muscles, the risk of severe mobility limitation was modified and progressed from high to moderate in the EG and from moderate to low in the MG. These findings may reflect the clinical relevance of both interventions. However, strength training, as many other training routines involving repetitive movements, has long-term adherence issues. 35 Thus, interactive and playful activities such as exergames may be an attractive alternative to keep older adults engaged longer in physical activities.
Some practical applications can be drawn. The first refers to the postponement of frailty status. Both interventions (EG and MG) delayed frailty status. Postponing frailty using exercise interventions may allow older adults to remain physically independent and in a nonfrail status over a more extended period. Therefore, exercise is one of the alternatives to prevent and delay frailty adverse effects. The second refers to the specific effects of exergaming on perceptive–cognitive aspects, which were more pronounced than multicomponent exercise. Besides, exergames can be considered a dual-task activity, and the interaction between older people and exergames may stimulate brain regions related to cognition. The third refers to multicomponent exercise effect on muscle function. In the present study, the progression and overload of the exercises showed a significant impact, which amplified health promotion possibilities in prefrail older adults.
The reduced number of participants along with the large dropout rate are limiting factors, although the reasons were unrelated to the intervention programs. The absence of a control group and ankle and/or hip measures in the muscle function assessment are also limitations. The assessment of these muscles is relevant as they play a relevant role in activities, especially those involving locomotion or complex tasks (e.g., dressing). Future studies are required to observe the influence of other relevant aspects such as gender, institutionalization status, different ages, and health conditions. The comparison of exergames with other training protocols and physical activities (e.g., walking programs) is required to confirm the positive effects observed in the present study over perceptive and physical aspects of older adults.
Conclusion
Exergame or multicomponent exercise training routines were effective for postponing frailty. The fear of falling and fall risk awareness improved after the training program. Both programs can be considered as relevant options to prevent and delay frailty aspects in older adults, as well as improving cognition and physical function. The present study provided evidence that exergames might be a better alternative to improve basic and advanced cognition functions, while multicomponent exercises may be a better option when the training is designed to provide physical function gains.
Footnotes
Acknowledgments
The authors gratefully thank all volunteers who participated and cooperated in this study, the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES) and the Programa de Pós Graduação em Educação Física (UFPR).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was financed by the Universidade Federal do Paraná (UFPR) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001 (grant no. 0548/2015; process no. 88887.091671/2014-01; PGPTA Program).