
Abstract
Resistance training (RT) is considered a viable strategy to enhance the autonomy and functionality of older populations. We randomized 49 older women (64.2 ± 3.8) into one of two groups: an intervention group (IG) (n = 29) that performed regimented RT or a nontraining control group (CG) (n = 20). The RT protocol was carried out three times a week for both the upper and lower limbs over a 12-week study period. A 30-second arm flexion test was used to test upper limb endurance and a 30-second chair stand test was used to analyze lower limb endurance. Dynamic balance was tested by a Y balance test normalized by leg length. A Soda Pop test was employed to analyze coordination. Results showed significant improvements in IG versus CG in both upper limb (19.50 ± 1.52 vs. 11.40 ± 2.87, p = 0.001) and lower limb muscular endurance (14.90 ± 3.10 vs. 26.56 ± 3.17, p = 0.001). Moreover, the training group showed superior improvements in anterior and posterolateral balance compared to CG (63.9% ± 3.1% to 70.2 ± 2.1 and 88.1 ± 3.9 to 94.2 ± 2.7 with p = 0.001, respectively). There were no significant differences in coordination outcomes between groups. In conclusion, we demonstrate that RT is effective in developing muscular endurance and dynamic balance in postmenopausal women, but does not influence muscular coordination in the measures studied. Study registered in the Brazilian Registry Clinical Trials Registry (No. RBR-7MZ2KR).
Introduction
Morphological and functional declines characterize the aging process, promoting alterations in anthropometric components (i.e., muscle mass, bone mass density, and fat mass), as well as in neuromuscular patterns (i.e., muscle strength, balance, and motor control). 1 –7 The deleterious changes observed in these components indicate a direct association between aging and reductions in physical function. 8,9 Accordingly, the term “dynapenia” was coined to describe the significant decrease in strength observed with advancing age, and its onset predisposes those afflicted to an increased risk of functional limitations. 7,10 Reductions in lower limb strength are usually related to impairments in gait and balance, reducing the mobility of older adults. The combination of strength reductions, muscle atrophy, and physical inactivity associated with aging results in a condition known as sarcopenia. 2,5,10
Impairments in balance and motor coordination correlate with strength declines and incidence of falls in older adults, which can be even more dangerous when observed in postmenopausal women, which usually presents substantial declines in bone mass when compared to men due to several hormonal changes, leading to severe injuries related to falls. 11,12 Reductions in balance and coordination combine to discourage an active lifestyle, 8,13 triggering alterations that are seen throughout the neuromuscular system after short periods of inactivity. 10,14
Resistance training (RT) has been advocated as an effective strategy to counteract sarcopenia and dynapenia effects in older adults, 15 with reported increases of 5% to 10% in muscle cross-sectional area and improvements of 20% to 100% in muscle strength depending on the exercise/muscle group. 16,17 It has been speculated that resistance exercise requires a continuous activation of antigravitational muscles, and these activations stimulate increases in motor coordination, thus providing beneficial effects on balance, especially in older populations. 18 However, although the beneficial effects of RT on muscular strength are well established, the interdependence with muscle endurance and balance remains controversial. 19
The muscle endurance plays a significant role in the older adults' lifestyle by developing muscle endurance, reducing older populations' inactivity levels. 20 Nevertheless, it has been observed that muscle endurance seems to play a direct role linked to the incidence of falls, considering that one of the most common reported causes of falls in postmenopausal women is associated with muscle weakness and muscle fatigue, suggesting the viability of the muscle endurance development in that population. 21 Therefore, considering the impact of the aging process associated with the postmenopausal, this study aimed to investigate the effects of 12 weeks of RT on balance, muscle endurance, and motor coordination in postmenopausal older women.
Methods
The study employed a quasi-experimental design with repeated measurements, 22 whereby we aimed to assess the effect of 12 weeks of RT on women 60 years of age or older. The independent variable was RT with three dependent variables: muscle endurance, dynamic balance, and coordination. All participants signed an informed consent form, detailing the possible benefits and risks related to the protocols applied during the intervention. The Ethics committee board approved the study (protocol number, CAAE: 03763312.7.0000.0117), and the study complied with the intent and principles of the Declaration of Helsinki for human research.
Subjects
Participants were recruited by the convenience method that employed a three-stage process: (1) mapping of possible locations where the target population could be found; (2) establishment of inclusion and exclusion criteria; and (3) visits to community groups where we explained the research procedures and possible benefits and then, when applicable, invited potential participants to volunteer in the study. We determined a sample size of 41 participants was required based on a priori power analysis using a target effect size (ES) of 0.8, an alpha of level 0.05, and a power level of 0.80. Factoring in an estimated sample loss of 20%, 49 active older women (BMI: 25.1 ± 5.0 kg/m2; age: 64.2 ± 3.8 years; and body mass: 61.3 ± 15.1 kg) were recruited to participate in the training program. 23
Inclusion and exclusion criteria
All participants had to meet the following criteria. Inclusion: (1) postmenopausal, as determined by self-report; (2) classified as physically active by IPAQ questionnaire 24 ; and (3) answer in the negative to all PAR-Q (Physical Activity Readiness Questionnaire) items. Exclusion: (1) presence of joint, neurological, cardiovascular, or respiratory disease that impairs strength training performance; (2) use of medications that affect exercise responses; (3) contraindication to performing intense exercises, based on medical examinations performed within 12 months before the beginning of the evaluations.
Experimental design
Initially, all participants completed an anthropometric evaluation in the Physiology Laboratory of Universidade Federal do Paraná (UFPR) that included assessment of height, body weight, and body fat (%BF). In a subsequent visit, participants were tested for baseline muscle endurance, dynamic balance, and motor coordination. 25 After completing these assessments, participants were familiarized with the RT protocol, which consisted of five exercises for the lower limbs and five exercises for the upper limbs. Following familiarization, a 10-repetition maximum (10-RM) test was conducted to estimate the one-repetition maximum (1-RM) for all exercises used in the RT protocol, aiming to determine the training intensity in each of the exercises performed during our intervention.
Participants were randomly divided into two groups: an intervention group (IG; n = 29) that performed a regimented RT program or a nontraining control group (CG; n = 20) that refrained from any structured exercise. The IG engaged in a 3-week acclimation period using 30% of 1-RM, and then performed 12 weeks of RT using intensities of 60% of -RM 3/4 days a week with a recovery interval of at least 24 hours between each training session. Small adjustments in the workload were made every 4 weeks to avoid problems related to adjustments to the load. Following the 12 weeks of training period, participants repeated the initial testing protocol. All tests and interventions were performed at the same time of the day (morning: 9:00 A.M) to avoid the potential influence of circadian variations.
RT protocol
RT was carried out for 12 weeks with training segmented into two protocols: one for the upper limbs and one for the lower limbs. Participants performed three sets of 10 repetitions for each of the 10 total exercises (five exercises for the upper limbs and five exercises for the lower limbs), with a rest interval of 45 seconds provided between sets and 90 seconds afforded between exercises, which seem to be suitable to provide benefits in both muscle endurance and muscle strength. 26 Figure 1 depicts the specifics of the training program.
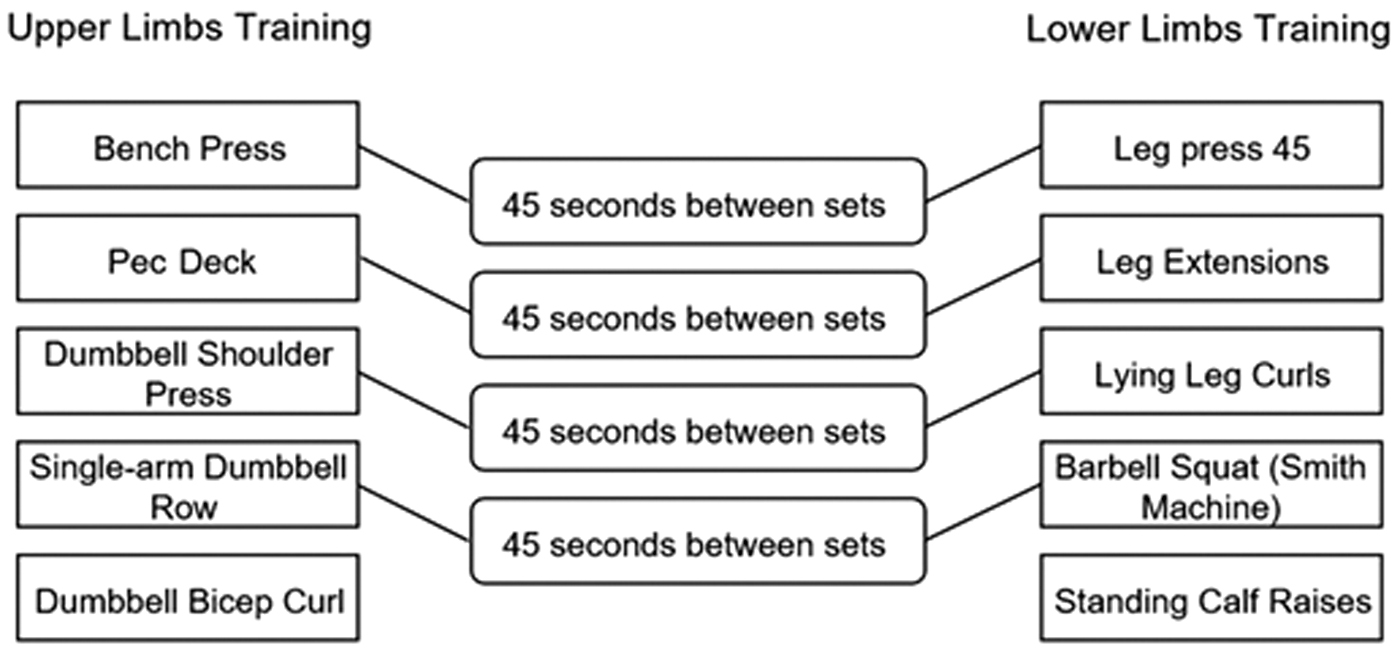
Training protocol for upper and lower limbs.
Instruments and procedures
Anthropometric components
In the first visit to the laboratory, we assessed participants' body weight and percent BF using a tetrapolar bioelectrical impedance analysis device (Model TFB-310, Tanita Corporation, Tokyo, Japan). Height was measured with a stadiometer (Holtain Harpen®) affixed to a wall following a standardized protocol. 27 BMI was calculated as the body weight, in kilograms, divided by the square of the participant's height, in meters (kg/m2). The complete anthropometric components in CG and IG are displayed in Table 1.
Baseline Anthropometric Values for Control Group and Intervention Group (N = 49)
p < 0.05.
BF, body fat; CG, control group; IG, intervention group.
Ten RM test
The objective of the first training session was to estimate the 1-RM values for each of the exercises using the 10-RM test, as proposed by Haff and Triplett. 28 This protocol was employed to gauge the maximal intensity (100%) of each exercise. Thus, the values for the training intensity (60% of 1-RM) were calculated and then used during the training sessions. Considering the muscle strength development associated with the training method and to avoid load adjustments and, therefore, reductions in the proposed load of 60% of 1-RM, a new evaluation was conducted every 4 weeks to estimate the appropriated 1-RM values.
Upper limb endurance
Upper limb endurance was assessed by the 30-second arm flexion test. 25 After being informed about the testing procedures, participants were instructed to sit in a chair without a backrest, holding a halter (2.27 kg) with their dominant arm and hand, and assuming a semipronated position. The movement comprised elbow flexion and extension throughout a complete range of motion performed as fast as possible for 30 seconds (TIMEX® timer). Three attempts were made with a five-minute rest interval between trials. The highest number of repetitions performed during the trials was accepted as the final value.
Lower limb endurance
Lower limb endurance was assessed by a chair stand test, which had a 30-second limit to reach the highest number of repetitions. 25 Participants were positioned with their arms crossed at the chest line in a chair without a backrest, with both feet planted on the floor. The participant performed the complete movement of getting up and sitting on the chair as many times as possible over the 30-second period. Three attempts were made for the chair stand test, with an interval of five minutes between each trial. The best result of the three tests was taken as the final value.
Dynamic balance test
A Y Balance Test (YBT) was used to assess participants' dynamic balance. The YBT testing was conducted in a manner as proposed by Gribble and co-workers, 29 where the participant's dominant foot was determined in the baseline analysis. Participants were instructed to reach the maximal anterior, posteromedial, and posterolateral directions (Y-pattern) while standing with their nondominant foot on a central footplate. If the participant's right foot was dominant, the test was conducted in a clockwise direction (anterior/posterolateral/posteromedial); if the left foot was dominant, testing was performed in a counterclockwise pattern (anterior-posteromedial/posterolateral). 30 The test was performed barefoot, and participants were instructed to reach the maximal distance without losing their balance. After the initial instructions regarding the testing procedures, participants performed six practice attempts in each direction. After these familiarization trials, participants performed the test three times, and a final value was obtained as the mean value of three trials. The mean was then normalized by dividing the value in centimeters by the leg length (distance from the anterior superior iliac spine to the most distal aspect of the medial malleolus) multiplied by 100 to obtain the distance reached in terms of percentage of leg length. 31
Motor control test
The coordination test used the “Soda Pop coordination test” component of the Functional Fitness Assessment for Adults older than 60 years (A Field-Based Assessment), 32 which has been validated in the population of interest. 33 The assessment was performed on a flat surface, with a piece of 76.2 cm long adhesive tape attached to the floor. 34,35 Six marks were made on the tape, and were placed at 12.7 cm equidistant from each other with the first and last mark at 6.35 cm away from the ends of the tape. In each of the six marks, another piece of adhesive tape, 7.6 cm in length, was affixed perpendicular to the first piece of tape. If the participant was right-hand dominant, one aluminum can was placed in position 1, another in position 3, and the third in position 5, creating an average distance of 25.4 cm between points 1–3 and 3–5. When the evaluator gave the signal, the participant rolled the can, reversing the base of support at points 1-3-5 as fast as possible. 25 The final score reflected the eye-hand coordination time taken to complete the test.
Statistical analysis
All data are reported as the mean ± standard deviation (SD). Descriptive statistics were used to elucidate measures of central tendencies and variability for the characterization of study participants. The Shapiro–Wilk test assessed the normality of data distribution. A two-way ANOVA (mixed models) with repeated measures was employed to compare the means of the dependent variables at different times and between groups, with a Bonferroni multiple comparison test used to identify any possible differences. The ES was analyzed through a Cohen's D test, using the scale proposed by Rhea (2004), 36 where values <0.41 represent a small ES, 0.41–0.70 represent a moderate ES, and >0.70 represent a large ES. Statistical significance was established a priori at p < 0.05.
Results
Muscle endurance
As displayed in Figure 2, both upper limb endurance (ULE) and lower limb endurance (LLE) showed significantly greater increases for IG compared to CG (p = 0.005 and 0.001, respectively), with large associated ES values (0.82 and 0.89, respectively). A significant within-group difference was also observed in ULE and LLE between preintervention and postintervention at IG (p = 0.01 and 0.006, respectively), with a large associated ES (0.75 and 0.86, respectively).

Upper and lower limb endurance between groups and time (preintervention/postintervention). *p < 0.005. † p < 0.01. CG, control group; IG, intervention group.
Dynamic balance
As shown in Table 2, anterior and posterolateral balance significantly increased in IG compared to CG across the study period (55.3 ± 2.1 to 49.4 ± 4.1 and 79.6 ± 2.7 to 73.6 ± 55 with p = 0.001 and p = 0.005, respectively), with a moderate ES (0.67 and 0.56, respectively).
Absolute Reach Distance Obtained on Y Balance Test
p < 0.05.
Significant difference between CG post and IG post.
Significant difference between IG pre, and IG post.
A significant difference was also observed in anterior and posterolateral balance across the study between preintervention and postintervention in the IG (50.4 ± 2.8 to 55.3 ± 2.1 and 74.7 ± 3.2 to 79.6 ± 2.7 with p = 0.005, respectively) with a moderate ES (0.7 and 0.63). That significant improvement represents an increase of 5.7% in anterior and 6.5% in posterolateral dynamic balance. No other significant difference was observed (p > 0.05).
The relative (normalized) reach distance presented in %, and corrected by the limb length, is presented in Table 3. A significant change is observed in normalized anterior and posterolateral balance between CG and IG across the intervention (63.9 ± 3.1 to 70.2 ± 2.1 and 88.3 ± 55 to 94.2 ± 2.7 with p = 0.001), with a moderate ES (0.69 and 0.56). That improvement represents an enhancement of 10.5% when comparing the GC to IG after 12 weeks of resistance exercise.
Normalized Reach Distance (Absolute Reach Distance/Limb Length * 100) Between Time and Groups
p < 0.05.
Significant difference between CG post and IG post.
Significant difference between IG pre, and IG post.
In regard to prestudy to poststudy IG changes in dynamic balance, the relative anterior and posterolateral balance significantly improved (63.9 ± 3.1 to 70.2 ± 2.1 and 88.1 ± 3.9 to 94.2 ± 2.7 with p = 0.001, respectively) with a large ES (0.76 and 0.71). That improvement represents an increase of 9.8% in anterior and 6.9% in posterolateral dynamic balance.
Motor coordination
As displayed in Figure 3, no prestudy to poststudy differences were identified between CG and IG in markers of coordination (p = 0.305); however, a small ES difference (0.27) favoring IG was noted for this outcome.
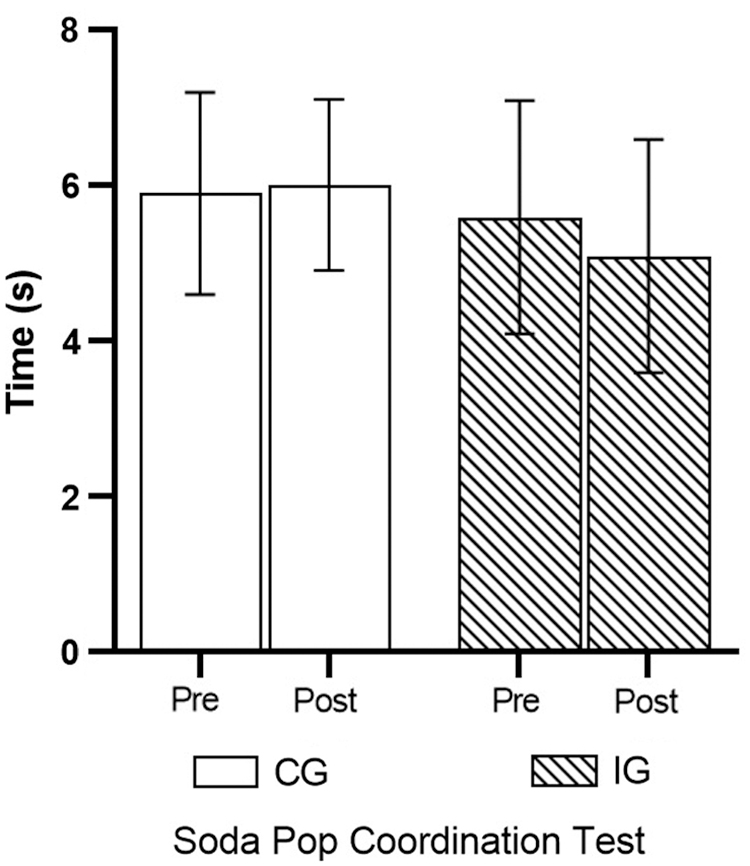
Coordination test between groups and time (preintervention/postintervention).
Discussion
For the best of our knowledge, this is the first study that aimed to analyze the impact of RT on dynamic balance and coordination in postmenopausal older women using a controlled and moderated exercise intensity of 60% of 1-RM. The findings of this study demonstrated that a 12-week RT program elicits significant improvements in balance as well as upper and lower limb muscle endurance in older adults. Alternatively, in contrast to previous reports, we did not find a benefit for RT in improving motor coordination. 37 We discuss the implications of these findings in the context of this literature in the following paragraphs.
This study observed a significant increase in muscular endurance capacity of both the upper and lower limbs. Research indicates that muscular endurance of the lower limbs is directly related to dynamic balance, which in turn is fundamental for the performance of daily activities. 11,38 Aagaard and colleagues 4 demonstrated that RT significantly heightens neuromuscular activation, which is purported to be a primary mechanism responsible for increases in balance. 39 When a moment of imbalance occurs between an individual's center of gravity and base of support, the central nervous system responds by increasing muscular recruitment through efferent signaling. 40 Nevertheless, it is essential to highlight that muscle strength enhancements observed through RT may be responsible for muscular recruitment improvement. 4 Therefore, a greater ability to activate motor units is proposed as a possible mechanism for improvements in balance through RT. 4,39
Regarding balance, other researchers have found balance-related improvements following regimented RT, 19,41 which is consistent with the findings of this study. Conversely, some studies have shown that RT does not significantly improve markers of either static or dynamic balance in adult and older populations. 42,43 It is noteworthy that both studies 37,43 showing no benefit used subjective criteria to determine the intensity of the workout session, and therefore may have either underestimated or overestimated the actual intensity of the workload. Another possible explanation for discrepancies in the literature in regard to balance adaptations may be related to the duration of the training interventions. Some studies showing significant improvements in balance lasted at least 12 weeks, 41,44 while others with shorter durations had null findings. 43,45 Moreover, Schlicht et al. 37,43 did not present significant resistance-related improvements, thus providing a rationale for the lack of improvement in balance. It also is important to highlight that participants only performed lower limb exercises, but the muscle endurance capacity was assessed by upper limb tests, making the lack of similarity between training and testing a potential confounder in determining the true benefits of strength training. 46
RT-induced increases in muscular endurance capacity are usually associated with improvements in the performance of daily tasks such as walking and physical independence, conceivably due to enhancements in muscular coordination that reduce the effort needed to complete routine activities. 47 In this study, participants did not show statistically significant improvements in coordination after 12 weeks of RT, despite a significant increase in muscle endurance. Coordination development may arise from improvements in strength and/or as a result of the motor learning process. 48 The learning process results in the establishment of new neural pathways in the central nervous system; however, it mainly affects gross coordination patterns. 39,48 Therefore, changes in aspects of gross motor coordination may have been masked by the fact that the test used to assess coordination involved a predominance of fine motor skills. It should be noted that, despite a lack of statistically significant differences, a modest ES difference favoring IG was noted for improvements in the test of coordination, suggesting the RT regimen may have played some role in enhancing fine motor skills.
In conclusion, 12 weeks of RT significantly increased markers of muscle endurance and balance in postmenopausal older women. Alternatively, no significant changes in motor coordination were observed, conceivably because of the specificity of the applied testing protocol. These data reinforce the importance of resistance exercise protocols for older populations as a strategy to counteract the detrimental effects of aging on functional performance. This study's main limitation was the lack of specific strength analysis, such as peak force, rate of force development, and power, making it harder to determine the influence of strength development in the balance of the analyzed population. Besides, the motor coordination test applied aims to determine fine motor skills, hiding gross motor coordination development. Future studies should endeavor to investigate the effect of RT on coordination in older adults using strength-specific tasks to better understand its effect on this parameter and consider gross motor coordination tests.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was partially funded by the Coordination for Higher Education Staff Development (CAPES, Grant No. 88882.181208/2018-01). Ferreira et al. were grateful for the financial support from CAPES-PROEX.