
Abstract
Aging induces changes in bone. Growth hormone (GH) is reduced by aging, and age-related changes observed in old bones might be due to a decrease in the GH/insulin-like growth factor-I (IGF-I) axis. GH administration on aged individuals is controversial. This study aimed to assess the effect of systemic GH treatment on bone properties, bone metabolism, and bone mineral density (BMD) in long bone of old rats. Aged Wistar rats were treated with GH at a dose of 2 mg/kg/day during 10 weeks. Plasma osteocalcin, IGF-I, and carboxy-terminal telopeptide of type I collagen levels were measured. Cross-sectional bone areas and BMD were measured by morphometric and densitometric analysis, respectively. Femora were analyzed by three point-bending testing. t-Test was used for statistical evaluation. p < 0.05 was considered to be significant. Significantly enhanced bone area, at the expense of the cortical area, was found in treated rats. The densitometric analysis showed 11% higher BMD in the experimental group. Significantly higher bone flexural modulus, stiffness, and ultimate load were observed in the treated rats. Plasma osteocalcin and IGF-I levels were significantly increased in the treated group, while the resorption marker concentration remained unchanged. Within the limitations of this experimental study, systemic GH administration has shown to enhance biomechanical properties, BMD, cortical mass, and plasma IGF-I and osteocalcin in old treated rats, compared to the control group; consequently, GH could be considered as an alternative therapy against age-related changes in the bone.
Color images are available online.
Introduction
Bone is a dynamic tissue that undergoes the remodeling process, in which old bone is removed by osteoclasts and replaced by new bone by osteoblasts. Under physiological conditions, bone resorption and bone formation are tightly coupled, but, as age advances, the balance between the two processes moves toward bone resorption. Age-related bone changes are associated with reduced bone mass and deterioration of microstructure, increasing the susceptibility of fractures. 1
Age-related changes observed in bone could be due to a functional decrease in the growth hormone (GH)/insulin-like growth factor-I (IGF-I) axis, since both components, GH and IGF-I, decline with aging. 2 GH and its mediator IGF-I play an important role in the pubertal skeletal longitudinal growth, as well as in the appositional growth, which is essential for the acquisition of bone mass accrual during adulthood. 3 It is known that bone mass accrual is maximal in the 30s, thereafter it is maintained until the fifties, and from that point on begins to decrease. This fact is coincident with the decline in GH circulating levels, a process called “somatopause” by Toogood. 4
GH is an anabolic hormone, synthetized mainly in the pituitary gland, but also produced in the liver, lung, and bone, being also recognized as a local growth factor. 5 GH is one of the most important hormones that regulate bone growth and bone remodeling in vivo. 6,7 GH is able to increase longitudinal bone growth by direct stimulation of prechondrocytes in the growth plates 8 and by direct stimulation of osteoblasts, increasing its proliferation and differentiation. 9 GH also increases IGF-I synthesis by the liver 10 ; thus, GH exerts direct and indirect effects on bone. GH is able to increase osteoblast number and function, while IGF-I stimulates only osteoblasts activity. 11 GH and IGF-I exert not only endocrine effects on bone but also autocrine and paracrine effects. IGF-I and IGF-II are the most abundant growth factors deposited in the bone matrix throughout life. 12 IGF-I is a peptide that acts as a local and systemic regulator of skeletal growth. 13 In addition, GH is able to stimulate bone protein synthesis and mineralization, 14 increasing bone turnover 15 and enhancing bone fracture repair. 16,17 However, the potential use of GH for age-related bone loss is controversial, because of the inconsistent results and the possibility of adverse side effects in old population. 18 –21
In contrast, osteoporosis is the most frequent skeletal systemic disease, that affects more than 200 million people over the world, and is considered a major public health problem. 13 Nowadays, two types of therapies can be used for bone-loss disorder treatment: the antiresorptive and the anabolic drugs. The first therapies are most widely used, since bisphosphonates (BPs) are being used during the last forty years, due to its low costs, good results, and relatively low incidence of adverse side effects. BPs are able to increase bone mineral density (BMD) by reducing bone resorption, but, since bone resorption and formation are coupled processes, consequently bone formation is also reduced. There is high evidence that BPs are able to reduce the incidence of all types of fractures compared with placebo, not only vertebral fractures. 22 However, the use of antiresorptive treatments to prevent the risk of fractures in the elderly is beginning to be questioned, since an increased risk of occurrence of atypical subtrochanteric femur fractures and prolongation in the union times of certain fractures 23 have been associated with the long-term use of BPs. 24 Since Marx's article, 25 it is also known that BPs have been related with osteonecrosis of the jaws 26,27 and even with alveolar bone loss around dental osseointegrated implants. 28
Regarding anabolic therapies, the only drug approved by the Food and Drug Administration and the European Medicament Agency for the anabolic treatment of osteoporosis is teriparatide (1–34 parathormone), which has been used successfully for increasing bone mass in the elderly, 13 but this therapy is not recommended for a long time due to a possible increased risk of tumors, as has been shown in the rat model. 29 Although the risk of developing teriparatide-related osteosarcoma is low, 30 there are no clear scientific data, and the general recommendations are to limit its use to 18–24 months, closely following up these patients.
Elsewhere, since receptor activator of nuclear factor kappa B (RANKL) has been considered the major mediator in bone loss, Denosumab, the monoclonal antibody against RANKL, constitutes another good antiresorptive therapy and prevents the risk of fractures, but it has been also implicated in the development of osteonecrosis of the jaws 31 and atypical femur fractures. 32
Regarding GH, its use in the elderly is controversial. Certain authors, such as Krantz et al., 33 have observed 50% of reduction in the risk of fractures in postmenopausal women after 3 years of GH treatment, followed up for 10 years. Landin-Wilhelmsen et al. 34 showed also an increase in BMD in osteoporotic women with GH administration. However, Liu et al., 18 in their systematic review, did not find beneficial effects in old subjects after GH treatment.
Thus, the aim of this study was to assess whether GH could be an alternative therapy to conventional antiresorptive treatments for bone-loss disorders. The authors' working hypothesis was that GH replacement therapy in the elderly might be able to improve some of the age-induced changes in bone properties, bone metabolism, and BMD.
Materials and Methods
Animals
Twenty female 22-month-old Wistar rats were used in this study. Animals were given a standard laboratory rat diet (A.O4 Panlab, Barcelona, Spain) and water ad libitum, in a light- and temperature-controlled room. Rats were divided into two groups (n = 10 per group): Group one remained untreated as old control (only saline and vehicle treated). Group two was the experimental group, treated with GH for 10 weeks amounting 2 mg/kg/day (Saizen; Serono, Madrid, Spain), given in two daily subcutaneous (sc) injections
All the animals received humane care according to the Guidelines for Ethical Care of Experimental Animals of the European Union, and the study was approved by the Ethics Committee for Animal Studies at the Complutense University (Madrid, Spain) and Consejería de Agricultura de la Comunidad Autónoma de Madrid (Spain) with the registration number ES280790000086.
After 10 weeks of treatment, animals were sacrificed by decapitation, and trunk blood was collected and centrifuged to obtain plasma for osteocalcin, IGF-I, and carboxy-terminal telopeptide of type I collagen (CTX) measurements. Both tibiae were dissected from soft tissues, fixed in 10% formaldehyde and cut in blocks to be included in 2-hydroxyethylmethacrylate resin, to be studied under light microscopy. Elsewhere, both femora were collected and fixed in 10% formaldehyde and phosphate buffered solution to test biomechanical properties.
Densitometric analysis
Left tibiae were dissected from soft tissues. BMD in the whole tibia was measured using the XR-26 Norland® densitometer (Norland Medical Systems, Fort Atkinson, WI), in an anterior–posterior direction. BMD was expressed in g/cm2. This densitometric study by dual-energy X-ray absorptiometry was performed following the method previously described. 35
Morphometric analysis
A morphometric study to quantify bone areas was carried out in the right tibiae, which were dissected from soft tissues, fixed in buffered formaldehyde, and cut in blocks to be included in 2-hydroxyethylmethacrylate resin, according to the Donath and Breuner method, 36 to cut undecalcified bone with the Exakt® microtome (Exakt Apparatebau, Norderstedt, Germany). The morphometric analyses were performed in the diaphysis-proximal metaphysis union of each tibia. Blocks of 20 mm thickness were obtained first, including the area to be measured, and then transversal cuts of 200 μm thickness were made with the Exakt cutting band. Each section was ground with the Exakt grinder until a final thickness of 50–80 μm was obtained. These sections were stained according to classical methods (Masson Trichrome and Toluidine Blue) and were observed under light microscopy (Leica, Wetzlar, Germany). The morphometric study was performed with an image analysis software (MIP-4, Digital Image System, Barcelona, Spain) imaging analyser (Digital Image System, Barcelona, Spain). The morphometric parameters directly measured by the MIP-4 in the cross-sectional tibia were: total area, bone area, cortical area, medullar area, and trabecular area, following the method previously described 37 (Fig. 1).

Figure drawing of morphometric parameters directly measured by an image analysis software (MIP-4, Digital Image System, Barcelona, Spain). Morphometric areas directly measured by MIP-4 were schematized in black color.
Mechanical testing
Biomechanical properties of rat femora were analyzed by a three-point bending test, 38 using an Instron 5569 tester (Instron Corp., Canton, MA) on the midshaft of the femora. The span of two support points was 20 mm, and the deformation rate was 0.1 mm/min. Stiffness, Young's modulus, ultimate force, and work to failure were calculated from the resulting load–displacement curves. Stiffness is a measure of resistance of bone to displacement; Young's modulus is a measure of stiffness related to the shape of the object; ultimate force is the maximum force that bone can resist; and work to failure is the energy required to break bone.
Plasma measurements
Trunk blood was collected and centrifuged to obtain plasma. Osteocalcin, IGF-I, and CTX concentrations were determined by different rat-specific immunoassays (ELISA kits, from Biomedical Technologies, Stoughton, MA).
Osteocalcin is an important bone formation marker synthesized by osteoblasts, which reflects new protein synthesis and provides a valuable tool for assessing bone formation. It is an indicator of osteoblast activity. 39
IGF-I is the major mediator of the anabolic effect of GH on bone. 6,7,10,40
CTX is generated by the action of catepsin K during osteoclast resorption. It is a specific marker of bone resorption. 39
Statistical analysis
The mean ± standard deviation of each group was calculated. A Shapiro–Wilk statistical test was applied to assess the normal distribution of data.
GH and control groups were compared using the t-test. Results and the statistical analysis were elaborated by SPSS 22.0 statistical software package. Significance for the analysis was considered when p < 0.05.
Results
Densitometric results
BMD was found to be 0.123 ± 0.005 g/cm2 in old rats, while GH administration increased the values to 0.138 ± 0.006 g/cm2, showing statistically significant differences (p < 0.05) (Fig. 2).

Densitometric analysis. Bone mineral density was found to be 0.123 ± 0.005 g/cm2 in control rats, while GH administration increases the values to 0.138 ± 0.006 g/cm2, showing statistical differences. Values are mean ± standard deviation. *p < 0.05. GH, growth hormone.
Histological analysis
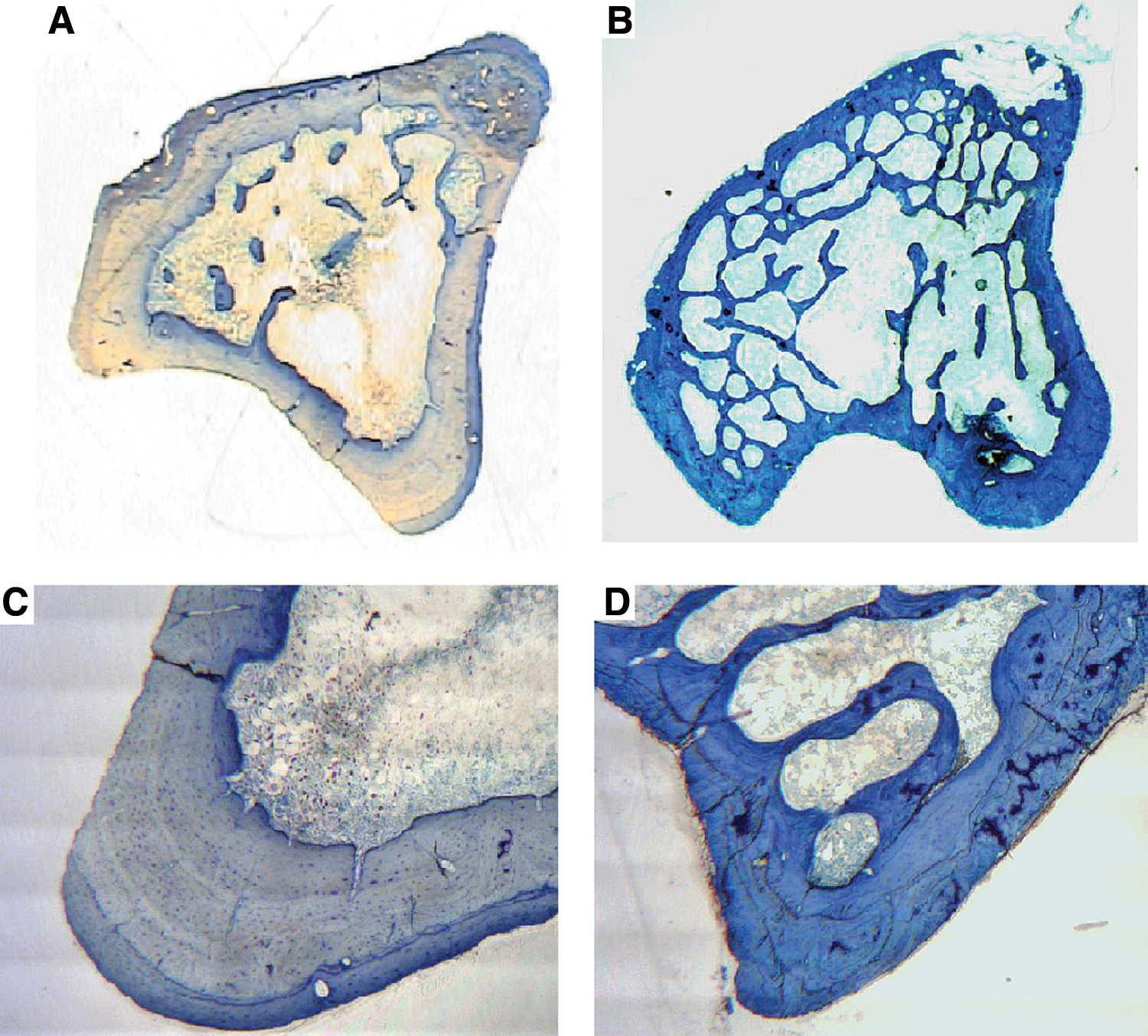
GH specimens show more bone area at the expense of cortical area than the control group (Fig. 3). GH-treated specimens show also greater bone remodeling into the cortical bone compared with the control group (Fig. 4).
Histologic analysis. Specimen with GH [
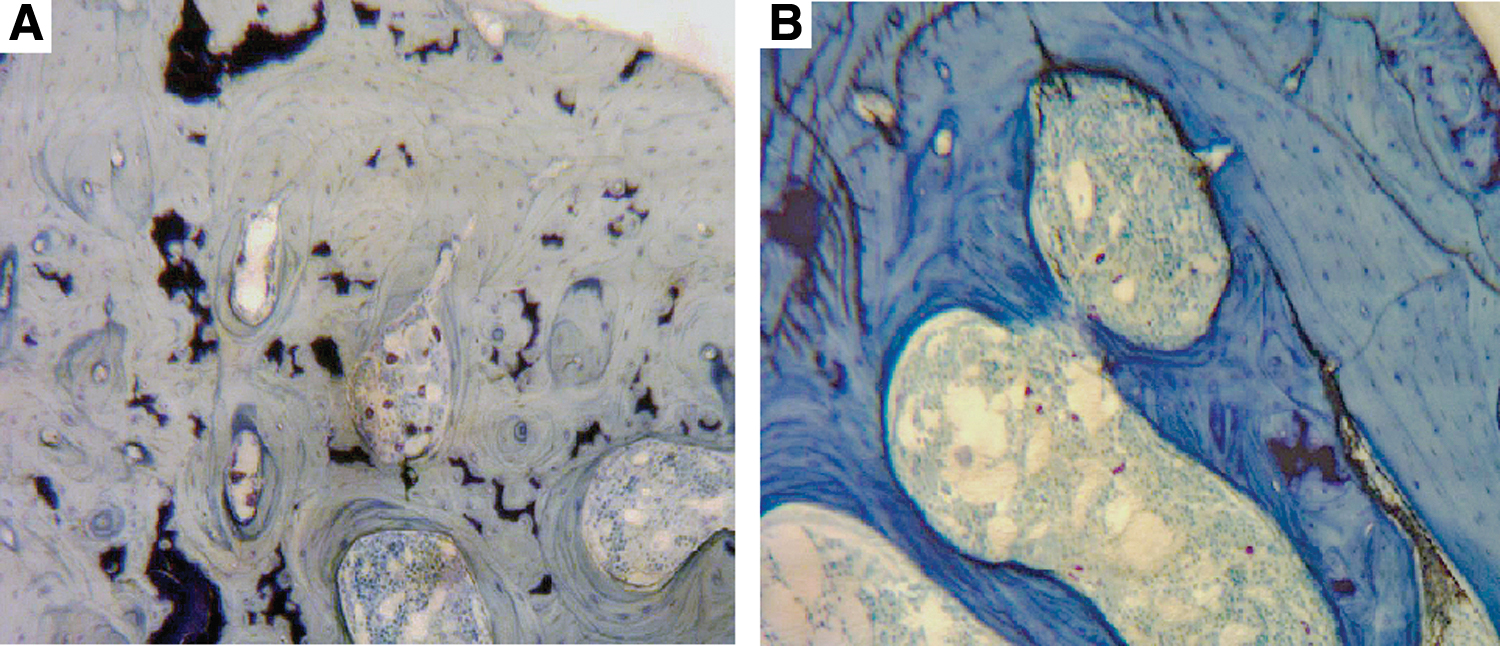
Histologic analysis. Specimen with GH, showing a greater bone remodeling into the cortical bone, with some fronts of osteoblasts [
Morphometric results
In GH treated rats, bone area and cortical area were significantly increased compared with the untreated old rats (6.23 mm2 ± 1.06 vs. 4.46 ± 0.75; p = 0.01; 5.40 mm2 ± 0.28 vs. 4.09 mm2 ± 0.59; p = 0.03, respectively). Total area, medullar area, and trabecular area were also increased, although without statistical significance (12.02 mm2 ± 1.93 vs. 10.07 mm2 ± 1.15; p = 0.12; 6.61 mm2 ± 2.13 vs. 5.97 mm2 ± 0.68; p = 0.5; 0.95 mm2 ± 0.34 vs. 0.43 mm2 ± 0.3; p = 0.36, respectively) (Fig. 5).
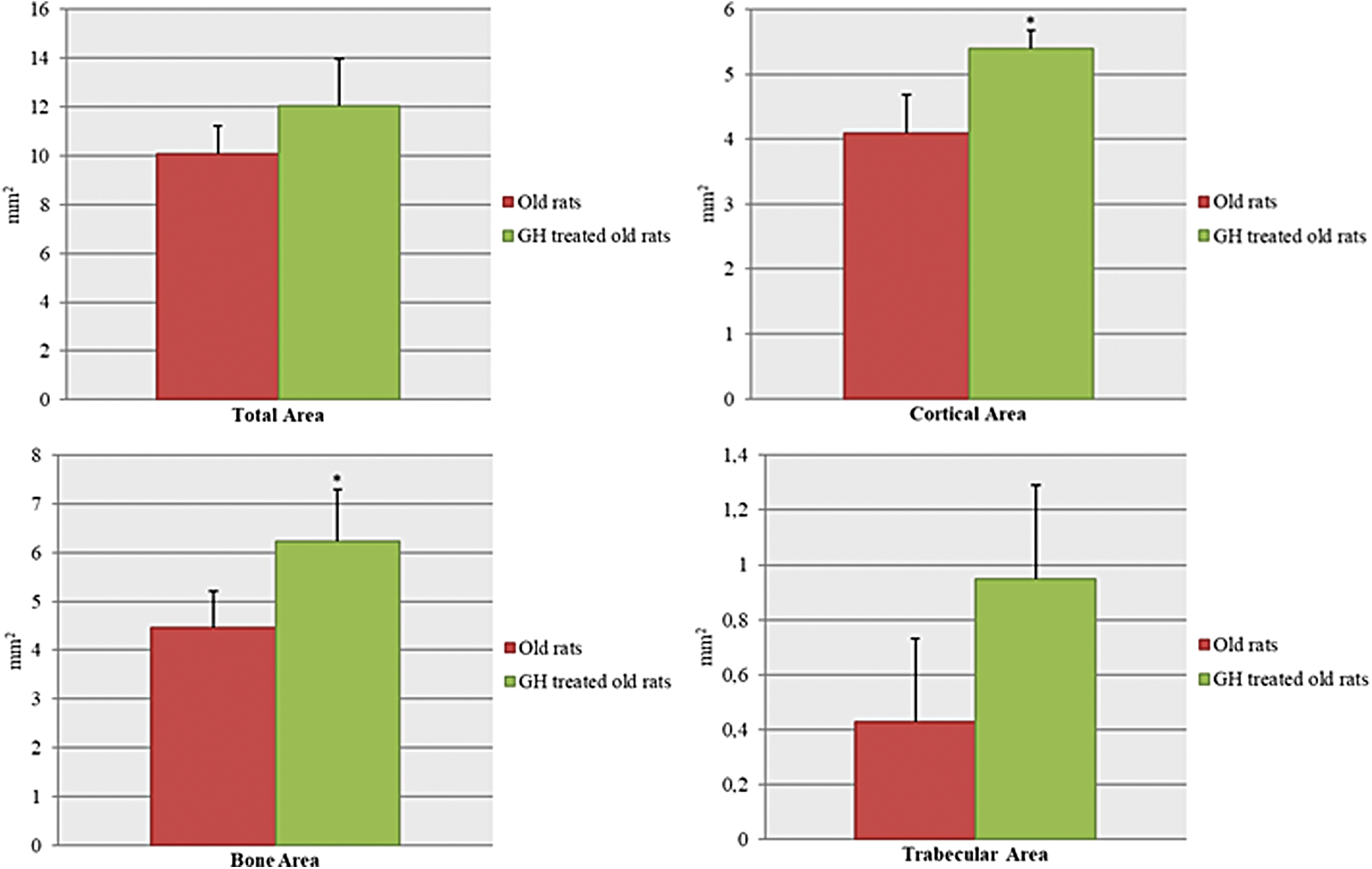
Morphometric analysis. Bone area was significantly increased with GH treatment (6.23 mm2 ± 1.06 vs. 4.46 mm2 ± 0.75; p < 0.05), at the expense of cortical area (5.40 mm2 ± 0.28 vs. 4.09 mm2 ± 0.59; p < 0.05). Total area was increased with GH treatment, although without statistical significance (12.02 mm2 ± 1.93 vs. 10.07 mm2 ± 1.15; p > 0.05), as well as medullar and trabecular areas (medullar area: 6.61 mm2 ± 2.13 vs. 5.97 mm2 ± 0.68; trabecular area: 0.95 mm2 ± 0.34 vs. 0.43 mm2 ± 0.3; p > 0.05). Values are mean ± standard deviation. *p < 0.05. Color images are available online.
Mechanical testing
Analysis of bone mechanical properties showed significantly higher bone stiffness (367 ± 112 N/mm), flexural modulus (2512 ± 756 N/mm2), and ultimate load (141 ± 34 N) in GH-treated rats than in controls (stiffness 201 ± 35 N/mm; flexural modulus 932 ± 83 N/mm2; ultimate load 108 ± 21 N; p < 0.05, Fig. 6). No significant differences were found regarding work to failure.

Mechanical analysis. GH administration was able to significantly increase bone stiffness (288.3 ± 52 N/mm vs. 205.1 ± 34.7), flexural modulus (1227.4 ± 156.3 N/mm2 vs. 837.7 ± 43.5 N/mm2), and ultimate load (121.3 ± 24.4 N vs. 93.7 ± 27.1 N), with regards to the control group. Values are mean ± standard deviation. *p < 0.05. Color images are available online.
Body weight
GH administration for 10 weeks did not induce significant changes in the body weight (mean of 435.3 ± 92 g in GH rats vs. 363.7 ± 33.6 g in old controls).
Plasma bone markers
In the GH group a significant increase in osteocalcin concentration was found compared with the old control group (267 ng/mL ±60.4 vs. 85.2 ng/mL ±13.2; p < 0.05).
In the old GH group, a dramatic increase in IGF-I levels was seen compared with the control group (1115.2 ng/mL ±75.8 vs. 490 ng/mL ±61; p < 0.05), reaching statistical significance.
CTX levels were not significantly changed in the GH group (GH treated 45.5 ng/mL ±12.2 vs. old rats 32.6 ng/mL ±10.1) (Fig. 7).
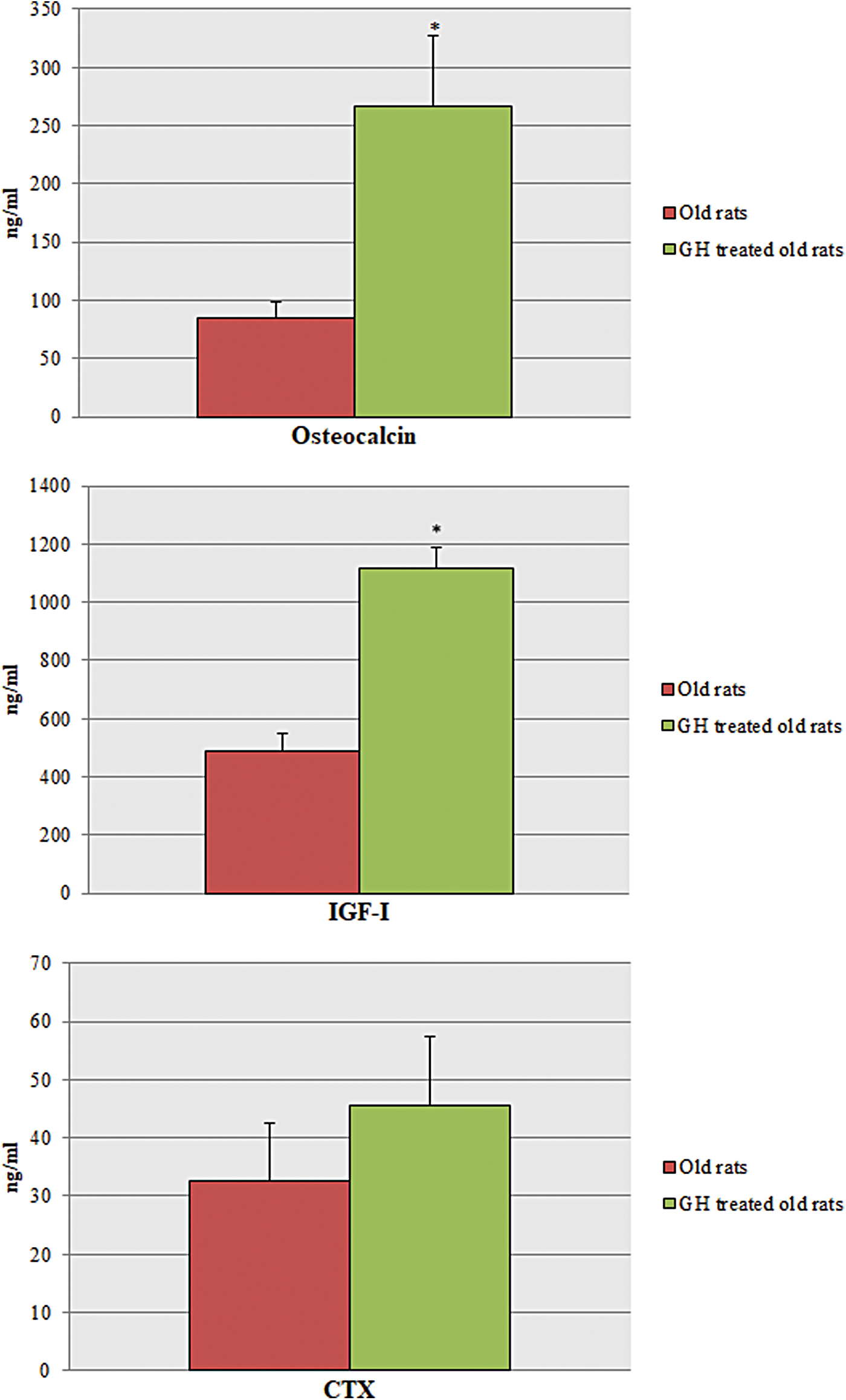
Plasma bone markers. A significant increase in osteocalcin and IGF-I concentrations was found in the GH group (267 ng/mL ±60.4 vs. 85.2 ng/mL ±13.2 and 1115.2 ng/mL ±75.8 vs. 490 ng/mL ±61, respectively), while CTX concentration remained unchanged. CTX, carboxy-terminal telopeptide of type I collagen. *p < 0.05. Color images are available online.
Discussion
Aging is associated with a reduction in the function of most physiological systems of the organism, including bone. Age-related bone changes include a thinner cortical, a reduction in the number of trabeculae, and more space among them, making old bones more likely to break. 1 These age-related changes could be related with the decline in the GH/IGF-I axis. 2 GH secretion is reduced with age, due to multiple factors, including lower levels of physical activity, poor slow wave sleep patterns, and inadequate nutrition, among others. 41 Anabolic hormonal signaling, a healthy nutrition, and regular exercise are crucial factors to maintain an adequate bone mass. As hormones and growth factors are diminished with age, reducing the tissue response to physiological stimuli, it has been suggested that hormone supplementation may be useful in aging, to at least protect the functions of aged organs, like the heart, 42 or to improve oxidative stress in the liver, 43 thus leading to a higher ATP production.
Considerable evidence supports the hypothesis that GH plays an important role in bone metabolism in children with GH deficiency 44 or in GH-deficient adults, 45,46 but effects of GH administration on age-related bone loss are controversial in the elderly population. While Rudman et al. 47 considered that GH administration during 6 months was able to increase 1.6% lumbar BMD in elderly men, other authors like Liu et al., 18 in their systematic review, did not find any positive effects on bone turnover in an old population. Other authors have dismissed its use because of possible adverse side effects that have been associated with GH administration, such as carpal tunnel syndrome, joints' pain, weight gain, glucose intolerance, and edema, 18,19 or even an increased risk of cancer and mortality, as has been reported in adults who received the hormone as children with GH deficiency. 21,48
Our study was carried out to clarify the effect of exogenous GH administration on bone metabolism, mechanical properties, bone areas, and BMD in 22-month-old female Wistar rats. Twenty two months of age in rats is equivalent to 60 years in human age. 49 Experimental rats were treated with two daily sc injections of GH (2 mg/kg/day) for 10 weeks, to investigate its effects on tibiae and femora. However, as the experiment lasted these 10 weeks, at the end of the study rats were 2.5 months older (equivalent to 6 years in humans), that is to say 66 years old for human age. 49
BMD was increased with GH treatment
A statistically significant increase of 11% in BMD values with GH treatment has been found in old rats, in agreement with the data of Verhaeghe et al., 50 who observed an increase of 12%–14% in BMD after 8 weeks of GH administration in aged ovariectomized rats.
In humans, the use of GH administration to increase BMD and to reduce the risk of fractures in an old population is controversial. Recently, Krantz et al., 33 in the largest study to date, with three years of GH treatment and ten years of follow-up, observed an increase in BMD in all studied regions in postmenopausal osteoporotic women, and they found that the incidence of fractures was reduced by half (56% vs. 28%). Elsewhere, Landin-Wilhelmsen et al. 34 found an increase of 14% in total bone mineral content in osteoporotic women also after 3 years of GH treatment. However, in a recent systematic review, Atkinson et al. found no increase in BMD in osteoporotic women with GH administration. 20 This could be due to insufficient treatment periods or low dosages of GH.
Bone area and cortical area were increased with GH treatment
In the current study, a significant anabolic role of GH on cortical bone mass has been observed, but not on trabecular bone, in agreement with Andreassen et al., 51 Verhaeghe et al., 50 Mosekilde et al., 52 and Banu et al. 53 Andreassen et al. 51 found an increase in the cortical thickness of femora at the expense of the periosteum, both at 40 and 80 days after 2.7 mg/kg of GH administration in 2-year-old rat femora, similar to our data.
The increase in cortical bone mass that has been observed in the current study is associated with an increase in mechanical strength, as was described previously by Mosekilde et al. 52 This anabolic response could be due to a direct effect of GH on periosteal bone apposition, but also to the indirect action exerted through IGF-I, as suggested by Yakar and Isaksson. 54
Regarding the trabecular bone, no effect was morphometrically demonstrated with GH treatment, in agreement with Andreassen et al., 51 Mosekilde et al., 52 and Andreassen and Oxlund. 55 The latter authors concluded that in old rat, without linear growth, GH treatment did not influence neither cancellous bone volume nor trabecular thickness. These results are partially different from others obtained by our group with locally administered GH. When 1.3 mg of GH was applied into an ostectomy before the surgical implant insertion in osteoporotic rabbits, a great bone neoformation was observed from both the periosteum and the endosteum. 37 Maybe 1.3 mg dose of GH administered locally was so high that it could directly stimulate osteoblasts from the endosteum. However, taking into account the current histological results, GH was found to enhance not only the cortical thickness but also accelerate the remodeling process into the cortical bone, as can be seen in Figure 4.
GH is able to increase biomechanical properties
GH is able to significantly increase bone stiffness by 200%, flexural modulus by almost 300%, and ultimate load also by 200%, increasing the strength of femoral diaphysis. This could be due to the new bone apposition from the periosteum even under aging conditions, in agreement with Andreassen and Oxlund. 55 These improvements in biomechanical properties could be of interest to prevent and treat fractures and the delayed fracture consolidations in the elderly.
In humans, these data are consistent with those of Krantz et al., in which a dramatic reduction in fracture incidence was observed in osteoporotic women after 3 years of GH treatment. 33
Plasma osteocalcin and IGF-I levels were increased with GH treatment
GH administration induced a dramatic and statistically significant increase in osteocalcin levels compared with untreated old rats (by more than 300%), indicating a direct effect of GH on osteoblast proliferation and differentiation, 9 even under aging conditions. Osteocalcin is a γ-carboxyglutamic acidic protein secreted solely by osteoblasts, 56 whose levels are reduced by age. 57 In the current study, a great increase in osteocalcin levels has been observed after chronic GH administration, in agreement with Yeh et al. 58
Moreover, IGF-I levels increased by more than 200% in the GH group, due to a direct effect of GH on hepatic IGF-I release capacity, as could be expected. These increased levels reflect an anabolic effect on bone, since IGF-I is able to stimulate osteoblast function. 13 Although IGF-I does not have a direct effect on osteoblast differentiation, Playford et al. 59 have suggested that it is able to stabilize β-catenin, enhancing Wnt-dependent activity and indirectly stimulating osteoblastogenesis.
CTX levels were not changed
CTX (carboxy-terminal telopeptide of type I collagen) is a marker of bone resorption, which is released to the bloodstream after catepsin K action. Cathepsin K is one of the main catalytic enzymes secreted by the osteoclast. It plays a role in the degradation of type I collagen from the bone. 39
In the current study, GH administration was not able to induce significant differences on CTX levels, even though GH is able not only to increase bone formation 9 but also to increase bone resorption, 60 thus stimulating the remodeling process. Perhaps, if the markers had been measured in the early stages of the experiment, the CTX levels would have been higher, because of the initial effect of GH on bone resorption. In addition, when GH has been applied to older women to increase BMD, during the first 6 months, the markers of bone resorption have prevailed over those of bone formation. On humans, 1 year of GH treatment seems not to be enough to produce effects on BMD, as observed by Saaf et al. 61 At least 18 months of GH treatment seems to be necessary to induce new bone formation and new mineralization in osteoporotic women.
GH doses and duration of the experiment
In the current study, GH has been injected to old rats at a dose of 2 mg/kg/day (7 days per week) in two daily injections. This amount was lower than the 2.5 mg/kg/day used by Banu et al. 53 and Mosekilde et al. 52 or the 2.7 mg/kg/day used by Andreassen et al. 51 and Bak and Andreassen. 62 However, Yeh et al. 58 found no differences on cortical bone areas with 0.5 mg/kg of GH (5 days per week) for 9 and 16 weeks, although most authors observed significant effects on cortical bone when the dose of GH was higher than 1.25 mg/kg/day.
The duration of GH administration in the current study was 10 weeks, similar to Banu et al., 53 but other authors' studies lasted longer, as the 80 days of Andreassen et al.'s article 51 and Bak and Andreassen's 62 or the 3 months of study by Mosekilde et al. 52
Mechanism by which GH could improve old bone properties
In the elderly, GH secretion is reduced, 2 –4 and many of the age-related signs and symptoms, like muscle and bone mass loss, increased adiposity, and even psychological alterations, have been linked to GH decline. 41 A recent theory to explain the relationship between GH reduction and age-related bone loss has been proposed by Bolamperti et al., 63 who postulate that the amount of fat tissue in bone marrow increases with age, and thus, the osteogenic capacity of the mesenchymal stem cells (MSC) is reduced, due to the low levels of GH. Under normal conditions, an equilibrium between osteogenesis and adipogenesis exists, but it is disrupted when GH secretion declines with age. GH was also shown to activate Wnt signaling, stimulating MSC differentiation toward osteogenesis and inhibiting MSC differentiation toward adipogenesis. Thus, the decline of GH with age could stimulate the expansion of bone marrow fat, contributing to loss of bone mass. 63
Under normal conditions, GH is able to increase the proliferation and differentiation of not only osteoblasts 9 but also osteoclasts, 60 thus stimulating the remodeling process 15,64 and resulting in new bone formation. This leads to the repair of the microdamage that occurs in old bone, which is carried out by the apoptosis 65 of the osteocytes. This is a substantial difference with BPs, which inhibit bone resorption and secondarily bone remodeling. BPs have been shown to be able also to reduce the osteocyte apoptosis; thus, microcracks cannot be repaired and bones become more fragile and more likely to break. 65,66 Moreover, GH has been shown to be able to improve endothelial function and vessel structure when administered to old rats, 67 and even to increase the capillary density in aged rats, 68 whereas BPs have been shown to inhibit microangiogenesis, which has been suggested to be one of the mechanisms underlying the pathogenesis of the necrosis of the jaw. 66
With age, GH and IGF-I could act on the bone diaphysis to facilitate the recruitment of osteoblast to the bone surfaces and to enhance their activity, exerting their effects through the receptors expressed in osteoblasts, osteoclasts, and osteocytes, as reported by Yakar and Isaksson. 54
It has been suggested that GH might also have an anabolic effect on fracture healing, both in young and old animals. 16,17,62 Indeed, it has also been reported that GH administration might be effective in accelerating the consolidation of hip fractures in humans. 69
In contrast, GH has also been shown to be able to increase intestinal calcium absorption, 70 that could be of interest to counteract the secondary hyperparathyroidism present in the elderly, to increase the calcium availability toward the bone, allowing an increase in the mineralization process, even under aging conditions.
Risks of GH use in the elderly
The safety of potential GH supplementation in aged people is controversial. No increase in the risk for cancer has been reported in young patients since 1958, when treatments started. In old patients with GH deficiency, short-term trials have also shown no increase in the risk for cancer, but no data exist for long-term trials. However, since the seminal article of Rudman et al., 47 in the New England Journal of Medicine, many adult and old patients have been treated with GH, mainly in the United States for several indications, including aging itself, and to our knowledge no report about any increase in cancer appearance has been issued until today. Some authors have observed an increased risk for adverse effects, such as carpal tunnel syndrome, fluid retention, or insulin resistance with GH treatment, but only when higher doses of the hormone were used. 19
However, since increased levels of IGF-I have been found in relation to the development of osteosarcoma, 71 despite the positive effects observed with GH treatment on old bones, further studies to address the possible adverse side effects will be necessary to be absolutely sure of its potential therapeutic possibilities.
Conclusion
Within the limitations of this experimental study, systemic GH administration has shown to enhance bone biomechanical properties, BMD, cortical mass, and plasma IGF-I and osteocalcin in old treated rats compared to the control group; consequently, GH could be considered as an alternative therapy against age-related changes in the bone.
Footnotes
Acknowledgments
This article has been possible due to a grant from the Instituto Carlos III (FISS RETICEF RD12/0043/0032) and SAF 2007 66878C02-01. Authors wish to extend their gratitude to Professor Faleh Tamimi, from McGill University, for his expert assistance in biomechanical testing, and to María Teresa García de Juan, for her expert technical assistance in the morphometric analysis.
Disclaimer
None of the authors has any relationship with companies whose product is GH.
Author Disclosure Statement
All the authors have no conflict of interest to declare, including employment relationship or financial interest. All the authors are employed by public Universities of Madrid.
Funding Information
The project was funded by two public grants (Instituto Carlos III, FISS RETICEF RD 12/0043/0032 and SAF 2007 66878C02-01) afforded by the Ministry of Health and the Ministry of Science and Technology. These grants were obtained by a research protocol presentation and due to the research profile of the Professor Jesús A.F. Tresguerres.