
Abstract
The main active metabolite of vitamin D, the 1,25-dihydroxyvitamin D (1,25(OH)2D), and the shed form of the α-Klotho gene (S-Klotho) play an important role in aging-related physiological processes and are currently considered powerful antiaging renal biomarkers. We aimed to investigate the relationship between 1,25(OH)2D and S-Klotho plasma levels in middle-aged sedentary healthy adults. We also aimed to study the mediation role of body composition, physical activity levels, dietary parameters, and blood markers in the association between 1,25(OH)2D and S-Klotho plasma levels. A total of 73 middle-aged sedentary adults (53.4% women; 53.7 ± 5.1 years old) were enrolled in this cross-sectional study. The 1,25(OH)2D plasma levels were measured using a DiaSorin Liaison® immunochemiluminometric analyzer. S-Klotho plasma levels were measured using a solid-phase sandwich enzyme-linked immunosorbent assay. Body composition analysis was performed using dual-energy X-ray absorptiometry scanner. A tendency toward a negative association was observed between 1,25(OH)2D and S-Klotho plasma levels (β = −0.222, R 2 = 0.049, p = 0.059). The association was attenuated after controlling for age and sex and become significant after controlling for fat mass index. In addition, the association between 1,25(OH)2D and S-Klotho levels was indirectly influenced by bone mineral density (BMD), with a percentage of mediation of 31.40%. Our study shows that 1,25(OH)2D is negatively associated with S-Klotho plasma levels in middle-aged sedentary adults, which is partially mediated by BMD.
Clinicaltrial.gov: ID: NCT03334357.
Introduction
Aging is a natural and multifactorial process characterized by a progressive decline of physiological integrity leading to impaired physical and cognitive functions, and increasing the incidence of several age-related diseases (i.e., cardiovascular disorders, osteoporosis, diabetes, cancer, and neurodegenerative diseases, among others). 1 –4 These diseases represent the major cause of morbidity and mortality in developed countries, causing important public health problems and economic burden. 5,6 The discovery of specific antiaging biomarkers, as well as their physiological functions and interactions, have received considerable attention during the last decades aiming to detect therapeutic targets to promote personalized interventions to improve human health and longevity. 7
Recent studies have established the importance of vitamin D status on human health during the aging process beyond its role on specific physiological mechanisms in different organs and systems. 8 Vitamin D alterations have been consistently linked to greater incidence and prevalence of several age-related chronic diseases, impaired physical function, and mortality in different populations. 9 –11 In the kidney, the 25-hidroxyvitamin D undergoes hydroxylation by 25-hydroxyvitamin D-1-α-hydroxylase to form 1,25(OH)2D, which is the main active metabolite and responsible for the majority of functions. 12 Previous studies have reported important antiaging functions of 1,25(OH)2D specifically in bone mineral metabolism, 13 oxidative stress, 14 neurological functions, 15 energy metabolism, 16 and cardiovascular health. 17
In humans, the secreted form of the α-Klotho gene (S-Klotho) has been proposed as an accurate indicator of renal α-Klotho protein expression, 18 an antiaging gene, which extends life expectancy when is overexpressed, and accelerates aging-like phenotypes when is underexpressed. 19 S-Klotho is therefore considered a powerful antiaging biomarker in healthy humans, 20 which could maintain a reciprocal interaction with 1,25(OH)2D. 21 Murine studies 22 –25 have shown that 1,25(OH)2D stimulates the expression of the α-Klotho gene and fibroblast growth factor (FGF) 23, whereas increased levels of S-Klotho and FGF23 inhibit 1-α-hydroxylase leading to the lowering 1,25(OH)2D synthesis and its subsequent degradation. 21 However, to the best of our knowledge, there is no study investigating this relationship in humans.
Understanding the interaction between these two antiaging biomarkers in middle-aged adults is of clinical interest since, it has been previously established that interventions to delay age-related diseases are preferable when individuals are still relatively young and healthy. 2,7 Therefore, the aim of the present study was to investigate the relationship between 1,25(OH)2D and S-Klotho plasma levels in middle-aged sedentary adults. Given that 1,25(OH)2D and S-Klotho plasma levels have been associated with the body composition status in humans, 26,27 we also investigated the mediation role of body composition in the association between 1,25(OH)2D and S-Klotho plasma levels.
Methods
Study design and participants
The participants included in this cross-sectional study were engaged as part of the FIT-AGEING project, an exercise-based randomized controlled trial. The study sample was recruited in Granada (Spain) through electronic media, social networks, and leaflets. Details concerning the inclusion and exclusion criteria can be seen elsewhere. 28 Briefly, a total of seventy-three middle-aged sedentary healthy adults (39 women) between 45 and 65 years of age participated in the current study. They reported to be nonphysically active (i.e., less than 20 minutes of physical activity on less than 3 days/week), to have stable weight (weight changes <3 kg) in the past 12 weeks, to be free of disease, not to be pregnant, to be nonsmoker, and not taking any medication. An extensive medical examination was performed before the beginning of the study.
Design, rationale, and methodology of the study were approved by the Ethics Committee on Human Research of the Regional Government of Andalucía (CEI-Granada) (0838-N-2017) and all participants provided oral and written informed consent in accordance with the last revised ethical guidelines of the Declaration of Helsinki (2013). All baseline assessments were conducted between September and October of 2016/2017 at the Sport and Health University Research Institute (iMUDS, Granada, Spain) and at the “Campus de la Salud” Hospital (Granada, Spain).
Blood sample assessment
Blood samples were obtained from the antecubital vein after overnight fasting and in resting conditions (at least 10 minutes before) in a supine position. All participants were requested (1) to abstain from drugs and/or caffeine, (2) not to do any physical activity at moderate intensity (24 hours before) and/or vigorous intensity (48 hours before), and (3) to eat an established dinner before sampling (i.e., boiled rice and egg omelette with fried tomato sauce). Blood samples were collected in prechilled ethylenediaminetetraacetic acid-containing tubes (Vacutainer, SST, Becton Dickinson, Plymouth, United Kingdom), and were centrifuged at four thousand revolutions per minute for 7 minutes at 4°C and stored at −80°C. The 1,25(OH)2D plasma levels were measured using a DiaSorinLiaison® immunochemiluminometric analyzer (DiaSorin Ltd., Wokingham, Berkshire, United Kingdom) according to the manufacturer's instructions. S-Klotho plasma levels were determined according to a Solid-Phase Sandwich Enzyme-Linked Immunosorbent Assay Kit (Demeditec, Kiel, Germany) strictly following the manufacturer's recommendations. The kit uses two types of highly specific antibodies (i.e., purified mouse anti-human Klotho IgG). The optical density was measured at a wavelength of 450 ± 2 nm and a standard curve was generated using known antigen concentrations.
Anthropometry and body composition
Participants' body weight and body height were measured to the nearest 0.1 kg and 0.1 cm, respectively, with light clothing and without shoes using a prevalidated SECA scale and stadiometer (model 799; Electronic Column Scale, Hamburg, Germany). Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). Body composition analysis was performed using a dual-energy-X-ray absorptiometry scanner ( Discovery Wi, Hologic, Inc., Bedford, MA, USA) with analysis software version APEX 4.0.2, obtaining fat body mass (kg) and lean body mass (kg). A whole-body scan was performed to obtain all parameters following the manufacture's guidelines. The fat mass index (FMI) and the lean mass index (LMI) were calculated as (fat body mass [kg]/height 2 [m]) and (lean body mass [kg]/height 2 [m]), respectively. Bone mineral density (BMD) was calculated as (bone mineral content [g]/total bone surface [cm2]).
Physical activity parameters
Sedentary and physical activity time were objectively assessed by triaxial accelerometry employing a wrist-worn accelerometer (ActiGraph GT3X+, Pensacola, FL, USA) for seven consecutive days (24 h/day). 28 Data were exported and processed using the ActiLife v.6.13.3 software (ActiGraph, Pensacola, FL, USA) and the GGIR package (v.1.5-12) in R software (v.3.1.2). 29,30 The participants who did not wear the accelerometers for at least 16 h/day during 4 days (including 1 weekend day) were finally excluded from the analysis.
Dietary intake
A total of three 24-hour dietary recalls were performed in nonconsecutive days, obtaining two of them on weekdays and one on a weekend day. All 24-hour recalls were conducted through face-to-face interviews by qualified and trained research dietitians. The interviews consisted of a detailed description and assessment of food consumption. A colored photograph guide of different portion sizes of food was used to assist participants in terms of estimating the amount of food they consumed. 31 The dietary data were introduced, analyzed, and processed to obtain energy, macronutrient, and micronutrient content using the EvalFINUT® software (FINUT, Granada, Spain), with the USDA (United States Department of Agriculture) and BEDCA (“Base de Datos Española de Composición de Alimentos”) databases.
Statistical analyses
The present study is based on a secondary analysis using baseline data from the FIT-AGEING project, and therefore a specific power calculation was not developed for the present study. 28 Descriptive data are presented as mean and standard deviation. The distribution of all variables was verified with visual inspection of histograms, Q-Q and box plots, and the Shapiro–Wilk test. Comparisons between men and women were performed with independent samples T test. No interaction by sex was observed (p > 0.05), hence the appropriateness of fitting models for men and women were combined, including sex as a covariable.
Simple linear regression model was first used to examine the association of 1,25(OH)2D with S-Klotho plasma levels. Hierarchical regression analyses were subsequently performed to check whether 1,25(OH)2D predict S-Klotho plasma levels independently of potential confounders. The entry order of potential confounders in the hierarchical analysis were as follows: age, sex, BMI, FMI, LMI, BMD, total energy intake, vitamin D intake, and sedentary and physical activity time. Multiple linear regression analyses were built using the derived confounders.
We analyzed the potential mediating role of body composition, sedentary time, physical activity time, dietary intake, calcium and phosphorus levels in the relationship between 1,25(OH)2D plasma levels, and S-Klotho plasma levels. 32 Mediation was estimated using the indirect effect, which indicates changes in the effect of the independent variable on the outcome that can be endorsed to the proposed mediator. Indirect effects (a × b paths) with confidence intervals (CIs) not including zero are interpreted as statistically significant, 33 which could occur regardless of the significance of the total effect (i.e., c path, effect of the independent variable on the dependent variable) and the direct effect (i.e., c′ path, effect on the dependent variable when both the independent and the mediator variables are included as independent variables). 32 This estimation is based on the bootstrapping method, a nonparametric resampling method, which estimates the indirect effect through 5000 bias-corrected bootstrap samples and 95% CIs. If these CIs do not include zero, the indirect effect ab can be considered as different from this value and therefore the mediation is assumed. To quantify the magnitude of the total effect explained by mediation analysis, we calculated the percentage of mediation ([indirect effect/total effect] × 100) when the total effect was larger than the indirect effect with the same direction. 32
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, v. 22.0, IBM SPSS Statistics, IBM Corporation, Armonk, NY, USA), and p-value <0.05 was deemed significant. The mediation analyses were performed using the PROCESS macro version 3.3 developed by Andrew F. Hayes and the graphical presentations were prepared using GraphPad Prism 5 (GraphPad Software, San Diego, CA, USA).
Results
Table 1 shows the characteristics of the study sample by sex. Plasma levels of 1,25(OH)2D and S-Klotho were 40.3 ± 5.1 and 775.3 ± 363.7 pg/mL, respectively, with no differences between men and women (all p ≥ 0.3). Based on a hierarchical regression model, we included age, sex, and FMI as potential confounders (Table 2).
Descriptive Characteristics of Participants
Data are presented as mean (standard deviation).
Significance differences between sexes (p < 0.05) obtained by independent sample T test.
BMI, body mass index; FMI, fat mass index; LMI, lean mass index.
Hierarchical Regression Between 1,25(OH)2D and S-Klotho Plasma Levels
β, standardized regression coefficient; R 2; and p value were obtained from the hierarchical multiple linear regression analyses.
Simple linear regression analysis showed a weak tendency toward an inverse association between 1,25(OH)2D and S-Klotho plasma levels (β = −0.222, R 2 = 0.049, p = 0.059; Fig. 1). The association was partially attenuated after controlling for age and sex (p = 0.164 and p = 0.074 respectively; Table 3) and become significant after controlling for FMI (p = 0.047; Table 3). However, this association disappeared after controlling for age, sex, and FMI (p > 0.05; Table 3). We also calculated the 1,25(OH)2D/S-Klotho ratio, which was positively associated with age (β = 0.551, R 2 = 0.304, p < 0.001; Supplementary Fig. S1).
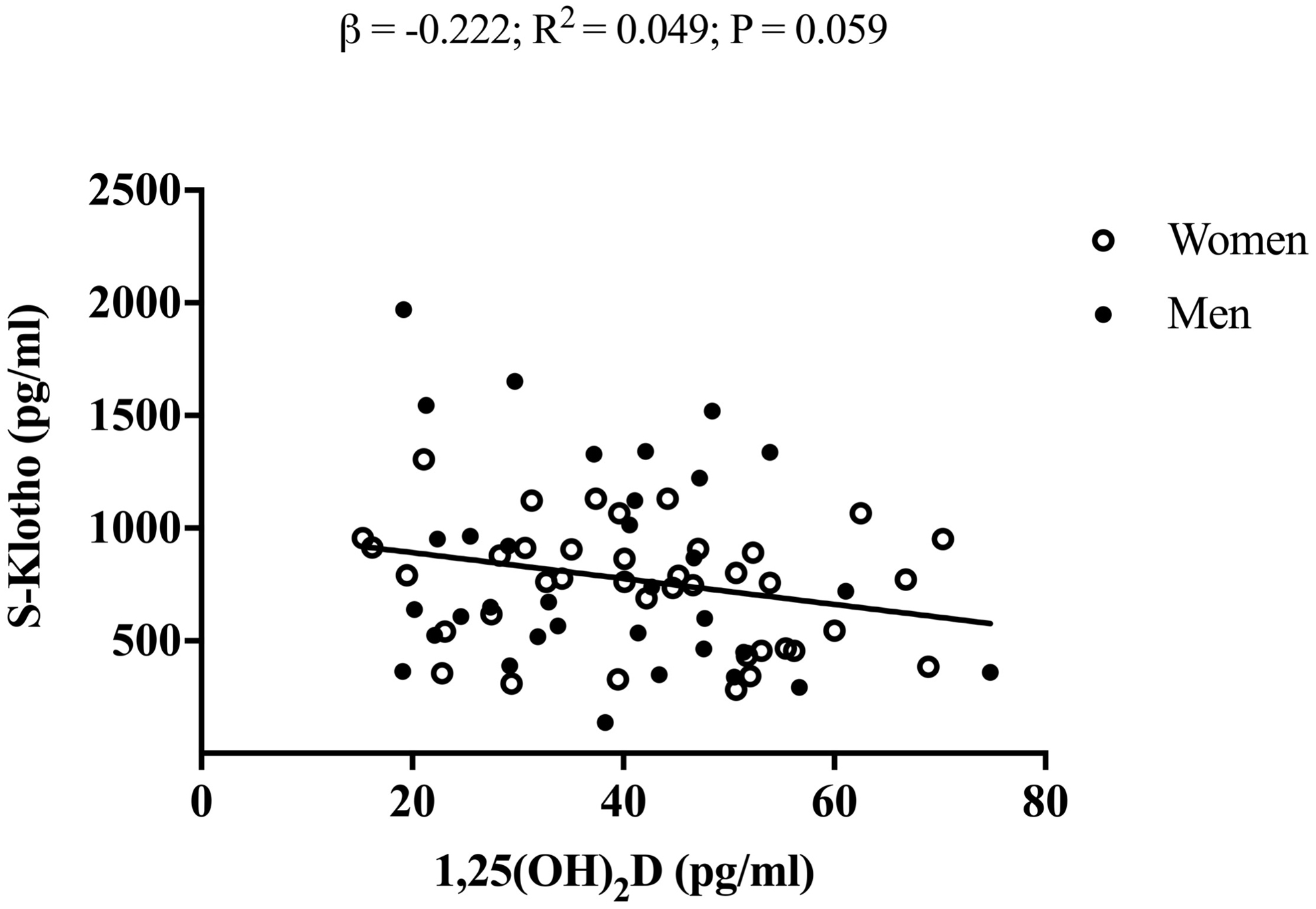
Simple linear regression graph between 1,25(OH)2D and S-Klotho plasma levels in middle-aged sedentary adults. β, standardized regression coefficient, R 2, and p from a simple linear regression analysis. 1,25(OH)2D, 1,25-Dihydroxyvitamin D.
Multiple Linear Regression Analyses Indicating the Association of 1,25-Dihydroxyvitamin D with S-Klotho Plasma Levels
The analyses were controlled for: age (Model 1); sex (Model 2); FMI (Model 3); age, sex, and FMI (Model 4). β, standardized regression coefficient; R 2 and p value were obtained from the multiple linear regression analyses.
Simple mediation analyses were carried out to test whether the association of 1,25(OH)2D with S-Klotho plasma levels could be mediated by body composition, sedentary and physical activity time, dietary intake, and calcium and phosphorus levels. We observed an inverse association of BMD and S-Klotho levels (b path p = 0.015; Fig. 2). There was a significant indirect effect (path ab) between 1,25(OH)2D and S-Klotho levels when BMD was included as a mediator outcome (Fig. 2). The association between 1,25(OH)2D and S-Klotho levels was indirectly influenced by BMD, with a percentage of mediation of 31.40%. Mediation analyses were not significant when other body composition parameters, sedentary and physical activity time, dietary intake, and calcium and phosphorus levels were included as mediator variables (Supplementary Table S1).
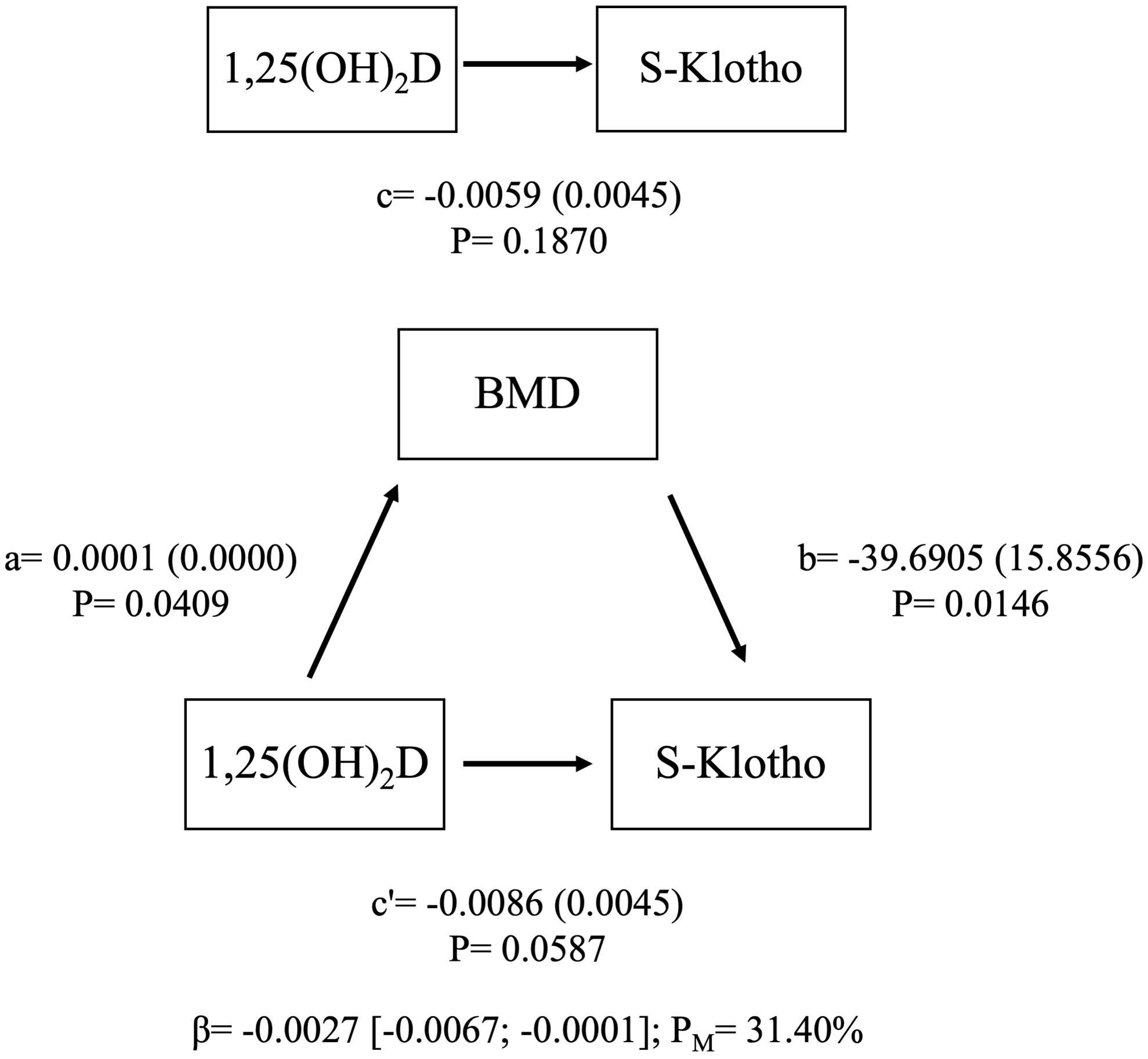
Mediation model of the relationship between 1,25(OH)2D and S-Klotho plasma levels in bone mineral density as a mediator variable. Paths a, b, c, and c′ are presented as unstandardized coefficients (SE). β = indirect effect (a × b paths) [lower-limit CI; upper-limit CI], lower and upper levels for bias-corrected 95% CIs of the indirect effect based on 5000 bootstraps. BMD, bone mineral density; CI, confidence interval; SE, standard error.
Discussion
Our study sought to elucidate the potential association of 1,25(OH)2D with S-Klotho plasma levels and, in turn, whether body composition parameters, physical activity levels, dietary parameters, and blood markers were potential mediating mechanisms explaining the closed association between 1,25(OH)2D and S-Klotho in middle-aged sedentary adults. The present results suggest that 1,25(OH)2D is slightly inversely associated with S-Klotho, with this association being increased after adjusting by FMI, and attenuated after adjusting by age and sex. Interestingly, BMD significantly explained the association between these two variables. To the best of our knowledge, this is the first study that elucidates an inverse relationship between 1,25(OH)2D and S-Klotho plasma levels in humans.
Both 1,25(OH)2D and S-Klotho have emerged as important hormones related to the promotion of health span by delaying chronic diseases. 34 Indeed, previous studies have suggested that 1,25(OH)2D and S-Klotho could function in a closed endocrine loop involving several physiological and molecular pathways that may lead to increase health span and prevent chronic diseases. 34 The relationship between 1,25(OH)2D and Klotho has been previously investigated in mice 22 –25 showing that a downregulation of α-Klotho gene expression induces an overexpression of 1α-hydroxylase. This fact was explained by an absence of the inhibitory effect of FGF23 signaling on renal 1α-hydroxylase (CYP27B1) expression, 25 leading to higher production of 1,25(OH)2D, 20,35 which produces subsequent mineral and hormone imbalances related to premature aging syndrome. 36 On the other hand, a recent clinical trial conducted by Azimzadeh et al. showed that 12 weeks of 50.000 IU Vitamin D3 (cholecalciferol) supplementation prevents the reduction of S-Klotho plasma levels inherent to the aging process in older population. 37 Furthermore, this study also observed an increment of 25-hydroxyvitamin D levels after the supplementation. However, the 1,25(OH)2D plasma levels were not determined, 37 therefore, it is unknown if changes in 1,25(OH)2D levels occurred. The slightly inverse association between 1,25(OH)2D and S-Klotho plasma levels in our study concurs with those observed in mice models, and could be explained by an inhibitory feedback loop between both metabolites. Higher levels of 1,25(OH)2D could increase S-Klotho plasma levels downregulating 1,25(OH)2D plasma levels in a negative feedback loop. 34,38 Similarly, low levels of S-Klotho could increase the activity of 1α-hydroxylase subsequently increasing 1,25(OH)2D levels. 20,25,35 S-Klotho decrease upon age, inhibiting FGF23 signaling of 1,25(OH)2D inactivation in kidney, being subsequently upregulated. 38 Therefore, since we observed that 1,25(OH)2D/S-Klotho ratio was positive associated with age, it could be a plausible biomarker of age.
Our results suggest a mediation role of BMD in the relationship between 1,25(OH)2D and S-Klotho plasma levels. FGF23 is mainly produced in bone by osteoblasts and osteocytes in response to elevated 1,25(OH)2D 39 functioning as an auto-/paracrine inhibitor of bone mineralization by suppressing alkaline phosphatase. 40 In this sense, high FGF23 levels have been associated with an impaired trabecular bone microarchitecture in osteoporosis, 41 low BMD in childhood, 42 and biomarkers of vertebral fractures in elderly. 43 It seems therefore plausible that the mediation role of the BMD may be explained by FGF23 plasma levels, suggesting the presence of an endocrine bone/kidney axis in humans, where 25(OH)D, 1,25(OH)2D, FGF23, and S-Klotho are involved 38,39 (Fig. 3): (1) 1,25(OH)2D would increase intestinal calcium and phosphorus absorption and bone deposition ensuring an adequate BMD status, 44 and in a negative feedback loop, it would be suppressed by the restoration of a normal range of calcium and BMD 44 ; (2) 1,25(OH)2D would promote FGF23 secretion and, in a negative feedback loop, 1,25(OH)2D would be suppressed by FGF23. 39 FGF23 also downregulates the synthesis of 1α-hydroxylase in the renal proximal tubules, thus suppressing 1,25(OH)2D production 39 ; (3) 1,25(OH)2D increases S-Klotho plasma levels and, in a negative feedback loop, 1,25(OH)2D would be suppressed by S-Klotho. 34,38 Furthermore, 1,25(OH)2D is part of the structural basis of the FGF23-α-Klotho-FGFR1c complex formation, which triggers into increased levels of S-Klotho 38 ; (4) FGF23 is released by bone cells 39 and is associated with a poor bone status. 41 –43 This fact could be explained by the suppression of 1,25(OH)2D. Similarly, given that FGF23 took part in the structural basis of the FGF23-α-Klotho-FGFR1c complex formation, it may lead to an increased release of S-Klotho into circulation 38 ; (5) S-Klotho is associated with higher BMD in middle-aged adults. 27
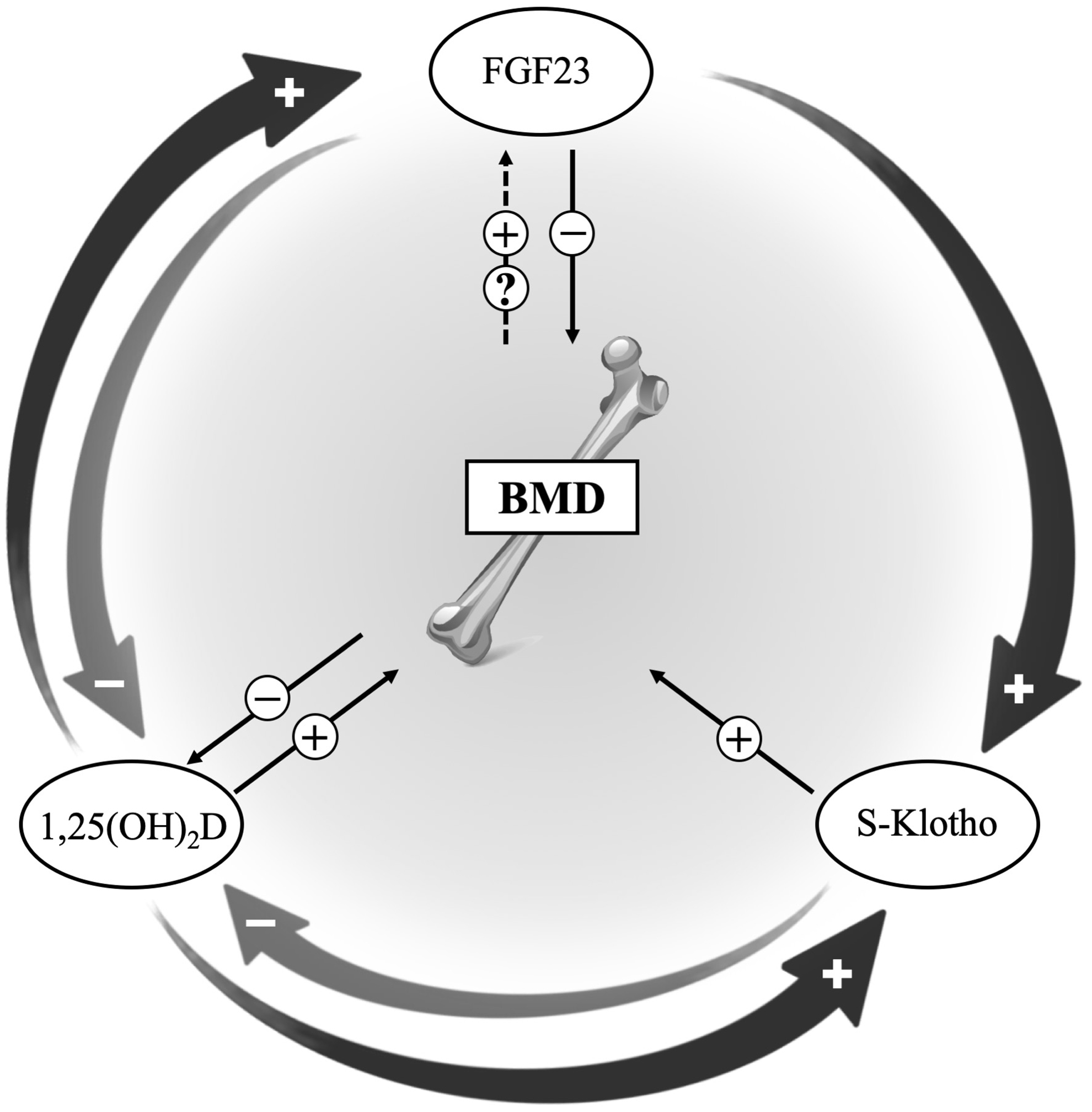
1,25(OH)2D-bone mineral density-S-Klotho axis. BMD, bone mineral density; FGF23, fibroblast growth factor 23.
Taking all together, our results suggest that BMD is closely related to the FGF-Klotho endocrine system, which has been identified as a key factor in the pathophysiology of age-related disorders. 38 Our results have a marked clinical implication, since the disruption of the FGF23-αKlotho endocrine axis has an important role in the pathophysiology of renal and bone disorders. 38 Future studies investigating the influence of different interventions in the whole FGF23-αKlotho endocrine axis, where BMD is taken into account are needed.
Limitations
The limitations of the present study include a cross-sectional design, which means that no causal relationships can be established. Our participants were middle-aged sedentary adults (45–65 years old), so we cannot extrapolate these findings to older, younger, and/or physically active individuals. We did not have data of FGF23 and 25-hydroxyvitamin D plasma levels, which would be desirable to understand our study findings well. Lastly, since the sample size of this study is relatively small, data should be interpreted with caution.
Conclusions
In summary, our results suggest that 1,25(OH)2D is negatively associated with S-Klotho plasma levels in middle-aged sedentary adults, which is partially mediated by BMD. Therefore, we suggest that BMD should be taken into account in future studies investigating the relationship of 1,25(OH)2D with S-Klotho plasma levels. Future studies are therefore needed to elucidate whether changes in 1,25(OH)2D and/or BMD are related to changes in S-Klotho plasma levels after different antiaging interventions (i.e., vitamin D supplementation, exercise, and/or dietary interventions).
Footnotes
Acknowledgments
The authors would like to thank all the participants who took part in the study, and for their time and effort. This study is part of a PhD thesis conducted in the Official Doctoral Program in Biomedicine of the University of Granada, Spain.
Author Contributions
Study design: A.D.-L.-O., L.J.F., M.J.C., A.G., and F.J.A.-G. Study conduct: A.D.-L.-O., L.J.F., M.J.C., A.G., and F.J.A.-G. Data collection: A.D.-L.-O., L.J.F., and F.J.A.G. Data analysis: A.D.-L.-O., L.J.F., and F.J.A.-G. Data interpretation: A.D.-L.-O., L.J.F., M.J.C., A.G., and F.J.A.-G. Drafting article: A.D.-L.-O., L.J.F., and F.J.A.G. Revising article content: A.D.-L.-O., L.J.F., M.J.C., A.G., and F.J.A.-G. All authors approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study is supported by the Spanish Ministry of Education (FPU14/04172 and FPU15/03960).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.