
Abstract
Idiopathic pulmonary fibrosis (IPF) is a chronic debilitating fibrotic lung disease leading to respiratory failure and ultimately to death. Noninvasive biomarkers, for the early diagnosis, differential diagnosis, prognosis, and prediction of therapeutic response, are needed. Previous studies support a role for periostin in lung fibrosis. The aim of our study was to analyze periostin levels in the airways of patients with IPF and to investigate its role as a useful predictive biomarker of the disease. We enrolled 30 IPF patients and 5 control subjects. All subjects underwent all standard radiological, functional, and biological examinations for IPF diagnosis and staging and exhaled breath condensate (EBC) collection. Periostin was assessed by an enzyme-linked immunosorbent assay kit on EBC. Periostin was dosable in the EBC of all subjects enrolled. We found higher exhaled periostin levels in IPF patients than healthy controls (65.5 ± 23.5 pg/mL vs. 33 ± 21.4 pg/mL, p < 0.05). Moreover, in receiver operating characteristic analysis, the clinical reference value of periostin was 37.88 pg/mL to discriminate patients with IPF from healthy subjects, with the area under the curve of 0.8815. There was no significant correlation between periostin levels and gender or pulmonary function tests. These preliminary results support our working hypothesis that periostin is dosable in the airways of patients with IPF. As the circulating periostin, also airways periostin may be a potential biomarker to support IPF diagnosis and to monitor disease progression during follow-up.
Introduction
Periostin is highly expressed in the lungs and detected in the circulation of patients with idiopathic pulmonary fibrosis (IPF). 1,2 It is highly expressed at sites of injury or inflammation and promotes mesenchymal cell proliferation and fibrosis, and plasma levels of periostin at baseline predict clinical progression in patients with IPF. 2 Different studies have proved the possibility to use the periostin as a biomarker. Okamoto et al. found significant high levels of periostin in the serum of IPF patients compared with control subjects or patients with other idiopathic interstitial pneumonias (IIPs), showing a negative correlation between periostin levels and pulmonary function in patients with IPF. Therefore, periostin could be used to distinguish IIPs with fibrosis. 1 A study using a mouse model highlighted the eventual therapeutic role of periostin in IPF, demonstrating that it promotes the process of pulmonary fibrosis. 3
Other studies have also shown that serum levels of periostin are associated with IPF clinical progression. 4,5 Augmentation in periostin serum levels and the extent of the radiological fibrotic area were associated; moreover, the same study demonstrated that serum periostin level was a useful prognostic biomarker for predicting long-term outcome in terms of the survival time in patients with IPF. 4
Periostin is produced in response to transforming growth factor-beta (TGF-β) and interleukin-13 (IL-13), a fibrogenic cytokine highly expressed in IPF lung tissue and found to be involved in the development/progression of IPF. 6,7 In fibroblastic foci, the expression of periostin was significantly high, suggesting that fibroblasts, mainly myofibroblasts, produce periostin in IPF patients. 1,2,8,9
Nonetheless, although periostin has been considered as playing a role in the pathogenesis of pulmonary fibrosis, periostin blood levels have been already validated in the literature, whereas none studied the presence of this protein locally, in the airways, supporting a potentiality of periostin as an organ-specific marker of lung fibrosis.
Recently our group analyzed periostin concentration in the exhaled breath condensate (EBC) of asthmatic subjects, demonstrating the suitability of that type of sample for periostin analysis. 10
The EBC is a sample coming from airways, collected in a completely noninvasive way, asking patients to breathe at tidal volume in a mouthpiece valve collected with a condenser for 10 minutes. 11 The method allows to collect the airway lining fluid to analyze the physiologic and pathologic processes in the lung. 12 The noninvasiveness and simplicity of the technique are well accepted by affected patients, often frustrated by several examinations that they usually undergo and by their daily symptom burden. Furthermore, we believe the research of biomarkers in the target organ would offer more interesting information to better understand the pathogenesis of the disease. 13
The aim of this study was to study the periostin concentrations in the EBC from patients with IPF, analyzing the potentiality of this noninvasive biomarker in the management of those patients.
Materials and Methods
Population
Thirty patients with IPF (24 men, age 66.3 ± 1.2 years) and 5 healthy controls (3 men, 60.7 ± 3.4 years) were enrolled in the accredited outpatient pulmonary clinic for lung fibrosis of the Institute of Respiratory Diseases of the University of Foggia (Table 1). IPF was diagnosed according to the criteria of American Thoracic Society/European Respiratory Society/Japanese Respiratory Society/Latin American Thoracic Society statement for IPF after evaluation of all clinical, laboratory, functional, imaging, and histological data. 14 All patients were treatment naive. Furthermore, all patients underwent EBC for periostin analysis. This study was conducted in accordance with the amended Declaration of Helsinki. Written informed consent was obtained from all subjects, and the study was approved by our institutional ethics committee of Foggia.
General Characteristics of Patients with Idiopathic Pulmonary Fibrosis and Controls
p < 0.01 IPF versus controls.
p < 0.05 between IPF and controls.
DLCO, carbon monoxide diffusing capacity; IPF, idiopathic pulmonary fibrosis; L, C units; ND, not determined; VC, vital capacity.
Pulmonary function test
Pulmonary function tests were performed. Forced expiratory volume in 1 second, forced vital capacity, and carbon monoxide diffusing capacity were measured using a spirometer (Sensormedics, USA). The best value of three maneuvers was expressed as a percentage of the predicted normal value.
EBC and processing
One milliliter of EBC was collected in one setting from each patient at the time of diagnosis, by using a condenser, which allowed for the noninvasive collection of nongaseous components of the expiratory air (EcoScreen Jaeger, Wurzburg, Germany). The condensate was collected on ice at −20°C, transferred to 1.5 mL polypropylene tubes, and immediately stored at −80°C for subsequent analysis. We used the condensate within 1 month from the time it was stored.
Periostin analysis
Initially, a proprietary sandwich enzyme-linked immunosorbent assay (Human Periostin ELISA Kit; Thermo-Fisher Scientific) was used to determine periostin levels in undiluted samples of EBC. The intra-assay variability was <10% and the interassay variability was <12%, with a detection limit of 0.08 ng/mL. As we achieved unexpected results, below the detection limit, we chose to measure periostin levels in undiluted samples of EBC using a specific enzyme immunoassay kit (DuoSet ELISA; R&D Systems) according to the manufacturer's recommendations because this is a more sensitive assay. Before the test, the EBC was concentrated with Microcon-30 kDa Centrifugal Filter Unit with Ultracel-30 membrane (Merk Millipore) and then analyzed together with nonconcentrated EBC samples. We carried out several experiments with both EBC samples (concentrated and not), and then we compared the results. Our results showed no significant difference in the concentrations of periostin; therefore, we decided to use the unprocessed EBC samples for the next test.
Statistical analysis
Descriptive statistics (i.e., means, standard deviations, and percentages) were applied to summarize the continuous and categorical variables.
We performed a t-test to assess the difference of periostin levels in the EBC of IPF patients and control group. The relationship between two continuous variables was determined by measuring the Pearsons correlation coefficient. Correlations between the two groups were evaluated by Spearman's rank correlation coefficient.
Receiver operating characteristic (ROC) curves were used to examine the usefulness of exhaled periostin concentrations in discriminating patients with IPF from healthy controls. The Kaplan–Meier method was used to estimate the probability of survival as a function of time, and survival differences were analyzed using the log rank test. A p-value <0.05 was considered significant. These evaluations were performed using statistical software (Statistica version 8.0; StatSoft, Inc., 2007, USA) that was used to analyze the data.
Results
Demographic, clinical, and functional data of patients affected by IPF and healthy controls enrolled in the study are reported in Table 1.
Periostin was dosable in the EBC of all subjects enrolled. We found a significantly higher exhaled periostin in IPF patients than in healthy controls (65.5 ± 23.5 pg/mL vs. 33 ± 21.4 pg/mL, p < 0.05) (Fig. 1). There was no significant correlation between periostin levels, pulmonary function tests, oxygen saturation, exertion tolerance, and anthropometric data.

Periostin levels in the EBC of IPF patients and healthy controls. Patients with IPF showed a higher level of EBC periostin (65.5 ± 23.5 pg/mL vs. 33 ± 21.4 pg/mL, p < 0.05). EBC, exhaled breath condensate; IPF, idiopathic pulmonary fibrosis.
ROC analysis of the IPF cohort revealed that an EBC periostin concentration of 37.88 pg/mL can be reliably used to discriminate subjects with IPF (>37.88 pg/mL) from healthy controls (≤37.88 pg/mL), with a sensitivity of 96.3% and specificity of 80.0% (area under the curve: 0.8815, p = 0.007) (Fig. 2; Table 2).
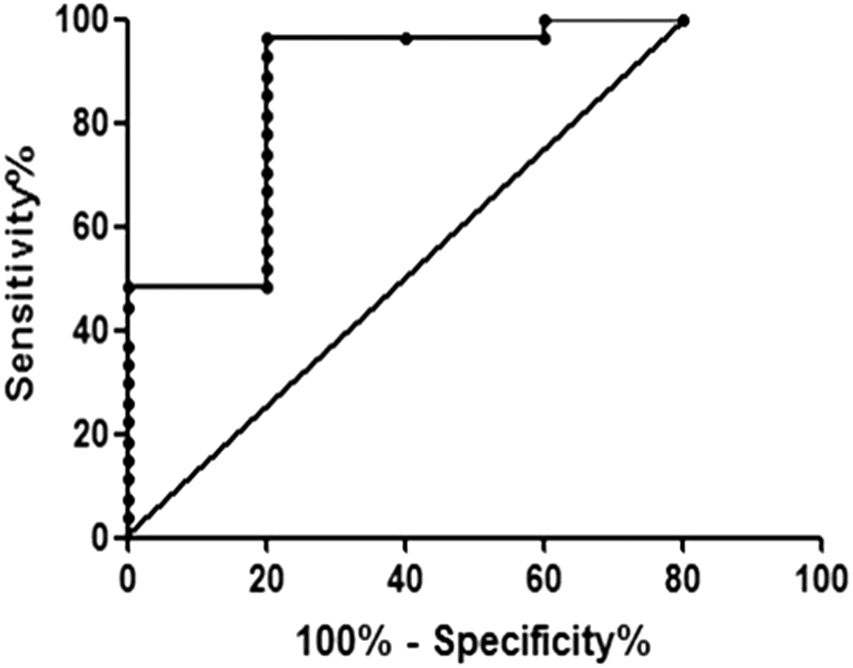
Receiver operating characteristic curve of the IPF cohort used to separate IPF from healthy subjects according to EBC periostin levels (cutoff 37.88 pg/mL).
Receiver Operating Characteristic Curve Analysis Used to Discriminate Subjects with Idiopathic Pulmonary Fibrosis from Healthy Controls
AUC, area under the curve; CI, confidence interval.
To investigate the prognostic effect of EBC periostin level, we divided the patients into two subgroups by the median value of EBC periostin content (60.75) and estimated the association between this marker and the overall survival of IPF patients (Fig. 3). Patients' survival was calculated as the interval between the date of diagnosis and date of death or date of the last follow-up visit, and accounted for the most important clinical endpoint. The results of this analysis indicate that periostin levels in the EBC were not significantly associated with unfavorable prognostic value (Table 3).

Kaplan–Meier curve of the overall survival analyses in EBC of IPF patients. The curve indicated that patients with EBC periostin levels higher than 60.75 showed higher mortality than others. Color images are available online.
Survival Analysis (χ2 and p-Value for Log Rank Test) for Periostin Content
EBC, exhaled breath condensate.
Discussion
In this study, we demonstrated that periostin is detectable in EBC and that its concentrations present significant differences between patients with IPF and healthy control subjects.
Moreover, further evidence supporting the finding of elevated periostin concentrations in IPF was provided by ROC curve analysis, which showed that EBC periostin concentrations could discriminate between healthy controls and IPF patients.
Next, we investigated the effect of airway periostin levels on survival of IPF patients. Although IPF patients with high periostin concentration seem to have a higher mortality rate than patients with low levels of periostin, the significance is not reached. The data showed that EBC periostin concentrations were not associated with overall survival.
Previous studies showed that periostin is highly expressed in the lungs and is found at increased levels in the circulation of patients with IPF, these levels are probably associated with a decrease in lung function, suggesting the likely prognostic value of this biomarker. 1,2
Our results agree with these observations; moreover, we have shown that it is possible to measure the periostin in the airways of IPF patients. It has been indicated that periostin is strongly expressed in fibrotic foci areas relevant for evaluating the prognosis of IPF, and this finding supports the use of periostin as a biomarker. 15 Periostin also seems to be a reliable biomarker for disease activity independently from age. Walsh et al. described stable levels of periostin from age 32 to >70 years. 16
Several studies confirmed the profibrotic role of periostin suggested in our study. Preliminarily, we expected an increase of periostin in IPF patients as well as that of other profibrotic mediators such as TGF-β 17 and IL-13. 6 The profibrotic role of periostin is probably more recognized compared with those markers, as the periostin plays an important role in helping to stiffen the lung pulmonary extracellular matrix (ECM). Lysyl oxidase is an extracellular enzyme that catalyzes the cross-linking between collagen fibrils. Periostin interacting with bone morphogenetic protein-1 induces the proteolytic activation of lysyl oxidase, causing an increase of collagen cross-linking that leads to stiffening of the ECM. This increase in the stiffness of the ECM is believed to promote ongoing fibroblast activation, which may perpetuate the progressive nature of IPF. 18,19 As the diagnosis of IPF is complex and mainly based on invasive procedures, there is a need to identify reliable biological markers that noninvasively can foster a confident diagnosis of IPF. 20,21
In this study, for the first time to our knowledge, we measured periostin levels in the airways (EBC) of IPF patients. EBC is completely noninvasive and safe, and this approach becomes very important when the subjects studied are patients with IPF, frustrated for numerous diagnostic tests that they must undergo for diagnostic and follow-up purposes and, moreover, they soon develop early respiratory failure, and they are unable to perform the most common tests required. Thus, we believe that the use of non-invasive samples such as EBC for the research of biomarkers of disease could be very useful for the diagnosis and monitoring of these type of patients.
Our findings show the possibility to measure periostin concentrations in EBC by a commercially available ELISA kit.
Cameli et al. have stated that alveolar nitric oxide levels were significantly higher in IPF patients and correlated with serum periostin levels. 22 In our study, we did not correlate EBC periostin levels with exhaled NO but we aim to overcome this lack with a future study, to better understand whether there is a common pathway between the biomarkers.
This study presents some limitations. The main limit of this study is the small number of subjects enrolled in each group. Nevertheless, this is a preliminary pilot study that will be followed by a larger study. Another important limitation is the measurement of periostin only in EBC samples not in serum samples.
Conclusions
In conclusion, these results support our working hypothesis that periostin is dosable in the airways of patients with IPF. As the circulating one, airways periostin may be a potential noninvasive biomarker to support IPF management in clinical practice.
Footnotes
Authors' Contributions
G.E.C., P.S., and D.L. designed the study; G.E.C., P.S., G.S., and G.P.P. contributed to the clinical and laboratory work for the study; G.E.C., P.S., and D.L. drafted the article and revised it critically for important intellectual content; G.E.C., D.L., and M.P.F.B. contributed to final approval of the version to be published. All authors read and approved the final article.
Authors' Agreement
The authors have seen and approved the final version of the article. The authors warrant that the article is an original work, has not received prior publication, and is not under consideration for publication elsewhere.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the amended Declaration of Helsinki and the study was approved by the institutional ethics committee of the University of Foggia (institutional review board approval number 17/CE/2014).
Consent for Publication
Informed consent was obtained from all individual participants included in the study.
Availability of Data and Materials
Source data and material will be made available upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.