
Abstract
Heart failure with reduced ejection fraction (HFrEF) is associated with reduced cardiac function and impaired quality of life. Blood flow restriction (BFR) training is emerging as a potential adjunctive therapy. This study aimed at evaluating the efficacy of combination of BFR and isometric exercises on cardiac function, functional status, and quality of life in HFrEF patients. Totally 44 patients with HFrEF were equally divided into a control group and a combined treatment group. Both groups received standard pharmacotherapy and upper limb exercise, with the combined group also undergoing BFR and isometric exercise training. We assessed demographic and clinical characteristics, New York Heart Association (NYHA) functional classification, cardiac function parameters, serum Brain Natriuretic Peptide levels, physical capacity via the 6-minute walking test, and quality of life using the Heart Failure Questionnaire (Minnesota Living with Heart Failure Questionnaire). Post-treatment, the combined group significantly improved in NYHA classification (p = 0.012), with more patients shifting to a better class. Cardiac function improved in both groups, with the combined group showing a greater increase in mean left ventricular ejection fractions (p < 0.001), and reductions in left ventricular end-diastolic and end-systolic diameters (p < 0.05). The addition of BFR training to standard pharmacotherapy with upper limb exercise in HFrEF patients led to significant enhancements in cardiac function, functional status, and quality of life. These findings support the integration of BFR training into conventional HFrEF treatment regimens to maximize patient recovery outcomes.
Introduction
Chronic heart failure (CHF), a widespread and complex condition, manifests due to the heart's diminished capacity to pump blood, evidenced by structural or functional anomalies and symptoms such as shortness of breath, fatigue, and swelling. 1 Diagnosing this persistent syndrome entails a careful assessment incorporating patient history, physical signs, and investigative tests, since it often presents subtly and is complicated by non-specific symptoms or concurrent health issues.
CHF often diagnosed based on clinical signs of left ventricular dysfunction, carries a grim prognosis, with up to 17% of patients dying during their initial hospital stay and more than half within 5 years. 2 Left heart failure is increasingly prevalent, encompassing conditions such as heart failure with preserved ejection fraction (HFpEF) where the ejection fraction is above 50%, heart failure with reduced ejection fraction (HFrEF) characterized by an ejection fraction of less than 40%. Around half of all heart failure patients are diagnosed with HFrEF, a condition that is increasingly being identified over time. In contrast, HFpEF, unlike HFrEF, is predominantly found in women (79% compared with 49%) and generally occurs in an older population. 3 –5
However, heart failure syndrome presents a small fraction of diagnosed cases visible within community care and cardiology, whereas a significant number of undetected cases and individuals with asymptomatic left ventricular dysfunction, who are susceptible to developing heart failure, remain hidden; accurate detection spans across systolic and diastolic dysfunctions, requiring detailed echocardiographic evaluation for proper diagnosis, 6 In addition, this high mortality and morbidity rate, including frequent hospital readmissions, underscores the urgent need for a deeper exploration of the underlying pathophysiological processes.
CHF patients often present with dyspnea and fatigue, with a significant reduction in activity tolerance. 7 Cardiac rehabilitation for this group necessitates judicious exercise selection to mitigate the risk of acute cardiac events and maximum the possibility to reduce mortality. 8 While high-intensity exercises might optimize cardiac conditioning, they also augment the cardiac workload, raising the risk of acute heart failure events, particularly during intense training sessions. 9 –11
There are several methods of exercise rehabilitation training for patients with HFrEF: aerobic training, resistance training, inspiratory muscle training, and neuromuscular electrical stimulation. 7,11,12 Isometric exercise training, characterized by static contractions against resistance without joint movement, has been historically underutilized in cardiac rehabilitation due to concerns over additional cardiac stress. 13 It has indicated that isometric exercises could be safely executed, even in a supine position, without significantly increasing heart rate or oxygen demand, thereby offering a safe and effective rehabilitation option. 14
Blood flow restriction (BFR), which strategically reduces arterial inflow and venous outflow during exercise, 15,16 has garnered international attention as a rehabilitative measure, especially after musculoskeletal injuries, to prevent muscle atrophy and enhance strength and endurance. 17 Since BFR increase showed the ability to increase skeletal muscle strength and hypertrophy for individuals, 18 we proposed that the combination of BFR with isometric exercise in HFrEF patients may have the potential to boost collateral circulation, enhance myocardial blood flow, and provide cardioprotective effects that may delay myocardial remodeling and improve cardiac function and perfusion.
Thus, this study seeks to explore the combination of BFR and isometric exercises as a therapeutic approach for patients with HFrEF, aiming at contributing to the growing body of literature on effective cardiac rehabilitation interventions and at providing evidence-based enhancements to current treatment paradigms.
Methods
Participants
Individuals admitted with HFrEF at Chuzhou First People's Hospital were enrolled. The study was approved by Chuzhou First People's Hospital (approval no.: 2021xkj201). Informed written consent was derived from the participants. The study flow was shown in Figure 1. Participants included those with a confirmed diagnosis of HFrEF, categorized between New York Heart Association (NYHA) functional classes II to IV, having left ventricular ejection fractions (LVEF) below 45%, and no episodes of acute myocardial infarction within the preceding 6 months.
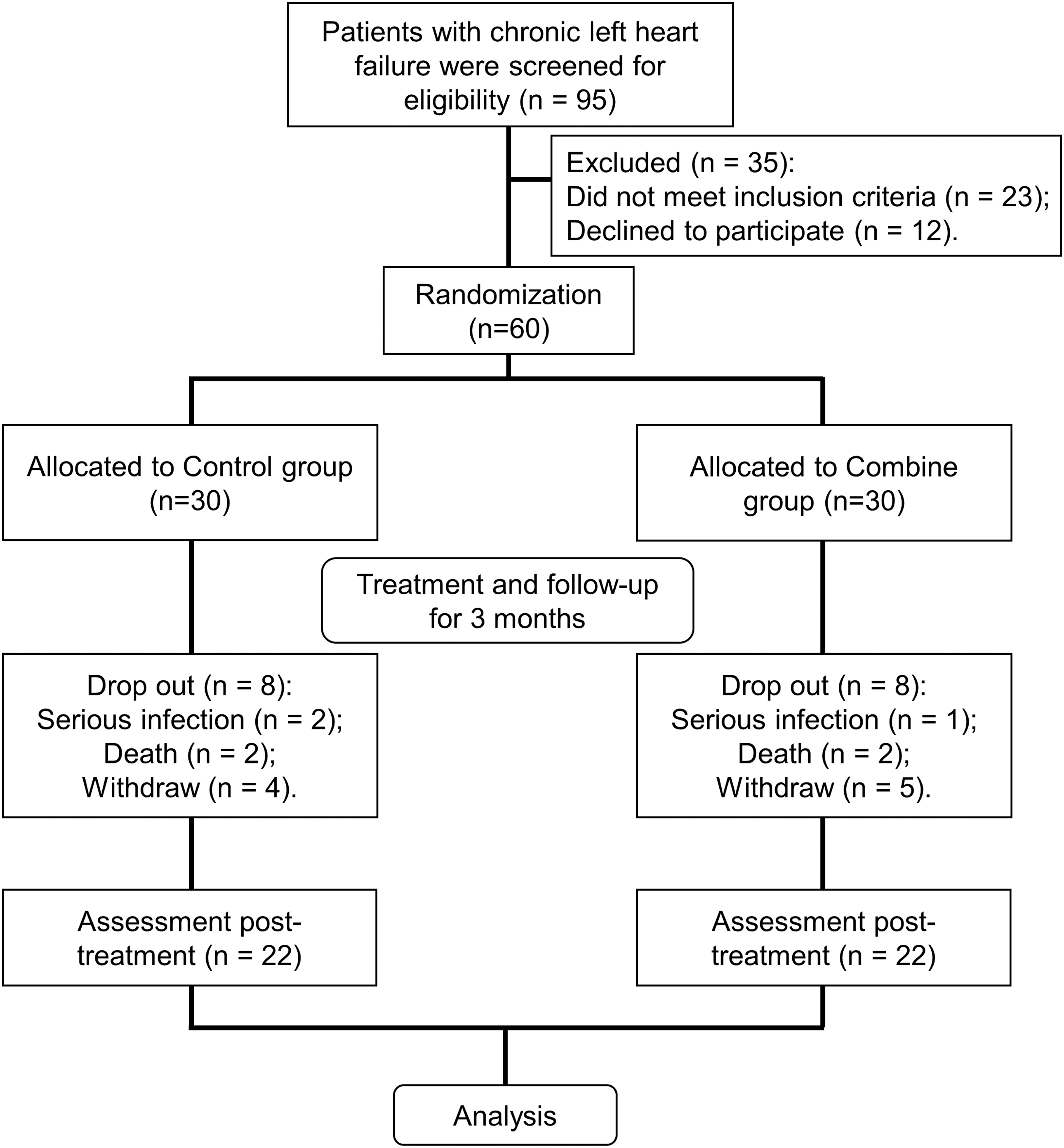
Study flow. A total of 95 patients were screened for eligibility, with 35 excluded due to not meeting inclusion criteria (n = 23) or declining to participate (n = 12). Sixty patients were randomized into two groups: 30 to the control group and 30 to the combined treatment group. Both groups underwent a treatment and follow-up period of 3 months. In each group, 8 patients dropped out due to serious health events (control group: n = 2; combined group: n = 1), death (control group: n = 2; combined group: n = 1), or withdrawal (control group: n = 4; combined group: n = 5). This left 22 participants in each group who completed the post-treatment assessment and were included in the final analysis.
Patients with unstable angina, uncontrolled arrhythmias, significant symptomatic aortic or mitral valve stenosis, hypertrophic obstructive cardiomyopathy, severe pulmonary hypertension, resting systolic blood pressure >200 mmHg or diastolic >110 mmHg, acute myocarditis or pericarditis, thrombophlebitis, systemic or pulmonary embolism, neuromuscular disorders, or severe proximal limb skin diseases or injuries were excluded.
Interventions
The control group underwent isometric contractions of the limbs in addition to standard pharmacotherapy, using handgrip exercises at 40%–50% of their maximum strength, 5 days a week for 3 months. The observational group received the same pharmacotherapy with upper limb exercise and performed limb isometric contractions with BFR, applying a tourniquet at 80% occlusion pressure at the distal upper limbs. A hand grip exercise involves squeezing a handheld device or object with hand, specifically targeting the muscles in forearm, hand, and fingers. This exercise is commonly used in rehabilitation, sports training, and general fitness routines.
Blood flow occlusion pressure measurement
Patients lie in a supine position while an occlusion cuff is fitted to the upper limb. Radial artery pulsation was located, and a Doppler ultrasound was used to detect the disappearance of the pulse sound, determining the occlusion pressure. Training began within 5 minutes of applying pressure at 40%–50% of the patient's maximum grip strength, with a breathing pattern of 2-second exhalation and 4-second slow inhalation, repeating for 50 cycles over 5 minutes.
Assessments
A 6-minute walking test (6MWT) was conducted 2 hours post-meal, following guidelines from the American Thoracic Society. Serum Brain Natriuretic Peptide (BNP) levels were measured using a chemiluminescent immunoassay before and after treatment. The Minnesota Living with Heart Failure Questionnaire (MLHFQ), encompassing 21 items on physical, social, emotional, and economic aspects, were used to assess life quality. Echocardiography was performed using a Philips ultrasound device to measure LVEF, early (E) and late (A) diastolic mitral valve flow velocities, and the ratio of these velocities (E/A), along with left ventricular end-diastolic diameter (LVEDd) and left ventricular end-systolic diameter (LVESd).
Statistical analysis
In this study, 95 patients with HFrEF were initially screened for eligibility. Of these, 35 were excluded: 23 did not meet the inclusion criteria, and 12 declined to participate. The remaining 60 patients were randomized into two groups, with 30 patients allocated to the control group and another 30 to the combined intervention group. Both groups underwent their respective treatments and were followed up for a period of 3 months.
During the follow-up, each group experienced dropouts: eight from the control group (two due to serious infection, two deaths, and four withdrawals) and eight from the combined group (one due to serious infection, two deaths, and five withdrawals). Post-treatment assessments were completed for 22 patients in each group, and the collected data were included in the analysis phase of the study.
The statistical analysis was performed using a mixed model of Analysis of Variance (ANOVA) to assess the differences in cardiac function parameters LVEF, LVEDd, LVESd, and the E/A ratio between the control and combined groups, serum BNP levels, and outcomes of the 6MWT and MLHFQ. Each group consisted of 22 participants at each timepoint. Following the ANOVA, Tukey's multiple-comparisons tests were applied to determine the significance of differences between the groups. The results were presented using box plots, with a p-value of less than 0.05 considered statistically significant.
Results
Demographic and clinical characteristics of the participants
The demographic and clinical characteristics of the participants who completed the study are presented in Table 1. Regarding the recruitment of cardiac rehabilitation in these patients, out of the 95 patients assessed, 12 patients declined to participate, and 23 patients did not meet the study criteria during the recruitment phase (Fig. 1). The analysis included 22 patients in the control group and 22 in the combined treatment group.
Demographic and Clinical Characteristics of the Study Participants
Values were expressed as n (%) or mean ± SD. p-values for each group were derived from Mann-Whitney test. Chi-square test or Fisher's exact test was used for assessing distribution of observations or phenomena between different groups.
ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; CCB, calcium channel blockers.
The mean age was 65.64 ± 7.41 years in the control group and 65.77 ± 5.30 years in the combined group, with no significant difference between the groups (p = 0.884). Gender distribution was also similar, with 63.6% males in the control group and 68.2% in the combined group (p > 0.999). No significant difference was observed in the distribution of the NYHA functional classification, with 31.8% in class II, 40.9% in class III, and 27.3% in class IV for the control group, compared with 18.2% in class II, 45.4% in class III, and 36.4% in class IV for the combined group (p = 0.561).
The prevalence of diabetes mellitus was 18.2% in the control group and 27.3% in the combined group (p = 0.721). Hypertension was present in 27.3% of the control group and 36.4% of the combined group (p = 0.747). Overall, the baseline characteristics were not significantly different between the two groups, indicating comparability in terms of age, gender, NYHA classification, and comorbidities such as hypertension and diabetes mellitus.
The attrition rate was identical for both groups, with 8 patients lost to follow-up during the 3-month treatment period, leaving 22 participants in each group for the final analysis. Regarding medication use, angiotensin converting enzyme inhibitors/angiotensin receptor blocker was taken by 54.5% of the control group and 45.5% of the combined group, β-blockers by 36.4% and 45.5% respectively, and calcium channel blockers by 27.3% in the control group versus 31.8% in the combined group, with no statistically significant differences noted for these medications.
Notably, it is worth mentioning that there were two cases of severe infection events in the BFR group compared with one case in the control group, with no significant difference between them. Likewise, both groups experienced two death events, and there was no significant difference between them.
Significant improvement in NYHA functional classification with combined BFR training
The study compared the NYHA functional classification before and after treatment between the control and combined groups, as shown in Table 2. Before the intervention, there was no significant difference in NYHA classification between the groups (p = 0.561). After the treatment period, the control group, which underwent isometric limb contractions in conjunction with standard pharmacotherapy, showed some improvement, although not statistically significant (p = 0.723).
Changes of New York Heart Association Scale Between the Two Groups
Values were expressed as n (%). Fisher's exact test was used for assessing distribution of observations or phenomena between different groups.
In contrast, the combined group, which received the same pharmacotherapy, upper limb exercise augmented with BFR training, demonstrated a statistically significant improvement in NYHA classification (p = 0.012). Specifically, the number of patients in NYHA class II increased from 4 (18.2%) to 13 (59.1%), and the proportion in class IV decreased from 8 (36.4%) to 2 (9.1%) post-treatment in the combined group. These results suggest that the addition of BFR to conventional exercise training may contribute to a more substantial improvement in functional status as measured by the NYHA scale.
Enhanced cardiac function parameters following combined training in HFrEF patients
Our study assessed cardiac function parameters through a comparative analysis between the control and combined groups. For the LVEF, the combined group showed a significant increase post-treatment, with the mean LVEF improving from 37.5% to 46.2%, whereas the control group mean LVEF also increased, though less substantially, from 38.0% to 42.2% (p < 0.001 for combined, p < 0.01 for control, Fig. 2A).

Cardiac function assessment comparing control and combined groups. Comparisons of the left ventricular ejection fraction
Regarding the LVEDd, the combined group mean LVEDd decreased from 64.0 to 52.4 mm, whereas the control group showed a smaller decrease from 63.5 to 57.3 mm (p < 0.01 for combined, p < 0.05 for control, Fig. 2B). The LVESd exhibited a similar pattern, with the combined group's mean LVESd reducing from 47.7 to 38.0 mm, compared with a reduction from 47.6 to 42.0 mm in the control group (p < 0.05 for combined, not significant for control, Fig. 2C).
The E/A ratio, indicative of diastolic function, improved significantly in the combined group, moving from 0.93 to 1.24, whereas the control group showed a marginal increase from 0.89 to 1.09 (p < 0.01 for combined, not significant for control, Fig. 2D). When comparing post-treatment results, the combined group mean LVEF was notably higher (46.2% vs. 42.2%, p < 0.01), their mean LVEDd and LVESd were lower (52.4 mm vs. 57.3 mm for LVEDd and 38.0 mm vs. 42.0 mm for LVESd, p < 0.05), and their E/A was elevated (1.24 vs. 1.09, p < 0.05) demonstrating a more significant improvement in cardiac function than the control group.
Substantial reduction in serum BNP levels signifying cardiac improvement
We next evaluated serum BNP levels, a cardiac stress marker, between the control and combined groups. Both groups experienced a decrease in serum BNP after the treatment period, with the combined group exhibiting a more substantial reduction (Fig. 3). The mean serum BNP levels in the control group fell from 963.1 pg/mL before treatment to 537.1 pg/mL after treatment.
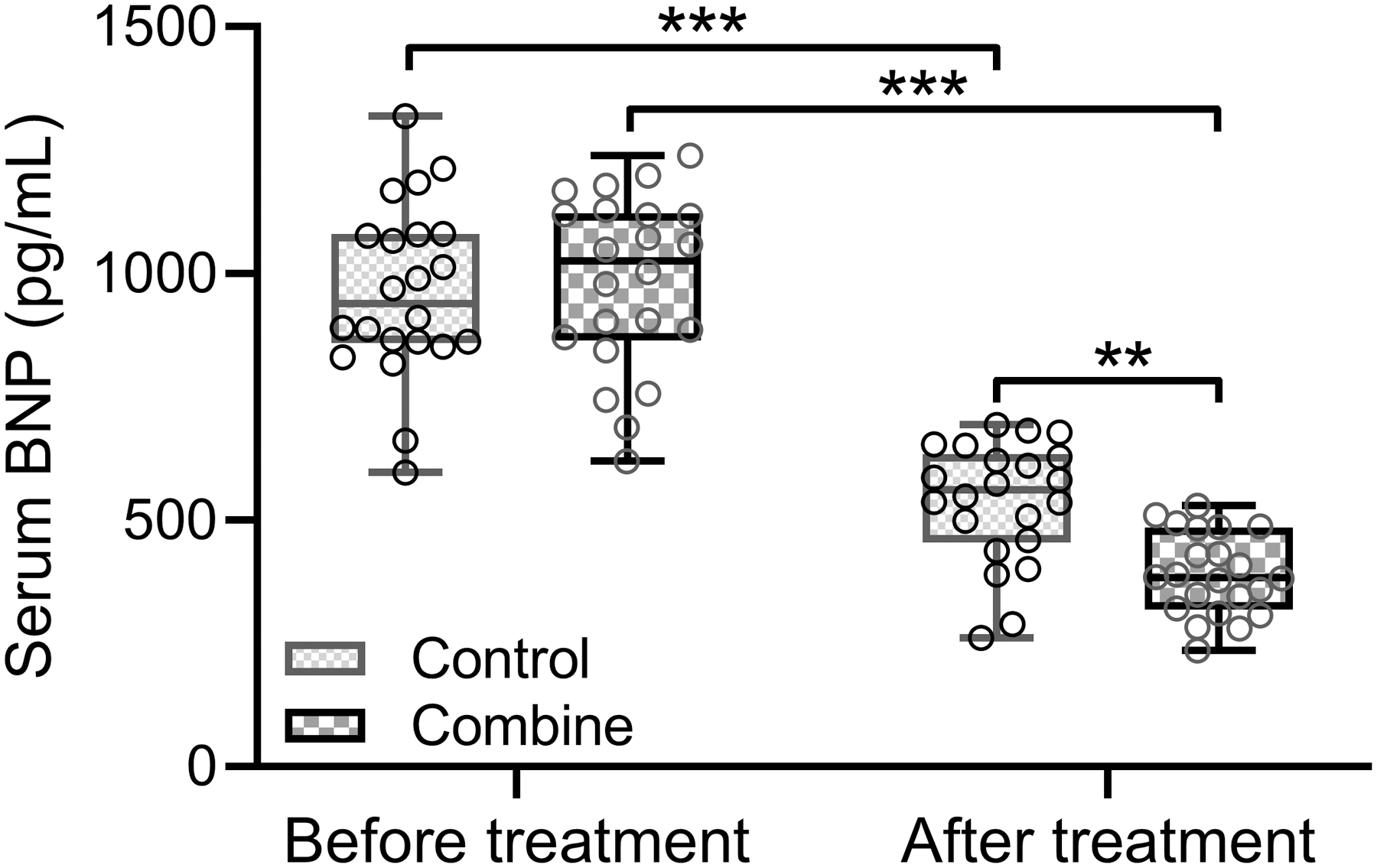
Serum BNP Levels in Control and Combined Groups Over Time. Displayed in box plots are the serum BNP levels compared between the two groups, each with n = 22 participants at each time point. The mixed model of ANOVA followed by Tukey's multiple-comparisons tests was used to calculate significance. Box plot was used to present the data. **p < 0.01, ***p < 0.001. BNP, brain natriuretic peptide.
The combined group saw a decrease from 983.8 pg/mL to 390.0 pg/mL (p < 0.001 for both groups). Notably, the reduction in serum BNP was more significant in the combined group (p < 0.01 when comparing the post-treatment levels between the groups). The box plot data suggest that the combined training regimen outperforms the control in reducing serum BNP levels, implying enhanced cardiac function in patients with HFrEF.
Enhanced physical capacity and quality of life in HFrEF patients post combined training
To assess the physical capacity and quality of life, we employed the 6MWT and the total Minnesota Living with MLHFQ before and after treatment. The result indicated significant improvements in both physical capacity and quality of life for patient post-treatment. Specifically, the mean distance walked in the 6MWT for the control group increased from 320.1 to 379.3 m, whereas the combined group improved from 318.8 to 420.5 m (p < 0.001 for both groups, Fig. 4A). In addition, the mean total MLHFQ score, which assesses the quality of life, decreased from 52.5 to 44.6 in the control group, indicating an improved quality of life, and from 51.1 to 36.9 in the combined group (p < 0.001 for both groups, Fig. 4B).
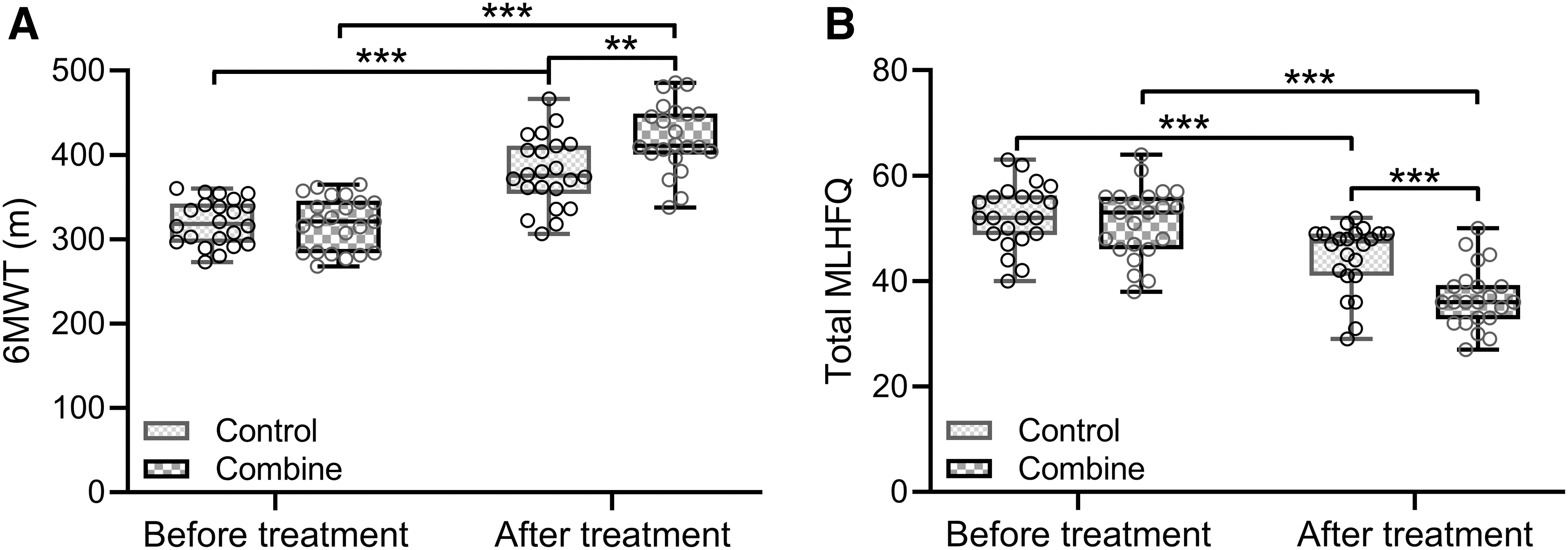
Functional and Quality-of-Life Outcomes Post-Treatment. The box plots for the 6-minute walking test
These results demonstrated that patients in the combined training group not only showed a significant enhancement in their ability to walk further distances but also experienced a greater improvement in their quality of life compared with the control group.
Discussion
This study provided compelling evidence that BFR training could significantly enhance functional, structural, and symptomatic outcomes in patients with HFrEF. Despite similar baseline characteristics, patients in the combined group, who received standard pharmacotherapy and isometric limb contractions augmented with BFR training, showed superior improvements compared with those receiving pharmacotherapy and isometric limb contractions.
Overall, both groups demonstrated effective improvements in cardiac function after a 3-month training period. However, the combined training group exhibited superior outcomes across all measured parameters of cardiac function, suggesting that the inclusion of the combined training regimen may confer a greater benefit to patients with HFrEF.
Our results showed that there were no significant differences in demographic and clinical characteristics between the control and combined groups, underscoring the improvements observed in the combined group as attributable to the intervention rather than underlying demographic or clinical differences. Importantly, our study revealed that the NYHA scales were significantly improved in the combined group compared with the patients who received standard therapy.
It is well known that the NYHA functional class is a subjective measure of a patient's functional ability, with clear distinctions between extreme classes. 19 This enhancement in functional status is an important clinical endpoint, as it directly correlates with patient symptoms, exercise tolerance, and overall quality of life. We observed the shift from higher to lower NYHA classes after combined treatment, suggesting that the combined treatment could facilitate better symptom management and physical function than isometric exercise only.
In fact, a number of studies have demonstrated that resistance exercise, characterized by slow movements and interval training principles, is safe and effective for patients with CHF, leading to improved exercise capacity, muscle strength, and quality of life by counteracting skeletal muscle maladaptation. 20,21 BFR exercise elicits effects comparable to high-intensity workouts, which could safely enhance muscle strength, functionality, and cardiovascular health in patients with cardiovascular disease. 22
A study on patients with congestive heart failure showed that low-load blood flow restricted resistance exercise significantly improved functional capacity, quality of life, and muscle mitochondrial function, unlike remote ischemic conditioning, suggesting its potential in heart failure rehabilitation. 23
Remarkably, our study is the pioneering research to demonstrate the significant enhancement of functional capacity and quality of life in HFrEF patients through combined BFR training. These findings are poised to provide valuable guidance for clinical practice.
Apart from the NYHA functional classification, our study also revealed improved cardiac function parameters in patients who received combined therapy, underscoring the efficacy of these clinical enhancements. The significant increase in LVEF and reductions in LVEDd and LVESd indicate a reversal of cardiac remodeling processes.
These findings are particularly promising, as they suggest that combined BFR training could be a potent adjunctive therapy to induce favorable cardiac adaptations beyond pharmacological management alone. Indeed, previous research has highlighted the advantages of BFR for individuals with considerable functional impairments, who were unable to engage in traditional high-load resistance training.
One clinical trial in musculoskeletal rehabilitation demonstrated that BFR training matched traditional resistance training in muscle rehabilitation efficacy, while providing the added advantages of enhanced functional capacity and pain alleviation without the necessity for high-intensity exertion. 24 Yet, another investigation into cardiovascular and muscular responses indicated that BFR applied during no-load exercise could induce greater fatigue. 25
However, a review on the impact of low-intensity resistance training with BFR on blood pressure, heart rate, and rate-pressure product, finding varied results and suggesting that such training may increase these cardiovascular parameters compared with low-intensity training without BFR, and that these effects are influenced by factors such as cuff width and continuous BFR but are generally within safe limits. 26 A meta-analysis also confirmed that low-load resistance exercise with BFR is as effective as high-load training in enhancing maximal muscle strength across a broad age range of healthy adults. 27
The substantial reduction in serum BNP levels in the combined group is another testament to the clinical efficacy of the combined treatment. Given that BNP is a recognized prognostic marker in heart failure, its marked reduction aligns with the improved cardiac function parameters and enhanced patient outcomes. Moreover, the improvements in physical capacity and quality of life, as evidenced by the 6MWT and the MLHFQ scores, are significant.
The combined group ability to walk further distances and report better quality of life post-intervention holds immense clinical relevance, as these are critical determinants of patient-centered outcomes. Collectively, these findings affirm the positive impact of combining BFR with isometric exercise in patients with HFrEF.
Our study brings forth a significant innovation in the field of HFrEF management. Unlike previous studies, our research explores the novel application of BFR training as an adjunctive therapy to standard pharmacotherapy and isometric limb contractions. The key differentiator lies in the comprehensive improvement observed across multiple dimensions, including functional, structural, and symptomatic outcomes. By combining BFR with isometric exercise, we have achieved notable enhancements in NYHA functional classification, cardiac function parameters, serum biomarkers, physical capacity, and quality of life, all of which collectively emphasize the potential of this innovative approach.
These findings signify a promising avenue for improving the clinical management of HFrEF and open doors to further mechanistic investigations and long-term outcome studies, ultimately advocating for the incorporation of BFR training into standard heart failure rehabilitation protocols.
Conclusions
In conclusion, our study suggests that the combined BFR training, when used in conjunction with standard pharmacotherapy and isometric limb contractions, could lead to substantial benefits in patients with HFrEF. These improvements span across functional classifications, cardiac function parameters, serum biomarkers, physical capacity, and quality of life. Future research should aim at elucidating the mechanistic underpinnings of the combined BFR training benefits and evaluating long-term outcomes to reinforce the integration of this modality into standard heart failure rehabilitation protocols.
New & Noteworthy
The study supported the integration of BFR training into conventional HFrEF treatment regimens to maximize patient recovery outcomes.
Footnotes
Authors' Contributions
P.W. and Y.L. contributed to the conception and design of the research; Y.L. contributed to the design of the research; P.W. and Y.L. contributed to the acquisition and analysis of the data; P.W. and Y.L. contributed to the interpretation of the data; and P.W. and Y.L. drafted the article. All authors critically revised the article, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the Research Fund of Anhui Medical University (2021xkj201).