
Abstract
Successful aging is essential for health, particularly as the global population of older adults rises. It assesses whether older adults maintain a healthy lifestyle and enjoy quality in their later years. This study explores the relationship between successful aging and mortality, focusing on how its components relate to mortality across different genders. We conducted a longitudinal analysis of 9633 older adults (aged 65+) from the Chinese Longitudinal Healthy Longevity Survey (2011–2018). This study used two definitions of successful aging: SA I includes five dimensions (the absence of major diseases, no subthreshold depression, freedom from disability, high cognitive function, and active social participation); SA II consists of four dimensions and excludes the absence of major diseases. Both genders exhibited lower mortality rates among those achieving successful aging (males: hazard ratio [HR] = 0.62 for SA I, HR = 0.65 for SA II; females: HR = 0.57 for SA I, HR = 0.58 for SA II). All successful aging dimensions correlated with reduced death risk, except for subthreshold depression in females. In males, significant reductions in mortality were linked to freedom from disability (HR = 0.49) and active social participation (HR = 0.60). In females, these were notable for freedom from disability (HR = 0.46) and high cognitive function (HR = 0.47). SA I, which includes the absence of major diseases, is more relevant for Chinese younger old. The influence of successful aging components on mortality risk varies by gender, emphasizing the importance of addressing functional daily living challenges to enhance the health of older adults in China.
Introduction
Population aging presents a global challenge, with the United Nations reporting that the population aged 60 and above was 962 million in 2017 and is projected to reach 2.1 billion by 2050. 1 In China, life expectancy at birth rose from 71.6 years in 2000 to 77.4 years in 2019, indicating a rapidly aging society. 2 This has led to a focus on “how to age better,” 3 emphasizing the significance of “successful aging.”
The term “successful aging,” initially defined by Havighurst 4 as “getting satisfaction out of life” and “adding vitality to the years,” has evolved through research. 5 Rowe and Kahn conducted a systematic study, characterizing successful aging as a relative concept marked by a slower decline in physical, social, and cognitive function than ordinary aging. 6 They proposed a three-factor framework: lower illness-related disability risk, higher cognitive and physical functioning, and active life participation. 7 Despite ongoing research, no universal criteria for successful aging exist.
Rowe and Kahn’s model remains prominent, yet some scholars critique its stringent requirement for the absence of disease. 8 The World Health Organization indicates that many older adults manage physical illnesses effectively, which minimally impacts their functionality. 9 A U.S. study suggests that redefining successful aging without strict disease criteria may be more beneficial. 10 Similarly, a Korean study found that recognizing the absence of chronicity aids in identifying successful aging in younger older adults. 11 Tkatch emphasized that older adults with chronic conditions can age successfully, highlighting the role of health awareness in the aging process. 12
Although scholars define successful aging differently, current global research on successful aging can be categorized into two primary components: the factors influencing successful aging and the predictions of successful aging on future health.13,14 Regarding the factors influencing successful aging, scholars have found that years of schooling, risk of falls, regular physical activity, and the sociodemographic characteristics of the individual are good predictors of successful aging in older adults.15–18 On the contrary, concerning successful aging as a predictor of health outcomes,19,20 foreign scholars have found that positive components of successful aging play a significant role in the prognosis of older adults. 21 Currently, research on successful aging in China has started later than in other countries, particularly those examining the relationship between successful aging and mortality.
This study aims to investigate the association between two criteria of successful aging, their components, and mortality. Moreover, it seeks to explore how this relationship varies by sex. The study also aims to determine whether the concept of successful aging, which excludes major diseases, is applicable to the older adults’ population in China. Lastly, it endeavors to identify the dimensions that older adults in China should prioritize.
Methods
Sample and study design
We utilized data from the Chinese Longitudinal Healthy Longevity Surveys (CLHLS), which includes 631 county-level regions across 23 provinces and cities in China. The baseline survey commenced in 1998, followed by surveys in 2000, 2002, 2005, 2008–2009, 2011–2012, 2014, and 2017–2018.
For this study, we analyzed the CLHLS longitudinal database from 2011 to 2018, involving two follow-up visits. The 2011 baseline included 9765 participants; we then excluded 132 participants who were under 65 years old or had missing data on assessing successful aging. Following the follow-up visits, there were 4666 survivors and 2832 deaths, with a total of 2133 individuals lost to follow-up. Ultimately, 9633 participants were included in the final analysis. (Fig. 1) The CLHLS study was approved by the Biomedical Ethics Committee, Peking University (IRB00001052-13074).
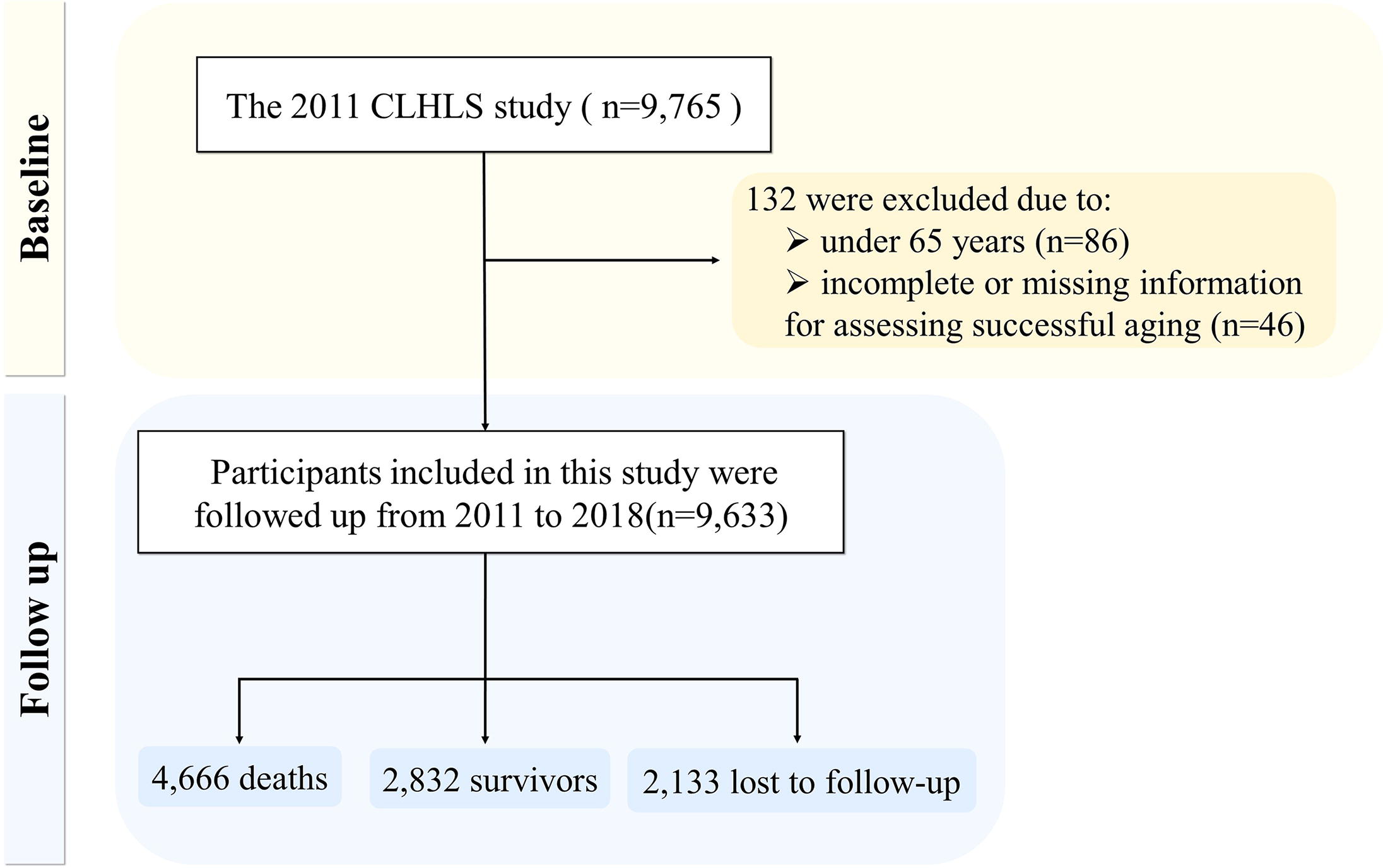
Flow chart of the study population.
Definition of successful aging
In this study, we have adopted two definitions of successful aging: SA I based on Rowe and Kahn’s model, 7 and SA II based on a Korean study. 11
SA I: According to Rowe and Kahn’s model, 7 it was characterized by five criteria that must be met simultaneously: absence of major diseases, no subthreshold depression, freedom from disability, high cognitive function, and active social participation.
SA II: In contrast, the Korean study 11 broadened the definition of successful aging to include four criteria: no subthreshold depression, freedom from disability, high cognitive function, and active social participation, while excluding the absence of major diseases as a criterion.
Components of successful aging
Absence of major diseases: Participants were asked if they had any of the following major conditions as diagnosed by a physician: diabetes, heart disease, stroke or cerebrovascular disease, chronic lung disease, or cancer. 22 Participants without any of these five diseases were considered to have an absence of major diseases; otherwise, they were considered to have major diseases.
No subthreshold depression: The 2011 survey did not include a complete depression scale; therefore, the participants’ depression was assessed based on two questions from the personality traits measurement section, 23 as investigated by Han et al. 24 : (1) Whether the participants felt sad and depressed for at least 2 weeks in the past year; (2) Whether there was a loss of interest in hobbies, work, or other enjoyable activities for at least 2 weeks in the past year. If the answer to both questions is “no,” the participant is considered to have no subthreshold depression. Conversely, if the answer to at least one question is “yes,” the participant is classified as having subthreshold depression.
Freedom from disability: We used the activities of daily living (ADL) scale to assess functional loss in older adults. 22 This scale comprises five daily activities: bathing, dressing, toileting, indoor mobility, and eating. Participants were presented with three response options: “No help,” “Need some help,” and “Need full help.” We defined “No help” for each of the five ADL as indicative of freedom from disability; otherwise, participants were classified as having a disability.
High cognitive function: The cognitive function survey included 25 questions across four categories: daily memory, word recall, arithmetic, and drawing. One point was awarded for each correct answer, while zero points were assigned for incorrect or unanswered questions. The total score ranged from 0 to 25. 25 In this study, a score of median or higher was defined as indicative of high cognitive function. 26
Active social participation: Drawing on existing literature22,23 and integrating data from this study, the social participation status of older adults was comprehensively evaluated using four specific questions: personal outdoor activities, involvement in social activities, card or mahjong playing, and travel frequency over the past 2 years. Participants were considered to have active social participation if they engaged in “personal outdoor activities” at least once a month, “participated in social activities” at least once a month, “played cards or mahjong” at least once a month, or had traveled at least once within the past two years.
Mortality
All-cause mortality was examined over a 7-year follow-up period extending from 2011 to 2018. Data on deaths were obtained from death certificates and family interviews.
Covariate data collection
We also gathered data on the basic characteristics, including age (65–84 or ≥85 years), residence (urban or rural), marital status (partner or no partner), education level (<4 or ≥4 years), self-rated economic status (good, average, or poor), cigarette smoking (smoking or no smoking), alcohol consumption (drinking or no drinking), and physical activity (yes or no).
Statistical analysis
Descriptive statistics for individual characteristics were stratified by sex. A chi-squared test was utilized to compare the two definitions and the composition of successful aging. The cox proportional hazards regression model was employed to evaluate the relationship between successful aging and mortality in older adults, and to determine the hazard ratio (HR) and 95% confidence interval (CI). The regression model was adjusted for residence, marital status, education level, self-rated economic status, cigarette smoking, alcohol consumption, and physical activity. Furthermore, cumulative mortality curves for successful aging and its components were plotted. All analyses were performed using IBM SPSS 22.0 software, with p ≤ 0.05 indicating statistical significance. GraphPad Prism 9 was used for plotting.
Results
Characteristics of the study population
The baseline characteristics of the 9633 participants, comprised 4309 males and 5324 females. Male participants were, on average, younger than their female counterparts (83.31 vs. 88.11 years, p < 0.001). Overall, a higher percentage of male participants exhibited the following characteristics: having partners, possessing >4 years of education, smoking, consuming alcohol, and engaging in physical exercise (p < 0.001) (Table 1).
Characteristics of the Study Population in 2011
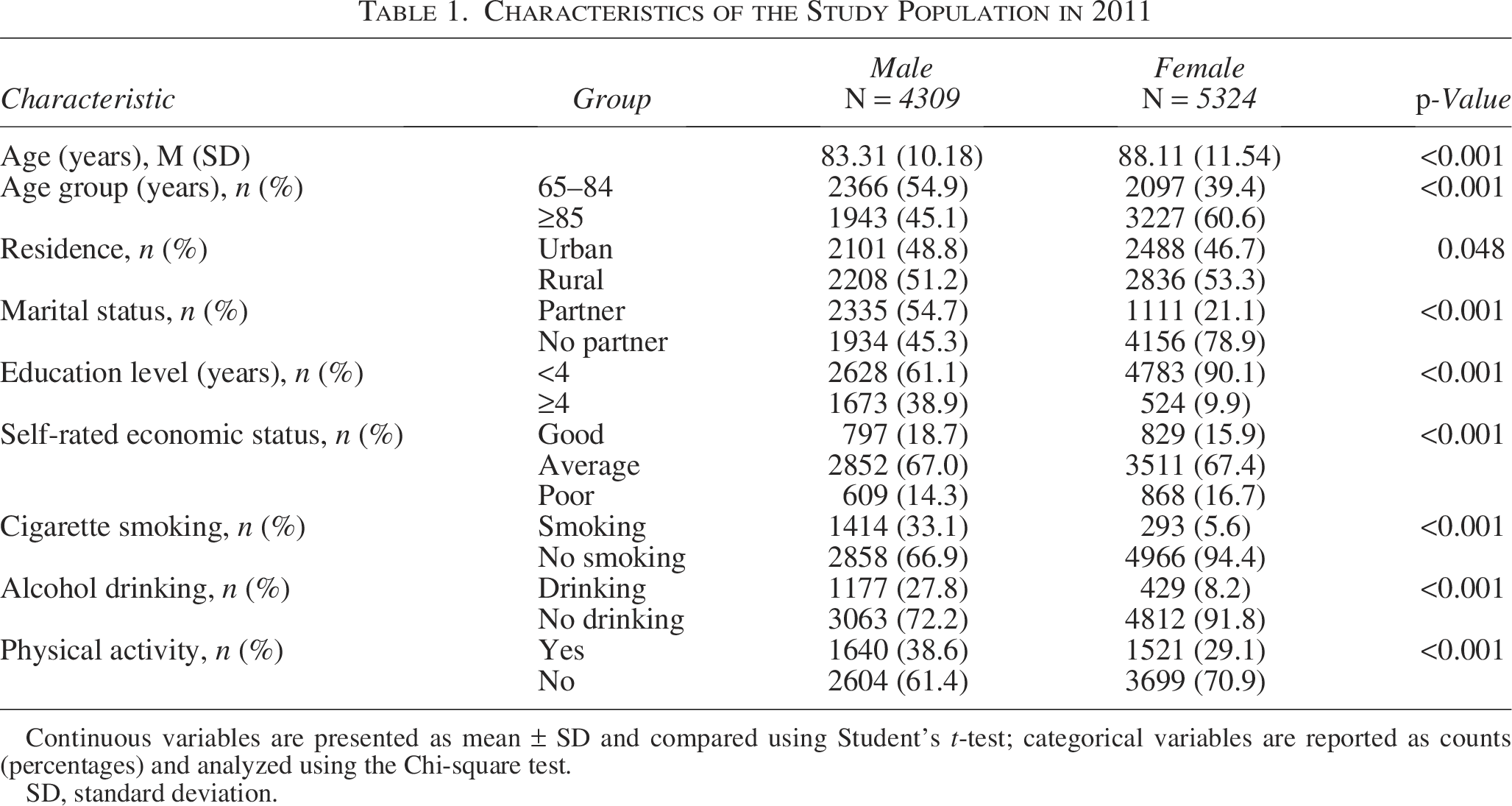
Continuous variables are presented as mean ± SD and compared using Student’s t-test; categorical variables are reported as counts (percentages) and analyzed using the Chi-square test.
SD, standard deviation.
Distribution of successful aging and its components
Table 2 shows the percentage of the study population meeting each definition and component of successful aging. Generally, the successful aging rate for SA I was 20.5% in 2011. If the criterion of successful aging did not consider major diseases, the rate of SA II (30.1%) was higher than that of SA I. A higher proportion of men (26.4%) achieved SA I compared with women (14.3%), and similarly, men had a higher successful aging rate for SA II (38.1%) than women (21.3%) (p < 0.001). However, the successful aging rate for SA I was lower than that of SA II for both genders. Men showed higher positive dimensions of successful aging than women, except for those with the absence of major diseases (p < 0.001).
The Percentage of Study Populations Meeting Each Definition and Component of Successful Aging
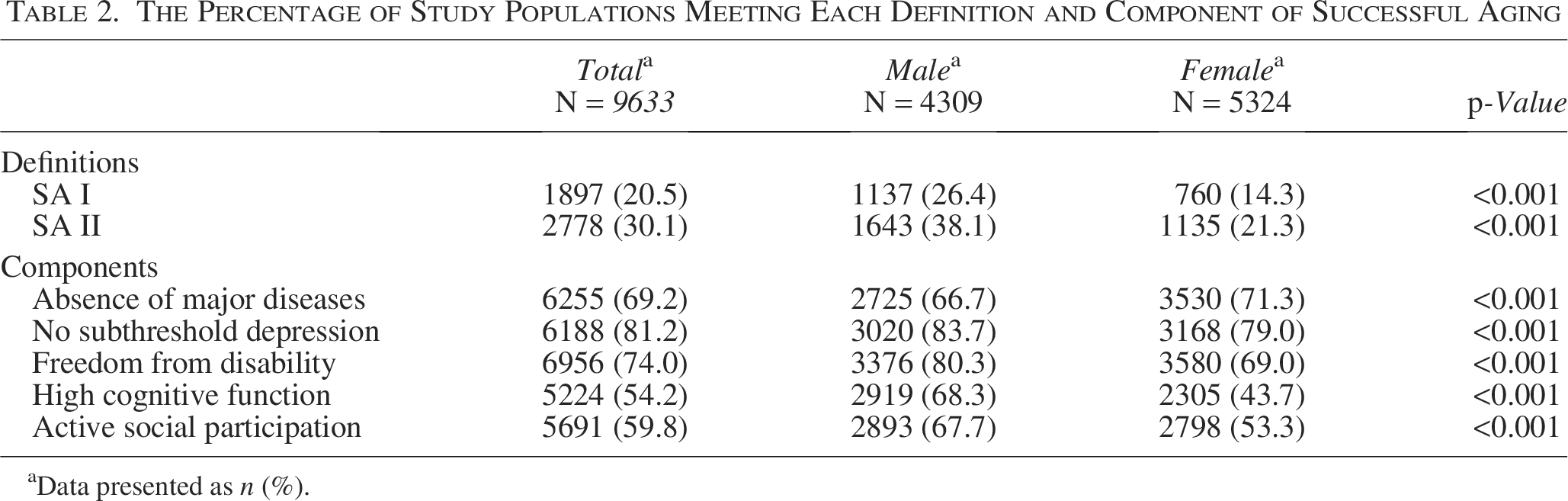
Data presented as n (%).
Cumulative mortality
Figure 2 depicts cumulative probability plots of all-cause mortality across components of successful aging. Among male individuals, the incidence of all-cause mortality was lower in older adults without major diseases and those without subthreshold depression (p < 0.05); however, no significant difference was observed between these two factors in females (p > 0.05). Furthermore, freedom from disability, high cognitive function, and active social participation were associated with a reduced risk of all-cause mortality, regardless of gender (p < 0.001).
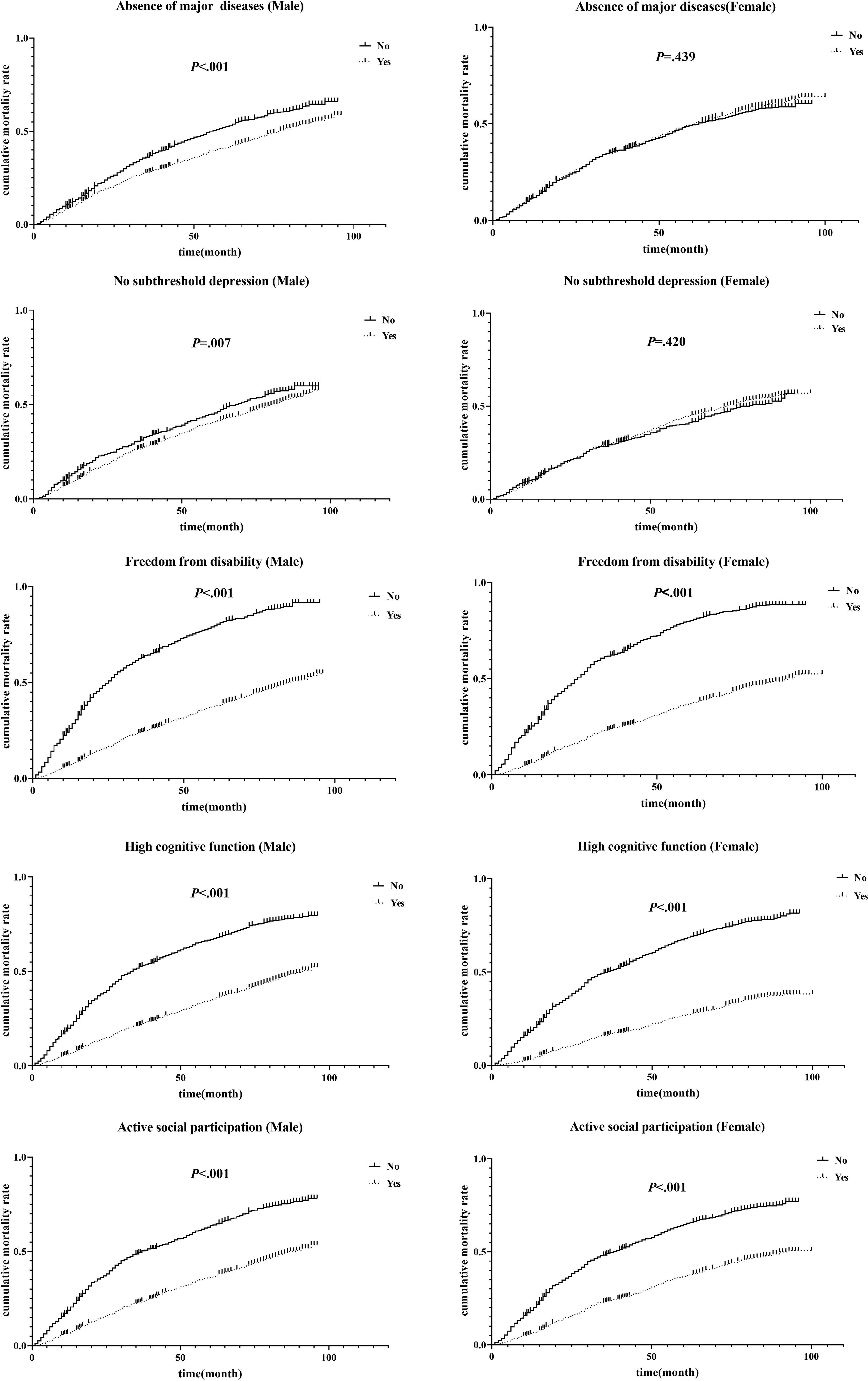
Cumulative mortality plot of all-cause mortality in successful aging by gender.
Association of successful aging and its components with all-cause mortality by gender
Table 3 shows the HR for all-cause mortality in relation to successful aging for both men and women. For males, achieving successful aging was associated with a lower mortality risk (HR = 0.62, 95% CI: 0.55–0.70 in SA I; HR = 0.65, 95% CI: 0.58–0.72 in SA II). Similar results were observed for females, with those who achieved successful aging having a lower risk of death (HR = 0.57, 95% CI: 0.49–0.67 in SA I; HR = 0.58, 95% CI: 0.51–0.66 in SA II). In terms of the components of successful aging, all positive components, except for the absence of subthreshold depression in females, were associated with a reduced risk of death in older adults. For males, freedom from disability (HR = 0.49, 95% CI: 0.44–0.54) and active social participation (HR = 0.60, 95% CI: 0.54–0.67) were the dominant factors in reducing the risk of death. For females, freedom from disability (HR = 0.46, 95% CI: 0.42–0.50) and high cognitive function (HR = 0.47, 95% CI: 0.43–0.52) were the dominant factors in reducing the risk of death.
Hazard Ratios (95% CI) of All-Cause Mortality for Successful Aging and Its Components by Sex
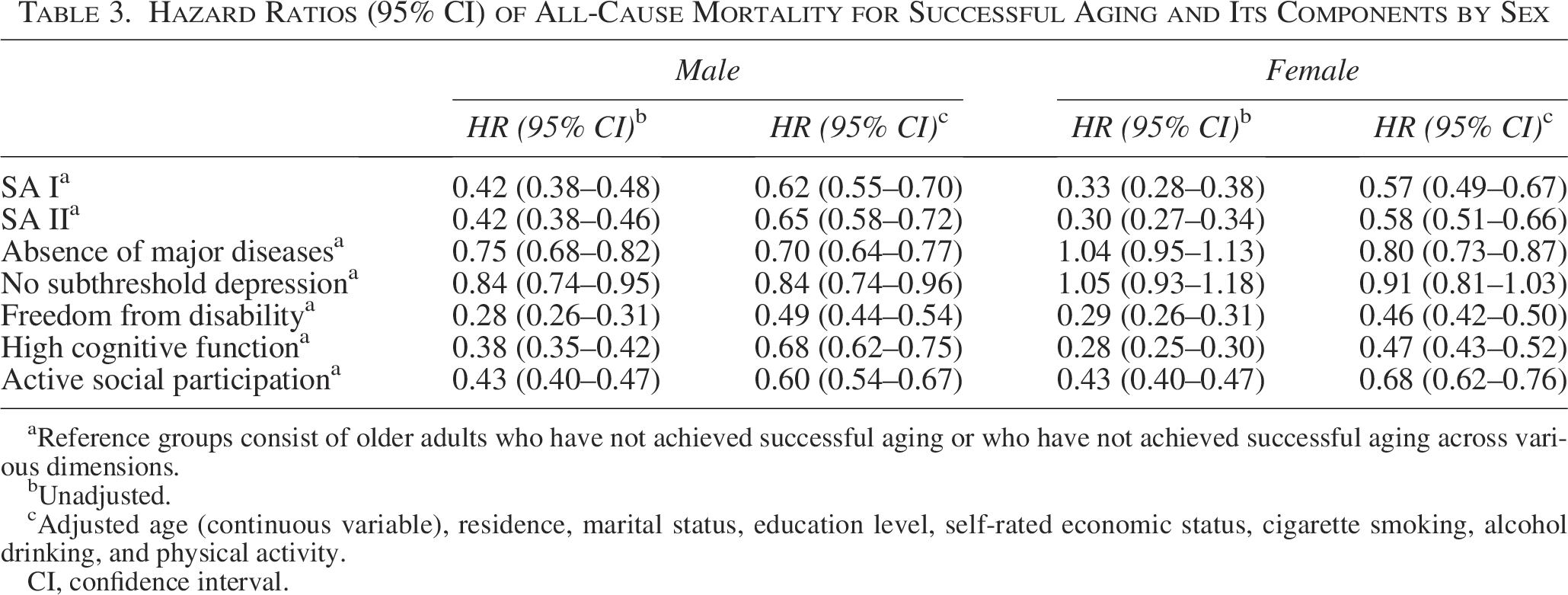
Reference groups consist of older adults who have not achieved successful aging or who have not achieved successful aging across various dimensions.
Unadjusted.
Adjusted age (continuous variable), residence, marital status, education level, self-rated economic status, cigarette smoking, alcohol drinking, and physical activity.
CI, confidence interval.
Age stratification analysis
Figure 3 shows the HRs for all-cause mortality in relation to successful aging and its components for both males and females across different age groups. In the 65–84 age group, males who achieved successful aging had a lower risk of death, with HRs of 0.60, 95% CI: 0.50–0.72(C-indexes of 0.58, 95% CI: 0.55–0.61) for SA I and 0.64, 95% CI: 0.54–0.75 (C-indexes of 0.57, 95% CI: 0.55–0.60) for SA II. For those aged 85 and older, the reduced risk remained significant, with HRs of 0.590, 95% CI: 0.499–0.699 (C-indexes of 0.56, 95% CI: 0.53–0.59) for SA I and 0.588, 95% CI: 0.508–0.681 (C-indexes of 0.58, 95% CI: 0.55–0.60) for SA II (detailed results, preserved to three decimal places, are shown in Supplementary Table S1). Similarly, females exhibited comparable outcomes, with SA I predominant in the 65–84 age group (HR = 0.62, 95% CI: 0.47–0.80; C-indexes of 0.58, 95% CI: 0.55–0.61 for SA I; C-indexes of 0.56, 95% CI: 0.53–0.57 for SA II) and SA II dominating in the over 85 age group (HR = 0.49, 95% CI: 0.42–0.58; C-indexes of 0.55, 95% CI: 0.53–0.57 for SA I; C-indexes of 0.56, 95% CI: 0.54–0.59 for SA II). In older males and all females, the predominant low mortality risk factors remained unchanged. However, among males in the 65–84 age group, freedom from disability (HR = 0.31, 95% CI: 0.25–0.38) and absence of major diseases (HR = 0.54, 95% CI: 0.46–0.63) were the primary factors associated with reduced mortality. Specific results are presented in Supplementary Tables S1 and S2.

Forest plot of hazard ratios for all-cause mortality in relation to successful aging and its components.
Discussion
This study examined successful aging among the older adults in China, revealing that older adults who successfully aged had a reduced risk of all-cause mortality. All positive components of successful aging were linked to lower mortality risk, except for women without subthreshold depression. In males, the strongest association was between freedom from disability and active social participation, while in females, it was between freedom from disability and high cognitive function. Our findings suggest that successful aging criteria excluding major diseases may better identify successful aging in younger older adults, with looser criteria being more applicable to older adults. Additionally, achieving successful aging correlates with a lower risk of all-cause mortality, with varying contributions of each component by sex.
In this study, the prevalence of successful aging in the 2011 CLHLS was 20.5%, with a lower rate of 30.1% using a relaxed definition, both significantly lower than the 38.1% reported in a 2012 CLHLS study. 27 This discrepancy may arise from differing criteria for successful aging; the previous study assessed it based on six dimensions, requiring only three to be met, while our criteria are more stringent. Notably, prevalence rates of successful aging vary widely in prior studies, ranging from 0.4% to 95.0%.28,29
The rate of successful aging was higher in male older adults than in females, regardless of the criteria applied, consistent with previous research.21,30 Females showed lower rates across all dimensions of successful aging, except for a higher prevalence of major chronic diseases. While females generally have a longer lifespan, older females often face disadvantages in financial income, physical and mental health, and social status compared with older males. 31
Older adults who achieved successful aging exhibited a lower risk of death compared with those who did not, with a 38% (HR = 0.62, p < 0.001) reduction in the risk of death for males who achieved SA I and a 43% (HR = 0.57, p < 0.001) reduction for females. These results align with those of two previous studies on the potential relationship between successful aging and mortality.13,21 Although these two studies employed different definitions of successful aging, but their findings support our results by emphasizing the importance of achieving successful aging to decrease the risk of future death. Successful aging is closely related to an individual’s health status, mental health, functional abilities, cognitive function, and social participation, all of which are associated with health outcomes in older adults. Therefore, the relationship between successful aging and mortality may interact through multiple mechanisms involving these factors, ultimately influencing an individual’s overall health and survival rate.
It is noteworthy that our stratified analysis revealed that SA I is more effective in identifying the survival status of younger older adults, while SA II is better suited for older populations. A study conducted in South Korea similarly found that the definition of chronic diseases is less applicable in individuals aged 74 and older. 11 Although the older individuals with one or more chronic diseases generally have lower survival probabilities,32–35 other research indicates that those reaching the age of 80 or older are more likely to experience better control and management of their chronic conditions compared with their younger counterparts. 36 Therefore, it is crucial to focus on daily functioning in this high-age older adults.
In terms of the components of successful aging, this study revealed that the absence of major diseases, lack of subthreshold depression (except in females), freedom from disability, high cognitive function, and active social participation were all significantly associated with a reduced risk of death. These findings are consistent with previous research.37,38 High levels of depressive symptoms have been shown to increase mortality risk in older adults, 39 and those with disabilities experience higher mortality rates compared with their nondisabled counterparts. 19 Declining cognitive function can diminish older people’s perception of their underlying illness and symptoms, leading to severe functional dependence and poor quality of life, ultimately resulting in disease progression and more serious outcomes. 40 Meta-analysis indicates that individuals with good social relationships may benefit from better health practices and psychological processes and have higher survival rates than those with inadequate social relationships. 41
Notably, the strength of the association between successful aging and lower mortality risk differs by gender: among males, the strongest correlations are seen with being free from disability and active social participation, while among females, these are freedom from disability and high cognitive function. The health status differences between the sexes are multifactorial, influenced by biological, genetic, and social factors.42–44 Older men typically have more social participation opportunities, which can alleviate negative emotions and enhance life satisfaction, thereby promoting physical and mental health. 45 Conversely, lower educational levels and postmenopausal estrogen reduction in females contribute to decreased cognitive function compared with males. 46 Cognitive dysfunction adversely affects daily life and may lower life expectancy. 37 Future research should explore how these risk factor differences contribute to gender disparities in mortality.
This study has several limitations. First, death information was sourced from household interviews based on death certificates, providing all-cause mortality data without specifying the exact causes of death. Second, recall bias may affect the self-reported data in the CLHLS questionnaire, which relies on older adults’ memory for disease diagnosis. Third, the absence of a depression scale in the 2011 CLHLS questionnaire led to the use of two related questions to assess subthreshold depression, potentially misrepresenting respondents’ actual conditions. Lastly, while multiple covariates were adjusted for, the possibility of confounding the relationship between successful aging and mortality by unmeasured variables remains. Future research should consider additional factors such as dietary behaviors, family dynamics, social support, and health care access patterns.
In conclusion, our findings indicate that the criteria for successful aging, including the absence of major diseases, are particularly beneficial for younger older adults in China. Interestingly, when this dimension is excluded, the criteria become more applicable to older adults. Individuals who experience successful aging have a lower mortality risk than those who do not. The impact of successful aging factors on mortality risk varies by gender. Initiatives focused on addressing daily functional disabilities in older individuals may promote successful aging. To increase the life expectancy of older men, it is essential to improve their social participation and chronic disease management. Additionally, enhancing cognitive function is particularly important for older women.
Authors’ Contributions
W. Li.: Conceptualization, data curation, formal analysis, data visualization, writing—original draft. X.F.: Data curation, formal analysis. W.X.: Data visualization, writing—sections of the article. G.Z.: Data visualization. Y.L.: Writing—sections of the article. X.Z.: Writing—sections of the article. W. Lu.: Conceptualization. Y.W.: Conceptualization, writing—sections of the article.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the participants and researchers from the CLHLS who contributed or collected data. This work was made possible by the generous sharing of CLHLS summary statistics.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
Ethics Statement
This study gained the approval of the Biomedical Ethics Committee of Peking University (IRB00001052-13074).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.