
Abstract

Introduction
According to the Intergovernmental Panel on Climate Change (IPCC), climate change refers to naturally occurring or anthropogenic changes in climate that may be observed through long-term changes in climate attributes such as mean surface temperature and precipitation (United Nations Framework Convention on Climate Change, 2011). Despite the multiple facets of climate change, most documented evidence and contemporary deliberations have focused on global warming. Global warming refers to the rapid increase of Earth's mean surface temperature in the recent past, which has substantially been driven by anthropogenic activities. The IPCC has stated that between 1951 and 2010, anthropogenic activities contributed to more than half of the recorded rise in average surface temperature of Earth (Pachauri et al., 2014; Stocker et al., 2014).
Combustion of fossil fuels, in addition to other factors such as deforestation, is regarded as the principal cause of global warming. Combustion of fossil fuels leads to the emission of greenhouse gases (GHGs), predominantly carbon dioxide (CO2), which in turn causes warming of the planet by inhibiting the transmission of heat away from its surface (Climate Impact Lab, 2019). Therefore, even though global warming and climate change are often used interchangeably, they represent distinct but related phenomena. However, global warming, primarily driven by CO2, may be considered as the single-most important cause of climate change (Singh & Singh, 2012). It is crucial to note that although combustion of fossil fuels releases a number of pollutants such as CO2, nitrogen oxides, and sulfur dioxide, the emphasis on CO2 is justified not only because it is a fundamental constituent of GHGs, but also because it increases ambient ozone and particulate matter (PM) concentrations that are known to have adverse implications for human health (Jacobson, 2008).
While most research examining the linkages between climate change and human health has emphasized the need to mitigate human health risks emanating from extreme weather events such as heat waves and vector-borne diseases such as malaria and dengue, only a limited amount of evidence has elucidated the relationships between climate change and noncommunicable diseases (NCDs) (Friel et al., 2011). Furthermore, even though the Paris Agreement is widely perceived as the most persuasive health agreement that has garnered global support from member states to help decelerate the pace of global warming to below 2 degrees Celsius, and ideally below 1.5 degrees Celsius (from pre-industrial levels), recent projections on global warming present a dismal scenario (World Health Organization, 2018).
According to recent projections, if the current rise in CO2 emissions continues unabated, global mean temperatures could rise by 3 to 5 degrees Celsius by 2100 (IPCC, 2018). Given that NCDs accounted for almost 74 percent of global deaths in 2019 and rapid increase in primary energy consumption would further increase environmental pollutants, accelerate the climate change process, and cause an increasing number of premature deaths, it is vital to take cognizance of factors that exacerbate the looming threat posed by NCDs (Institute for Health Metrics and Evaluation, 2019).
With the help of cross-country examples, this Commentary makes a case for mainstreaming NCDs in climate change discourses. Since fossil fuel-driven primary energy consumption is anticipated to register an unprecedented spike and cause an overwhelming increase in CO2 emissions, the human health impact of environmental pollutants is likely to manifest in the form of NCDs (Armaroli & Balzani, 2011; Frumkin and Haines, 2019). A global consortium that tackles the impending burden of NCDs has the potential to mitigate the threat posed by environmental pollutants.
Fossil Fuel Combustion and Environmental Pollutants
According to the World Health Organization (WHO), PM, ozone, carbon monoxide, nitrogen dioxide, and sulfur dioxide are among pollutants that pose grave hazards to human health (WHO, 2022). While PM and ozone are typically referred to as ambient air pollutants, this Commentary uses the term environmental pollutants because these pollutants exacerbate the burden of NCDs by causing climate change and via several environmental pathways.
Several toxic pollutants including volatile organic compounds (VOCs) have also surfaced in contemporary discussions related to pollution management. However, it is worthwhile to clarify that many pollutants such as carbon monoxide and VOCs (including methane) can act as precursors to the formation of PM and ozone. Moreover, nitrogen oxides and sulfur dioxide interact in the atmosphere to form PM. Elevated levels of nitrogen oxide often cause ozone levels to rise (Melamed et al., 2016).
Note that PM is a generic term that encompasses a multitude of pollutants. PM consists of particles varying in size. PM2.5 and PM10 are the most commonly measured PM and refer to particles of aerodynamic diameter smaller than 2.5 mm and 10 mm, respectively. The composition of PM may also differ from heavy metallic particles to compounds that dissolve in air. It is also important to highlight that PM refers to both primary and secondary PM. While primary PM is released directly into the air from combustion of fossil fuels, secondary PM is produced from precursor emissions such as sulfur dioxide, nitrogen oxides, VOCs, and ammonia (Hodan & Barnard, 2004). VOCs are often the main source of secondary PM in warm and humid conditions (Shao et al., 2020). The term VOCs is an umbrella term that includes a variety of gaseous compounds that are released from certain solid and liquid substances. These compounds have a very high vapor pressure at normal temperatures, which is why their concentration in indoor environments is much higher than in the outdoors.
Despite the role of CO2 emissions in intensifying the process of global warming and escalating the burden of NCDs, CO2 is not regarded as an air pollutant. This is because the ambient mixing ratios of CO2 are inadequate so that by itself CO2 can seldom be harmful for human health (Jacobson, 2008). However, CO2 increases ambient ozone and PM concentrations that are known to have adverse effects on human health.
Elevated CO2 levels create a greenhouse effect and prevent solar radiation from reflecting back to space. Heat and water vapor from high CO2 levels trigger the interaction of carbon monoxide, a compound released as a result of combustion of fossil fuels, with hydroxyl radicals to form CO2. Elevated levels of nitrogen oxides further catalyze oxidation of the gaseous compounds to form ground-level ozone. Higher levels of CO2 increase PM concentrations by increasing air temperatures, which help PM remain stable above the ground for longer durations. Raised CO2 levels also lead to an increase in relative humidity and reduced wind speed, which help in the accumulation of PM and inhibit its diffusion (Crutzen & Andreae, 1990).
Environmental Pollutants and NCDs
Combustion of fossil fuels enhances the risk of developing NCDs mainly via two interdependent pathways: environmental pollutants such as PM and ambient ozone, and climate change. The two pathways are interdependent because in addition to causing NCDs directly, environmental pollutants accelerate the process of climate change, which may also indirectly lead to NCDs (Frumkin & Haines, 2019). While it is well established that prolonged exposure to toxic environmental pollutants can result in a significant mortality burden caused by NCDs like cardiovascular diseases (CVDs), climate change may exacerbate the risk of these NCDs through a host of mechanisms. NCDs typically include heart diseases and stroke, but also include diabetes and chronic kidney diseases, chronic respiratory diseases, neoplasms/cancers, and digestive diseases. In addition, it is important to note linkages between exposure to environmental pollutants and impaired cognitive function and neurotoxicity, which are also being investigated (Clifford et al., 2016).
Climate Change and NCDs
Climate change can aggravate the NCD burden through several pathways. Since climate change is expected to increase the average number of hot days in a year, physiological responses such as heavy breathing may increase the inhalation of environmental pollutants. The inhalation of environmental pollutants, for example PM, can result in oxidative stress and an excessive sympathetic nervous system (SNS) response. Short-term SNS activation is often the cause of serious cardiac episodes such as atrial fibrillation and myocardial infarction while chronic SNS activation is linked to ischemic heart disease and congestive heart failure. Excessive perspiration due to warming is also associated with an increase in cardiac strain, plasma cholesterol, and blood viscosity, which increases the risk of CVDs. There is also evidence to indicate that inhalation of certain micro- and nanoparticles has the potential to adversely impact the cardiovascular system by rapidly translocating into the circulatory system (Manolis et al., 2014; Morishita et al., 2015).
Warmer temperatures increase the risk of mortality and morbidity due to CVDs by causing sleep disturbances. Shorter sleep duration and fragmented sleep is linked to increased risk of hypertension, calcification of the arteries, and obesity, all of which are risk factors for CVDs. In certain epidemiological studies, shorter sleep duration has also been associated with vascular damage (Cappuccio et al., 2011). Furthermore, physical activity is considered beneficial for cardiovascular health as it reduces hypertension and abnormal SNS activity (Mueller, 2007). Hot weather contributes to the risk of developing CVDs by acting as a deterrent to outdoor physical activity (Edwards et al., 2015).
Warmer ambient temperatures are likely to worsen the burden of cancers and diabetes due to increased physical inactivity and obesity (Dain & Hadley, 2012). An excess amount of body fat and persistently high levels of blood glucose lead to insulin resistance and hyperinsulinemia. Excess stimulation of insulin and accompanying binding proteins can aggravate the risk of several cancers by causing tumorigenesis. On the other hand, regular physical activity elevates the level of antioxidants in the body and reduces oxidative stress and insulin resistance. Physical activity is known to reduce inflammatory biomarkers in the body by reducing adiposity levels, which also trigger the development of cancers (Friedenreich et al., 2021).
Rural inhabitants living along the coastlines of developing countries are exposed to increased risk of NCDs such as hypertension and diabetes caused by salination of drinking water. The population in such locales is often dependent on untreated water sources for meeting their drinking water needs. For example, in South and Southeast Asia, tropical cyclones and inland flooding are expected to cause seawater contamination of coastal and inland drinking water sources (Hoque et al., 2016). In addition to direct contamination of water bodies, salination of soil and groundwater may lead to excessive sodium content in food crops (Frumkin & Haines, 2019). By causing an increase in the incidence and severity of cyclonic tropical storms and floods, climate change is likely to exacerbate the risks associated with saline intrusion.
Climate change can increase the burden of cancers through several mechanisms. First, by increasing the frequency and intensity of extreme weather events, climate change can cause enhanced exposure to carcinogens. Increase in the frequency of forest fires as a result of global warming is considered an important source of carcinogenic compounds that are suspended in air and carried to far-off places (Nogueira et al., 2020). Second, scientific evidence has suggested that global warming and stratospheric ozone depletion have contributed to the rise of skin cancer episodes worldwide (Parker, 2021). Third, the impact of altered meteorological phenomena on depletion of air and water quality is likely to worsen the burden of cancers in low- and middle-income countries (Ghosh et al., 2023). Fourth, climate change can increase the incidence of cancers by adversely impacting agricultural yield and limiting the availability of nutrient-rich food (Ghosh et al., 2023). Finally, the incidence of cancers is anticipated to increase due to indiscriminate pesticide use in agriculture. This is because rapidly changing climate has favored the survival of pests and caused a surge in pest infestations, which has in turn led to an increase in the use of synthetic pesticides in agriculture to sustain agricultural productivity (Dang et al., 2017).
An increase in the number of hot days as a result of warming is linked to an increase in the prevalence of renal diseases. Excessive sweating causes dehydration and serum osmolality, thereby leading to excessive concentration of insoluble urinary salts like calcium oxalate. When the concentration of urinary salts reaches the maximum solubility threshold, urinary salts begin to form crystals that become stones (Fakheri & Goldfarb, 2011).
The burden of neurodegenerative diseases is expected to increase as a result of global warming induced by climate change. Warmer temperatures can lead to heat stress, which may trigger biochemical processes that can produce elevated levels of proteins and lead them to accumulate and misfold, thereby stimulating the onset of neurological impairment. Heat stress may also lead to low antioxidant levels and excess production of free radicals, which is associated with mitochondrial dysfunction and neural degeneration. Exposure to heat is also linked to altered immune response and release of neuroinflammatory compounds that aid the progression of neurodegenerative disorders (Bongioanni et al., 2021).
Empirical Rationale
Primary energy may be referred to as any form of energy that is naturally accessible and has not undergone any form of exploitation. Such sources typically include fossil fuels like coal, natural gas and oil, and renewable sources of energy like hydro energy, wind energy, and solar energy. In view of the rapid expansion of three main sectors, namely, industries, buildings, and transport, primary energy consumption has skyrocketed in all regions of the world since the 18th century (Laloui & Loria, 2019). Primary energy consumption may either imply the crude use of primary energy fuels at their source or their untreated supply to users who can facilitate the conversion of such fuels into secondary fuels such as petroleum and gasoline (Hanania & Donev, 2020).
The focus of this Commentary revolves around the case of three economies: the United States, China, and India, selected for three reasons. First, these economies are the largest consumers of primary energy in the world. In 2017, China accounted for 23 percent of global primary energy consumption, making it the largest energy consumer in the world. The United States was the second-largest consumer of primary energy and utilized 17 percent of the total energy consumption in the world. India accounted for 6 percent of global energy consumption, ranking third in primary energy consumption (Wang, Li, et al., 2020). Second, all three economies are on unique levels of economic growth. China is the largest developing country in the world, whereas the United States is the largest developed country in the world (Wang, Li, et al., 2020). In addition, India's economy is expanding rapidly (Wang, Li, et al., 2020). Third, these three economies are the largest carbon emitters in the world, and together contribute to half of the global carbon emissions (Wang, Jiang, et al., 2020).
Primary Energy Consumption and Carbon Emissions
As shown in Figure 1, primary energy consumption was relatively modest for India as compared to the United States and China for the years 1995 and 2017. However, projections for the year 2040 indicate that India will overtake the United States and China in terms of percentage increase in primary energy consumption between 2017 and 2040. Even though India's primary energy consumption is projected to remain considerably lower than that of the United States and China through 2040 in absolute terms, the alarming increase in primary energy consumption that India is projected to register in percentage terms from 2017 to 2040 presents a fundamental concern from the perspective of environment and health systems (BP, 2019, 2020). This is because, unlike the United States and China, India is expected to continue to exploit its fossil fuel reserves for fulfilling its primary energy consumption needs (BP, 2019).
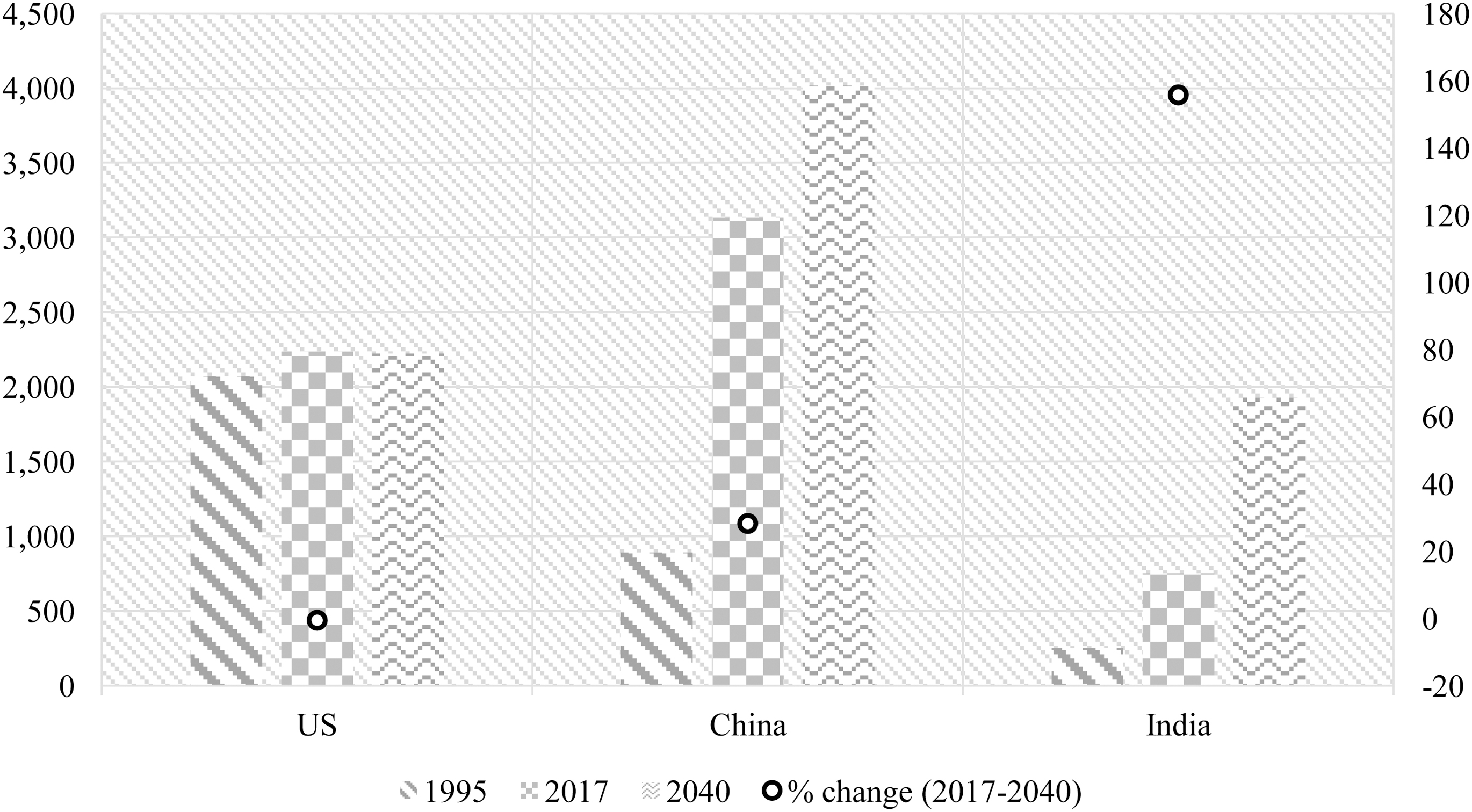
Primary energy consumption (million toe),a 1995-2040
As shown in Figure 2, while China's primary energy consumption using fossil fuels (oil, gas, and coal) is expected to have reached its plateau after 2020, India's fossil fuel-driven primary energy consumption will continue to rise steeply through 2040. China's primary energy consumption will be progressively propelled by renewables and nuclear energy whereas India's increase in primary energy consumption will only be minimally steered by renewables and nuclear energy. The dependence on fossil fuels is going to consistently decline for the United States, while its use of renewables and nuclear energy is expected to increase through 2040, but at a slower pace than China (BP, 2019). It is important to highlight that even though India was the third-largest contributor to net CO2 emissions after China and the United States in 2018, the prevalence of existing trends could make it the second largest CO2-emitting country after China by 2040 (BP, 2019, 2020). India would register the highest percentage increase in net CO2 emissions between 2018 and 2040 (Figure 3).
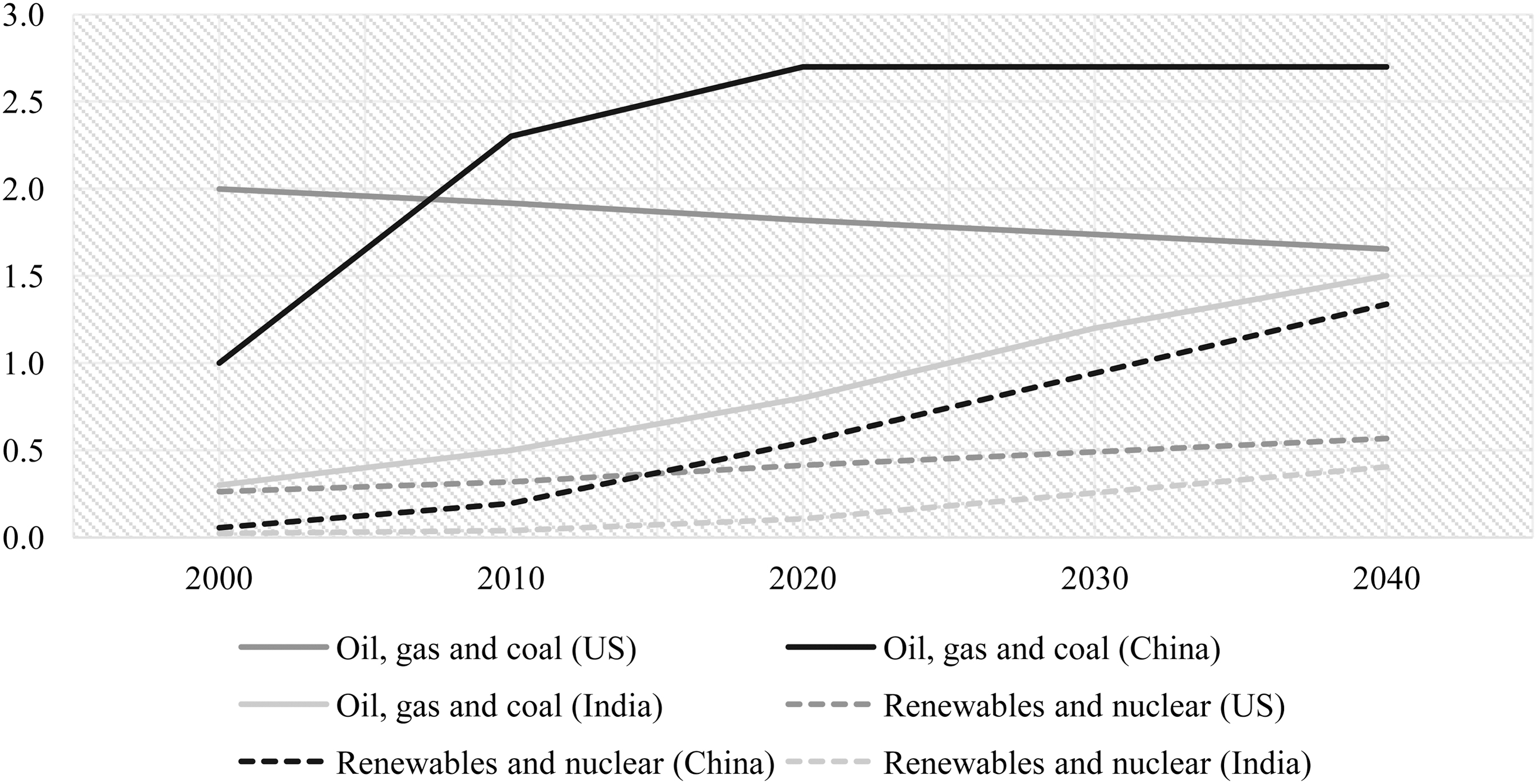
Primary energy consumption by fuel (billion toe), 2000-2040

Net carbon dioxide emissions (million tonnes), 1995-2040
Premature Mortality from NCDs Attributable to PM and Ozon
e
The two countries that have the highest burden of mortality from NCDs attributable to PM and ambient ozone pollution are China and India. As per estimates from the Institute for Health Metrics and Evaluation (2019), despite a lower burden of total deaths caused by NCDs attributable to ambient particulate matter pollution, compared to China, India has had to bear a higher burden of premature mortality; almost 50 percent of NCD deaths attributable to ambient PM pollution occurred among individuals who were under 70 years of age in 2019. In China, in contrast, the share of premature deaths due to NCDs attributable to ambient PM pollution was estimated to be 35 percent. In addition, almost 48 percent of NCD deaths attributable to household air pollution from solid fuels occurred among individuals under 70 years of age, resulting in India's disproportionate burden of premature mortality in this category. Likewise, the share of premature mortality accruing from NCDs attributable to ambient ozone pollution was significantly higher for India compared to China in 2019; nearly 30 percent of NCD deaths attributable to ambient ozone pollution occurred among people under 70 years of age. Since India's share of net CO2 emissions is expected to increase substantially by 2040, the existing human health impact from NCDs attributable to environmental pollutants, namely PM and ambient ozone pollution, could translate into an increasingly sizable burden of premature deaths. Urgent policy interventions are needed to contain the current level of fossil fuel emissions and address the increasing NCD-related death rate.
Policy Priorities: Indian Example
Even though the WHO has identified four main risk factors for NCDs—tobacco use, physical inactivity, harmful use of alcohol, and unhealthy diets (Schwartz et al., 2021) —the contribution of such behavioral risk factors to the aggregate burden of NCDs may vary significantly across different countries. In fact, the United Nations referred to the issue as a global NCD crisis and has called for a response, citing behavioral and environmental risk factors such as air pollution and mental health conditions as contributing factors (United Nations General Assembly, 2018).
As shown in Figure 4, PM and ambient ozone pollution play a more significant role in causing NCD-related mortality in India than internationally recognized behavioral risk factors. However, policies to address the burden of NCDs have perpetually emphasized the need for tackling behavioral risk factors of NCDs primarily through sensitization activities and counseling services (Ministry of Health and Family Welfare, 2017a, 2017b). While addressing behavioral risk factors is an important aspect of primary prevention measures for NCDs, the fact that a substantial proportion of NCD deaths is caused by environmental pollutants calls for a reorientation of strategies in existing national policies. Shifting focus to environmental pollutants should be considered essential because focusing exclusively on behavioral risk factors implicitly puts the onus of poor health outcomes on individuals and disregards the role of public institutions in proactively mitigating health risks (Linou et al., 2018).
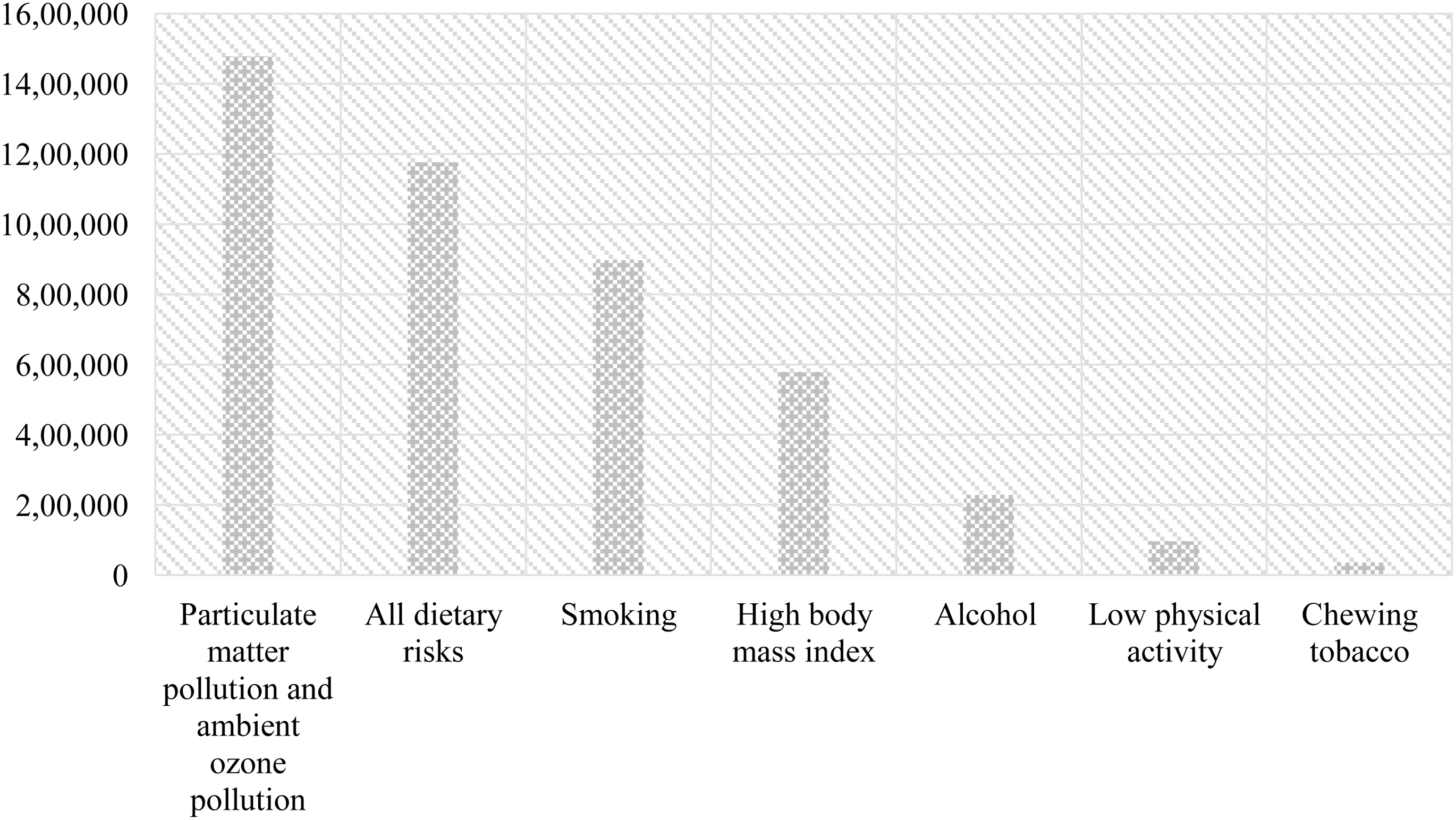
NCD deaths attributable to various risk factors in India, 2019
Even though India has made significant strides with respect to reducing the burden of climate sensitive vector-borne diseases, measures to curb the burden of NCDs caused by environmental pollutants have remained far from adequate. Furthermore, NCD-related schemes have not experienced a significant increase in public sector expenditure, which has resulted in high out-of-pocket expenditures (OOPE). For instance, using data from the 71st round of the National Sample Survey, Kastor and Mohanty (2018) show that OOPE and distress financing is significantly higher for hospitalizations occurring due to NCDs, especially cancers, heart diseases, and genito urinary diseases, as compared to communicable diseases and injuries. Given that the burden of NCDs such as CVDs and cancers would further escalate with the increase in primary energy consumption, it is important to prioritize public spending on NCDs.
Way Forward
Given that primary energy consumption and CO2 emissions are projected to rise and contribute to the existing mortality and morbidity burden, human health should be at the forefront of international deliberations on climate change and sustainability. The consequences of climate change on population health should provide an impetus for geopolitical resolutions on climate action. A global consortium to prevent and address environmental risk factors of NCDs is urgently needed. Specifically, such a consortium should:
Explore possible synergies between health, energy, and meteorological sectors to predict and mitigate the long-term impact of climate change on human health. Energy and environment sectors could also collaborate to identify sustainable solutions to substitute nonrenewable sources of energy with cleaner sources of energy. Since the health care sector is a major contributor to GHGs, the consortium should aim to identify long-term measures in collaboration and consultation with the aforementioned sectors to reduce the carbon footprint of the health care sector. Address the social determinants of health (SDH) from the perspective of reducing morbidity and mortality related to environmental pollutants. Strengthening the SDH involves addressing socioeconomic factors that improve health care outcomes. Approaches to strengthen SDH should involve the establishment of safe housing in neighborhoods that have adequate green cover and walking spaces so as to mitigate the risks associated with environmental pollutants. Furthermore, improving access to education is fundamental to ensure that pollution-related advisories are understood and followed by the general population. Specialized education in fields like green chemistry and public health could play an important role in health promotion and disease prevention. In the long term, enhanced education access could improve per capita incomes and increase community-level action and resilience to pollutants. Create an effective database that can provide evidence of risk factors and pathways that lead to NCDs. Proactive surveillance of NCD-related risk factors could substantially help curtail the burden of NCDs attributed to environmental pollutants by facilitating early diagnosis and treatment. Since primary care is the first point of contact between individuals and health care systems, robust primary care backed by a strong referral system could assume a significant role in this regard. Prioritize research on environmental factors, particularly pollutants, that contribute to NCDs. Local-level vulnerability assessments should routinely collect and compute data on the health vulnerability of population groups to PM and ambient ozone concentrations to identify high-risk populations and develop timely interventions to address their health risks.
The integration of human health and NCDs into climate change discourses is crucial. Countries need to commit to reducing the burden of NCDs associated with environmental pollutants in international conventions on climate change and sustainability, while also reinforcing their commitment to reducing GHGs.