
Abstract
Chronic spinal cord injury (SCI) is characterized by tissue loss and a stable functional deficit. While several experimental therapies have proven to be partly successful for the treatment of acute SCI, treatment of chronic SCI is still challenging. We studied whether we can bridge a chronic spinal cord lesion by implantation of our newly developed hydrogel based on 2-hydroxypropyl methacrylamide, either alone or seeded with mesenchymal stem cells (MSCs), and whether this treatment leads to functional improvement. A balloon-induced compression lesion was performed in adult 2-month-old male Wistar rats. Five weeks after injury, HPMA-RGD hydrogels [N-(2-hydroxypropyl)-methacrylamide with attached amino acid sequences—Arg-Gly-Asp] were implanted into the lesion, either with or without seeded MSCs. Animals with chronic SCI served as controls. The animals were behaviorally tested using the Basso–Beattie–Breshnahan (BBB) (motor) and plantar (sensory) tests once a week for 6 months. Behavioral analysis showed a statistically significant improvement in rats with combined treatment, hydrogel and MSCs, compared with the control group (P < 0.05). Although a tendency toward improvement was found in rats treated with hydrogel only, this was not significant. Subsequently, the animals were sacrificed 6 months after SCI, and the spinal cord lesions evaluated histologically. The combined therapy (hydrogel with MSCs) prevented tissue atrophy (P < 0.05), and the hydrogels were infiltrated with axons myelinated with Schwann cells. Blood vessels and astrocytes also grew inside the implant. MSCs were present in the hydrogels even 5 months after implantation. We conclude that 5 weeks after injury, HPMA-RGD hydrogels seeded with MSCs can successfully bridge a spinal cord cavity and provide a scaffold for tissue regeneration. This treatment leads to functional improvement even in chronic SCI.
Introduction
S
Chronic SCI is characterized by a stable, permanent functional deficit. However, according to several studies [6 –10], progressive injury is observed, including the delayed death of neurons and oligodendrocytes, axonal demyelination of intact fiber tracts, and retrograde tract degeneration even years after SCI in both experimental animals as well as in humans [10 –12]. Further, there is evidence of supraspinal alterations following SCI [13 –16].
Hydrogels are cross-linked hydrophilic polymers. In SCI repair, they serve as a bridge for axonal growth across the lesion cavities, and with their 3-dimensional porous structure, they provide an acellular mechanical framework for the regeneration of neural tissue [17]. In several studies [18 –23], hydrogels were shown to bridge a spinal cord lesion and promote tissue regeneration. While most studies evaluated the efficacy of hydrogels in acute SCI repair, there are also a few studies demonstrating that hydrogel implantation can lead to functional improvement and tissue reconstruction even in rats with chronic SCI [24].
Mesenchymal stem cells (MSCs) are pluripotent progenitor cells that can be attracted to a damaged site, where they secrete bioactive factors that trophically influence repair and regenerative processes [25]. The use of MSCs in cell therapies may have some advantages over the use of other sources of cells: they are relatively easy to isolate, they may be used in autologous transplantation protocols [26], and bone marrow as a source of cells has been already approved for the treatment of hematopoietic diseases. It was shown that transplanted human MSCs have the ability to increase the expression of growth and trophic factors in the ischemic rat brain [27]. Further, when MSCs are injected either intravenously or into a spinal cord lesion site 7 days after SCI, they improve behavioral outcome and prevent tissue loss [4,28]. In chronic SCI, the results have been, however, less promising [26,29].
As SCI research progresses, it becomes clear that combined therapies will play a major role in future experimental and clinical approaches. Recently, several attempts were made to create cell–polymer constructs with genetically engineered cells [30] or with stem cells [31] to provide a biohybrid system for tissue bridging in cases where a large tissue defect exists.
In our study, we evaluated whether implanting a hydro-gel based on poly N-(2-hydroxypropyl)-methacrylamide (PHPMA) with an attached oligopeptide sequence (RGD), either alone or seeded with allogenic MSCs, 5 weeks after SCI improves motor or sensory function in rats and whether such an approach can prevent secondary tissue damage.
Materials and Methods
Animals
We used 40 male Wistar rats (Velaz, Prague, Czech Republic) with body weight 300–330 g. This study was performed in accordance with the European Communities Council Directive of November 24, 1986 (86/609/EEC) regarding the use of animals in research and was approved by the Central Commission for Animal Protection of the Academy of Sciences of the Czech Republic in Prague.
Design of the study
Animals with chronic SCI were randomly divided into 3 groups 5 weeks after SCI: (1) animals treated by hydrogel implantation (n = 13), (2) animals treated by the implantation of a hydrogel seeded with MSCs (n = 12), and (3) untreated animals (n = 15). Behavioral testing was performed 1 day before and after SCI and then each week (same day, same hour) for 6 months by 2 independent testers in a blinded fashion. The numbers in each group represent the animals that survived the whole 6-month experiment; some animals were lost during the lesioning procedure, while a few animals died due to urinary infection during the later part of the experimental period. All animals that died prior to 6 months were excluded from further analysis.
Chronic spinal cord injury after a balloon-induced compression lesion
After the induction of anesthesia with 5% isoflurane in room air (flow 300 mL/min), animals were maintained in 3% isoflurane anesthesia (flow 300 mL/min) via a face mask throughout the operation. A lower concentration of anesthesia was not used in order to avoid neurogenic pulmonary edema [32]. All animals were heated to 37°C, and their body temperature was measured by a rectal thermometer to standardize the procedure and to exclude the influence of hypo- and hyperthermia [33,34]. For SCI, we used the model of an epidural balloon-induced compression lesion, as described in detail previously [35]. In brief, a 2-cm midline skin incision over the spinous processes of Th10-L1 was made under aseptic conditions. The muscles were detached from the laminae and retracted to the sides with a retractor. A small hole was drilled in the Th10 lamina using a tooth drill. A 2-French Fogarthy catheter (Baxter Healthcare Corporation, Irvine, CA) was inserted 1 cm upward into the epidural space at the Th8–9 level. A spinal cord lesion was made by balloon inflation (volume 15 μL). Inflation for 5 min produced complete SCI with paraplegia. The catheter was then deflated and removed. Soft tissues and skin were sutured in anatomical layers. Bladder expression was performed until the recovery of sphincter control, and gentamicin was administered i.m. for 5 days to prevent urinary infection.
Implantation of a hydrogel inside a balloon-induced compression lesion
The surgery was performed under pentobarbital (PTB) anesthesia (60 mg/kg). The animals were injected with gentamicin (0.05 mL i.m.) and mesocain (0.3 mL s.c. at the surgery site) as analgesia during the surgery and atropine (0.2 mL, atropine solution 1:5). Under aseptic condition, a linear 3-cm midline skin incision was made over the Th7–11 spinous processes. The paravertebral muscles were dissected from the vertebral laminae. A Th7–10 laminectomy was performed, adjusting the level of the laminectomy based on MRI images that were acquired 1 day before surgery and on the actual size of the compression lesion as seen perioperatively. After ensuring proper hemostasis, a longitudinal durotomy was performed over the lesion and the dura mater was suspended with a 10/0 thread. A 2–3 mm incision (dorsal myelotomy) was performed at the point where the pseudocystic cavity was closest to the dorsal surface (based on preoperative MRI) in order to minimize further injury to the spinal cord until we reached the cavity. The cellular debris was cleared from the cavity. The size and shape of the hydrogel implant was adjusted to assure complete bridging of the cavity with minimum undue pressure on the surrounding spinal cord tissue. The average volume of the implanted scaffold was about 2 mm3. The dura mater was sutured with a 10/0 monofil unresorbable thread (B Braun, Aesculap AG & CO. KG, Germany). The muscles and skin were sutured with a 4/0 monofil unresorbable thread (4/0 Chirmax, Czech Republic). The animals treated with hydro-gel and MSCs received cyclosporine (Novartis, 10 mg/kg i.p.) daily for 1 month postoperatively. All animals were kept in cages with food and water ad libitum.
Behavioral testing of animals
All animals were allowed to survive for 6 months post-injury. Hind limb performance was evaluated using the Basso–Beattie–Bresnahan (BBB) open-field locomotor test [36]. Sensation in the hind limbs was determined according to the latency (in seconds) of hind limb withdrawal from thermal stimulation using the plantar test (Ugo Basil, Comerio, Italy), as described previously [4]. Two independent observers performed the BBB and plantar tests for 5 days before injury for adaption, at 24 h after injury and then once a week throughout the survival period.
Chemicals
[2-(Methacryloyloxy)ethyl]trimethylammonium chloride (MOETACl) was prepared by a method described previously [37]. The synthesis of N-2-hydroxypropyl methacrylamide (HPMA) was also described previously [38].
Peptide synthesis
The oligopeptide [methacryloyl-glycine-glycine-arginine-glycine-aspartate (MA-GG-RGD)] was prepared using a solid phase peptide (SPPS) method, with methacryloylation as the last step. After completing the synthesis, the peptide was cleaved from the resin and deprotected using a mixture of 95% trifluoroacetic acid (TFA), 2.5% triisopropylsilane (TIS), and 2.5% water. After evaporation of the cleavage and deprotecting mixture, the peptide was precipitated in cold ether (0°C), filtered, and dried under vacuum. The MA-GG-RGD was then purified on HPLC with a UV detector (separative column C18), dried and dissolved into distilled water, and lyophilized. The purity of the cleaned product was measured on MALDI-TOF (MS 529.7 (M+H)) and a HPLC-UV detector (separative column C18, retention time 8.4 min) and found to be 95%.
Hydrogel synthesis
Macroporous hydrogels were prepared by the radical precipitating polymerization of monomers (HPMA, 0.08 mol%, MOETACl, 0.08 mol%, MA-GG-RGD, 2.6 wt%) with the cross-linking agent methylenebis(acrylamide) (MBAA) and the initiator azobis(isobutyronitrile) (AIBN), 0.3 wt%, in a solvent/precipitator mixture (dimethyl sulfoxide/acetone, 10 g in a ratio of 1/13) under a nitrogen atmosphere in a sealed glass ampule at 50°C for 16 h. After polymerization, the macroporous hydrogel was removed from the ampule and washed in a laminary box with absolute ethanol (3 times for 1 day each), 50% ethanol/water (3 times for 1 day each), distilled water (3 times for 1 day each), 0.5% NaHCO3 in water (for 1 day), distilled water (5 times for 1 day each), and saline (once a day for 5 days).
The hydrogels were macroporous; the communicating (interconnecting) pore fraction of the hydrogel was determined by immersing a dry xerogel in heptane and determining the weight of the heptane that penetrated into the communicating pores. Based on these measurements, 38% of the porous hydrogel was formed by pores, and 95% of these pores are communicating. The estimated water content, which was determined from the weight of the xerogel and the gel swollen to equilibrium, was between 85% and 90%. The mechanical properties of the resulting macroporous structure mimick those of the rat nervous tissue, and all of the properties were generally similar to those of HPMA hydrogels already published [21]. The morphology of the hydrogels was visualized by scanning electron microscopy (SEM). A hydrogel (after washing with water) was lyophilized and fractured, then the surface was sputtered with platinum and observed using high-vacuum SEM (Fig. 1).
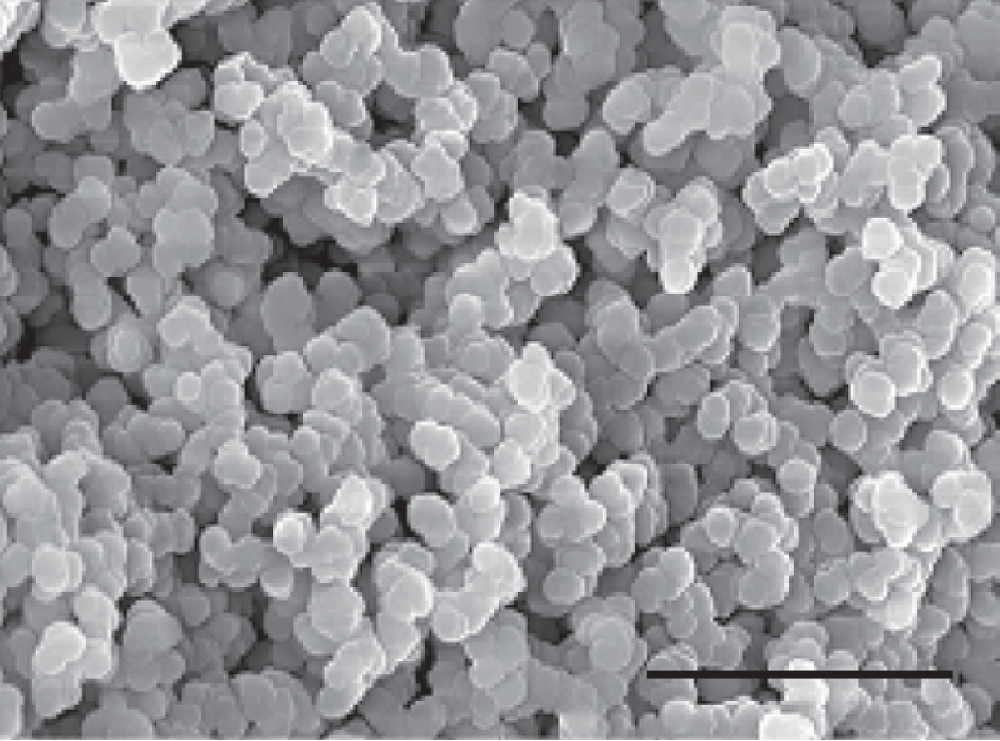
Scanning electron microscopy (SEM) of the N-(2-hydroxypropyl)-methacrylamide with attached amino acid sequences—Arg-Gly-Asp (HPMA-RGD) hydrogel in vitro. The structure of the hydrogel consists of ball-like particles with heterogeneous pores in between. Scale bar, 10 μm.
Seeding rat mesenchymal stem cells on hydrogels
To enable more easily distinguishable and stable tracking of transplanted cells, rat MSCs (rMSCs) expressing enhanced green fluorescent protein (GFP) isolated from GFP+ rats were used in our experiments. The transgenic Sprague-Dawley rats [SD-Tg(CAG-EGFP)CZ-004Osb] were kindly provided by Dr. Masaru Okabe (Osaka University, Japan) [39], bred at the laboratory of Dr. Martin Marsala (University of California, San Diego, CA), then subsequently sent to our Institute and bred in our animal facility. The cells were isolated by extrusion into a tissue culture Petri dish. The cells were characterized as follows: adherence to plastic, positive FACS staining for CD34, CD45, CD235a, and CD271, and negative FACS staining for CD29, CD44, CD73, CD90, and CD105. They were also tested for their ability to differentiate into adipocytes, chondrocytes, and osteocytes. For the full characteristics of MSCs, see Dominici et al. [40]. The cells were plated in DMEM/10% fetal bovine serum (FBS) with primocin (2 μL/mL). After 24 h, the nonadherent cells were removed by replacing the medium. On the day of hydrogel implantation, the cultures were trypsinized with a 0.25% trypsin/ethylenediaminetetraacetic acid (EDTA) solution. Then, 2 million cells per milliliter were placed in a test tube together with a 2 × 2 × 2 mm cube of hydrogel and put on a shaker (500 rpm) for 15 min in order to seed the 3D scaffold.
Magnetic resonance imaging
To determine the lesion size before hydrogel implantation and to evaluate the development of the lesion, animals were examined using an experimental MR spectrometer (Bruker Biospec 47/20, 4.7T, 20 cm room temperature bore) equipped with a 200 mT/m gradient system and a custom-made half-saddle coil for spinal cord imaging. Animals were anesthetized with a 1.5% isoflurane mixture in air through a breathing mask, positioned in a PVC-U animal bed, and fastened with surgical tape in a prone position. The coil was centered in the magnet, and the animal bed was positioned within the coil. The precise position was then adjusted according to localizer scans if necessary. Spontaneous breathing was monitored through a Graseby respiration sensor (Graseby, UK) connected to an EKGHR2 monitor (Rapid, Germany). The respiration signal was also used to trigger all MR acquisitions. T2-weighted sagittal (and coronal) RARE images were recorded in 2 successive experiments in an interleaved fashion to minimize the influence of neighboring slices (matrix 256 × 160, FOV 5 × 3 cm, slice thickness/gap 0.5/0.5 mm, TE/TR = 70/1,400 ms, RARE factor 16, 16 averages). T2-weighted axial RARE images with fat saturation were also acquired in an interleaved fashion (matrix 256 × 128, FOV 4 × 2 cm, slice thickness 0.5 mm, slice gap 0.5 mm, TE/TR = 36/2,000 ms, RARE factor 8, 16 averages).
Retrograde tracing
Six months after SCI, under isoflurane anesthesia, a laminectomy of the lumbar vertebra 12 and 13 was performed, and 2 μL of 2% hydroxystilbamidine (Fluorogold, Invitrogen, Carlsbad, CA) were stereotactically injected by a Nano-Injector (Stoelting Co., Wood Dale, IL) into the dorsal columns of 5 animals treated with hydrogel and MSCs. Two days later, the animals were perfused transcardially with phosphate-buffered saline (PBS) followed by 4% paraformal-dehyde. Sections were first incubated with anti-fluorogold antibody (1:10,000; Chemicon International, Temecula, CA) then with biotinylated goat anti-rabbit secondary antibody (1:1,000; Vector Labs, Burlingame, CA). They were processed using Vectastain ABC reagent (Vector Labs) and developed with diaminobenzidine (Vector Labs).
Tissue processing and histology
Six months after SCI, the animals were deeply anesthetized with an intraperitoneal injection of overdose PTB and perfused with physiological saline followed by 4% paraformaldahyde in 0.1 M phosphate buffer. The spinal cord was left in bone overnight, then removed and post-fixed in the same fixative for at least 1 week. A 3-cm long segment of the spinal cord containing the lesioned site was dissected out, and a series of 16-μm thick longitudinal sections was collected. Hematoxylin–eosin, Luxol Fast Blue, and Cresyl Violet stainings were performed using standard protocols. For immunohistological testing antibodies directed against the following markers were used: GFAP (1:200; Sigma-Aldrich, St. Louis, MO) to identify astrocytes, NF 160 (1:200; Sigma-Aldrich) to identify neurofilaments, p75 (1:100; Chemicon International, Temecula, CA) to identify Schwann cells, RECA-1 (1:50; Abcam, Cambridge, MA) to identify endothelial cells of blood vessels, GAP-43 (1:5,000; Chemicon International) to identify regenerating neurons, and CGRP (1:2,000; Chemicon International) to identify sensory axons. Alexa Fluor 488 goat anti-rabbit IgG (1:200; Invitrogen, Carlsbad, CA), Cy3-conjugated mouse anti-glial fibrillary acidic protein (1:100; Chemicon International), and Alexa Fluor 594 goat anti-rabbit IgG (1:500; Invitrogen) were used as secondary antibodies.
Transmission electron microscopy
Spinal cords were longitudinally cut in 60-μm slices and then transferred onto gelatin-coated coverslips, fixed in 2.5% glutaraldehyde in 0.1 M Sörensen buffer, and stained by 1% osmium tetraoxide in 0.1 M Sörensen buffer for 2 h. Spinal cord slices were then dehydrated in ethanol, immersed in propylene oxide, and flat-embedded in Epon 812 using gelatin capsules. After polymerization for 72 h at 60°C, cover-slips were removed by liquid nitrogen. Ultrathin sections of 65 nm were examined with a Philips Morgagni 268D transmission electron microscope (FEI Inc., Hillsboro, OR).
Tissue atrophy evaluation
We evaluated spinal cord tissue atrophy around the epicenter of the lesion. In each of the 3 experimental groups, 7 spinal cords were randomly chosen. We measured the cross-sectional areas at 2 locations in the spinal cord—6 mm cranial and caudal to the epicenter of the lesion. Longitudinal sections 16-μm thick were used, and every third section was measured. Ten normal spinal cords were used to evaluate the normal cross-sectional area of the rat spinal cord at the Th8–9 level. We used Image J software to calculate the cross-sectional area (Microsoft Java 1.1.4.).
Statistical analysis
The mean values are reported as mean ± SEM. Intergroup differences were analyzed using one-way ANOVA with post-hoc LSD test (P < 0.05). Morphometric measurements were used to construct plots of consecutive cross-sectional areas of the spared tissue at individual levels of the spinal cord rostral and caudal to the epicenter. The differences at each level were analyzed using the Kruskall–Wallis and Mann–Whitney U-tests. Statistically significant differences (P < 0.05) are marked in figures by asterisks.
Results
Behavioral testing
Motor score
All the animals had normal motor function of their hind limbs before SCI (BBB = 21 ± 0). After SCI, the animals were paraplegic (BBB = 0.3 ± 0.1). Over the course of 5 weeks, the animals gradually improved so that they were able to move extensively all 3 joints of their hind limbs without weight support (BBB = 7.4 ± 0.68). At 5 weeks, the animals were divided into 3 groups (SCI only, SCI+hydrogel, and SCI+hydrogel+MSCs). Animals in the control group did not show marked further improvement by the end of the 6 months observation period (BBB = 8.2 ± 0.8). From week 8 after SCI, the animals treated with hydrogel implantation showed a gradual but not statistically significant improvement. At 6 months after SCI, they showed plantar placement of the paw with weight support in stance only (BBB = 9.5 ± 1.0). The animals treated with hydrogels seeded with MSCs showed a gradual improvement in the motor function of their hind limbs, which was significantly better at about 5 months than that in animals with SCI only (P < 0.05, Fig. 2A). Their hind limbs showed occasional weight-supported plantar steps (BBB = 10.0 ± 0.6).

Functional evaluation (motor and sensory). (
Sensory score
The plantar score measures the time that is required for an animal to withdraw its paw when stimulated with heat. The reaction time (measured before SCI) was below 7 s (6.9 ± 0.4 s). The reaction time at 5 weeks post-SCI was 10 s (10.0 ± 0.6 s). Further, the animals were divided into 3 groups. In the SCI group, the reaction time slowly decreased to a time of 9 s at week 15 and remained stable for the next 11 weeks (8.45 ± 0.49). In the hydrogel-treated group, there was also a slight decrease in the reaction time after implantation; at 6 months after SCI, the animals had a reaction time 7.8 ± 0.69 s, without reaching a statistically significant difference. In the hydrogel+MSC-treated group, there was a statistically significant improvement in the reaction time 7 and 8 weeks posttreatment (hydrogel+MSCs implantation). This reaction time improvement became stable from week 17 until the end of the study, 25 weeks after SCI (5.4 ± 0.3 s, P < 0.05; Fig. 2B).
MRI evaluation
Two days after SCI, the spinal cord in the epicenter of the lesion was edematous as indicated by a hyperintense signal in T2-weighted images. There was no demarcated lesion apparent. One week after SCI, edema was still present. An area with a hyperintense signal without a well-demarcated border appeared (Fig. 3A and 3B). Three weeks after SCI, the lesion became demarcated. Signs of atrophy were apparent as indicated by an enlarged subarachnoid space (Fig. 3C and 3D). From 4 to 6 weeks after SCI, significant atrophy was present in the epicenter of the lesion, which was especially apparent in axial scans. A pseudocystic cavity or cavities in the center, with a well-demarcated border, became visible 4 weeks after injury, and the lesion was quite well demarcated (Fig. 3E and 3F). The epicenter of the spinal cord showed severe atrophy with pseudocystic cavities half a year after SCI (Fig. 3G and 3H). One week after implantation of the hydrogel inside the cavity, the signal of the hydrogel was hyperintense with a fuzzy border (Fig. 3I and 3J). The intensity of the hydrogel signal was lower than that of a developed pseudocystic cavity. However, 6 months after implantation, when the hydrogel was infiltrated with regenerating tissue, the hydrogel became isointense compared to the surrounding nervous tissue (Fig. 3K and 3L).

Spinal cord lesion development on MRI (sagittal and axial scans). (
Spinal cord tissue atrophy
The average cross-sectional area of the rat spinal cord at the Th8–9 level is 3.34 ± 0.29 mm2, while in spinal cords 6 months after SCI, 6 mm cranial and caudal to the lesion, the average cross-sectional area was 1.59 ± 0.16 mm2 in the group of SCI only, 2.05 ± 0.32 mm2 in SCI treated with hydrogels, and 2.68 ± 0.48 mm2 in SCI treated with hydrogels seeded with MSCs (Fig. 4). Animals with chronic SCI treated with hydrogel seeded with MSCs had a statistically significantly larger amount of spared spinal cord tissue in the perilesional area compared to animals with chronic SCI only (P < 0.05).

Tissue atrophy at the lesion site. The graphs represent the cross-sectional areas of the residual spinal cord tissue at 6 mm cranial and caudal to the epicenter of the lesion (excluding hydrogel). Asterisk indicates significant difference compared to spinal cord injury (SCI)-only animals (P < 0.05).
Histological evaluation of the lesion
Animals with SCI
In animals with SCI only, the center of the lesion was atrophic, dominated by several pseudocystic cavities with astrocytic scarring. There were cavities in the center of the lesion after 5 weeks (Fig. 5A), which progressed 6 months after SCI (Fig. 5B). Astrocytes constituted a dense network at the lesion site, forming an astrocytic scar around the epicenter (Fig. 5C). Residual axons were present in the remaining cellular debris in the pseudocystic cavities (Fig. 5D).
Evaluation of the lesion in animals with chronic spinal cord injury (SCI) 5 weeks and 6 months after SCI. (
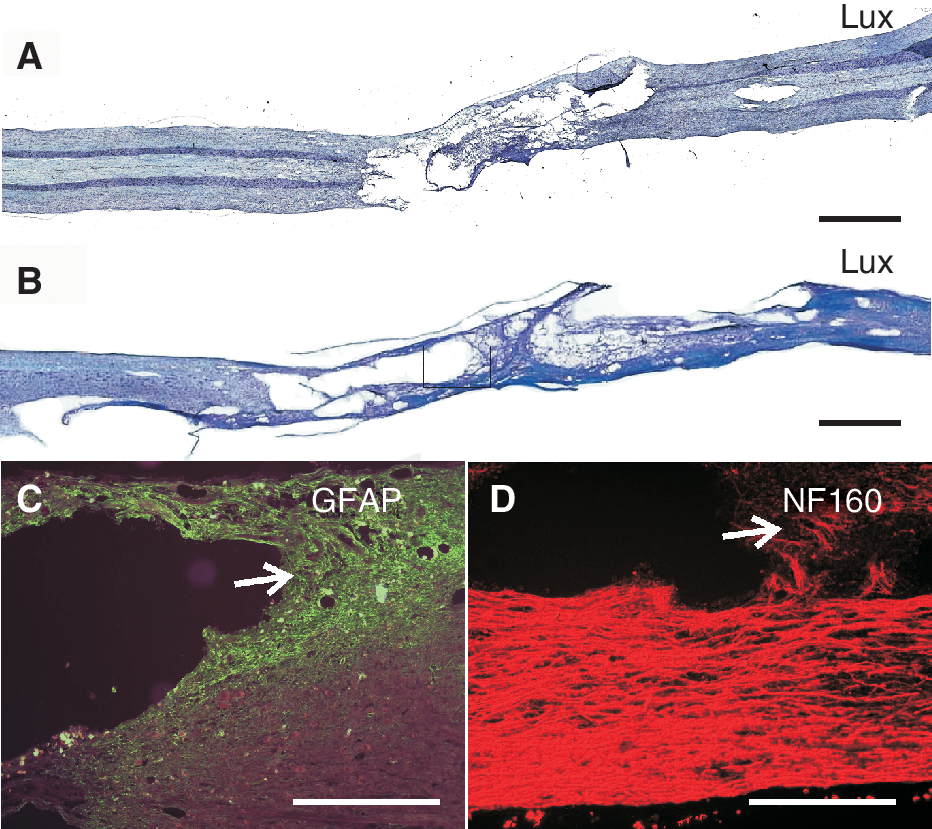
Hydrogels and hydrogels seeded with MSCs
The hydrogels in both implanted groups formed a bridge across the cavity. They adhered well to the surrounding tissue. We did not observe any signs of foreign body reaction. The pores of the hydrogels were infiltrated with connective tissue elements and formed a bridge across the lesion site (Fig. 6A). During the growth of the cells within the hydrogel, we observed a dislocation of the hydrogel structure caused by the cell growth. The morphology of the hydrogels slightly changed due to irregularities in cell growth; for example, the ingrowing vessels “pushed away” the hydrogel and interactively shaped the hydrogel's morphology to provide better cellular ingrowth (Fig. 6B). Axons grew inside the hydrogel implants in both treated groups and were found in the peripheral as well as in the central parts of the implant (Fig. 6C). The hydrogel therefore served as a scaffold for axonal infiltration. GAP-43 staining showed massive regeneration of the central nervous system (CNS) axons (Fig. 6D). Axons grew from the rostral as well as caudal parts of the surrounding spinal cord tissue and infiltrated the hydrogel bridge. They grew into the peripheral part of the hydrogel and further into the central part, thus infiltrating the whole volume of the implant (Fig. 6E). Also Schwann cells infiltrated the whole volume of the hydrogel implant (Fig. 6F). They grew from the spinal root entry zone toward the implant (Fig. 6G) Many Schwann cells grew in close contact with axons (Fig. 6H). The Schwann cells formed a myelin sheath around the axons infiltrating the hydrogel (Fig. 6I). Retrograde staining proved that the source of the axons infiltrating the hydrogel were CNS neurons (Fig. 6J). Also, several sensory neurons (CGRP-positive) were found infiltrating the hydrogel (Fig. 6K). Astrocytes and their processes created a dense astrocytic scar around the hydrogel implant. Many astrocytic processes crossed the border between the spinal cord and the implant, infiltrating the peripheral parts of the hydrogel and forming quite a dense network inside the hydrogel as well (Fig. 6L). At 6 months after implantation, astrocytes were also found in the central part of the scaffold, where they created a loose network. MSCs were found inside the hydrogel implants 6 months after SCI. MSCs were not only identified in the pores of the hydrogel (Fig. 6M), but also some MSCs were found in the spinal cord tissue adjacent to the hydrogel implant (Fig. 6N), as far as 1 mm into the spinal cord tissue. Many regenerating blood vessels growing inside the hydrogel implant were found in the close vicinity of the seeded MSCs (Fig. 6O, arrow indicates a blood vessel).

Evaluation of the lesion in animals treated with a hydrogel seeded with mesenchymal stem cells (MSCs) 6 months after spinal cord injury (SCI). (
Discussion
Despite the evident progress in experimental research, SCI still remains an untreatable condition. Particularly, there is no effective treatment for patients with chronic SCI. Therefore, patients with SCI could benefit from even a minor improvement in their clinical status. In the present study, we found that hydrogels seeded with MSCs provide functional improvement when implanted into a contusion lesion 5 weeks after SCI. Our results show that combined treatment using an HPMA-RGD hydrogel seeded with allogenic rMSCs: (1) improves motor and sensory function; (2) reduces tissue loss; (3) provides a scaffold for axonal regeneration and myelination; and (4) stimulates delayed astrocytic infiltration. Further, the hydrogel serves as a long-term stem cell carrier.
A proper experimental model of SCI together with an appropriate therapeutic window is necessary to mimic the real clinical situation if we wish to transfer experimental data to human SCI repair. Most spinal cord injuries in humans are the result of a combination of compression and contusion, rather than section, the most common experimental model used in hydrogel implantation studies [11,41]. A balloon-induced compression lesion [35], therefore, more accurately mimics human SCI and, in addition, requires minimal surgical intervention before the hydrogel implantation. Further, any use of an artificial material in a clinical setting would require a delay of several days or even weeks after the initial impact, when the injury and the functional status become stable. A therapeutic interval of hydrogel implantation 5 weeks after SCI, when the spinal cord lesion as well as the functional status of the animal became fairly stable, was therefore applied in this study.
Hydrogel bridge
One of the goals of tissue engineering is to develop a material that would provide a bridge across the lesion cavity in order to reconnect the disrupted axons [42]. This approach may be especially beneficial for patients with chronic spinal cord injuries, in whom stem cell therapy alone may not be sufficient for functional improvement [26]. Several studies have shown that hydrogels can provide a scaffold for tissue regeneration and improve functional outcome in acute SCI repair [21,23,43]. However, there have been only a few studies evaluating the effect of hydrogel implantation in chronic SCI repair [24,44]. In the study of Woerly and colleagues, a hydrogel implanted 3 months after SCI improved the functional outcome in animals with SCI but only when combined with an enriched environment [24]. In another study, chitosan guidance channels containing peripheral nerve grafts were implanted in a 50-g clip injury either subacutely (1-week post-injury) or in the chronic phase (4 weeks post-injury). In both treated groups the implants contained a high number of myelinated axons; however, with no statistically significant effect on the functional outcome of the animals 3 months after implantation [44]. In our study the animals in the control group reached a BBB score of eight 9 weeks after SCI, with no change for the next 16 weeks. In contrast, both treated groups showed a gradual improvement following hydrogel implantation, and the hydrogel+MSCs-treated group showed a statistically significant improvement in both motor and sensory functions of the hind limbs without an enriched environment. In this group, the animals showed gradual improvement in both motor and sensory tests, not reaching a plateau even at the end of the monitoring period. Our therapy thus extended the functional recovery period from 2 months to more than 6 months following SCI. It would be useful to perform further studies with a longer monitoring period, as further functional improvement may be apparent 1 to 2 years after SCI.
Preventing tissue loss
A phenomenon that adds to the complexity of regenerative failure is the process of progressive cavitation in which, after days to weeks, a CNS injury in the epicenter can expand in size, resulting in the formation of a scar-encapsulated cavity many times the size of the initial wound [45]. Although various hypotheses about this pathophysiology have been suggested [45 –48], the mechanisms that lead to cyst formation are still poorly understood.
Several therapeutic approaches employing different mechanisms were found to reduce tissue loss either in the acute or the chronic stage of SCI [4,18,43,49]. In our previous study, we found that delaying hydrogel implantation by 1 week in a transection model of SCI improves hydrogel integration and reduces pseudocystic cavities, thus preventing secondary tissue loss, compared to acute treatment [18]. We also showed that treating animals 7 days after the induction of a balloon-induced compression lesion with either MSCs, a freshly prepared mononuclear fraction of bone marrow cells, or G-CSF increases the spared white matter volume in the lesion area [4]. Implanting a hydrogel seeded with neural stem cells prevented secondary tissue loss and thus improved functional outcome [43]. In our study we found that implantation of a hydrogel seeded with MSCs prevented secondary tissue loss, leading to increased tissue volume. We can speculate that the hydrogel provided a scaffold for tissue infiltration, while MSCs provided neurotrophic support, thus preventing progressive cavitation.
Progressive tissue loss can be observed using noninvasive techniques such as MRI even in the chronic stages of SCI [50]. In our study, we also found that MRI can be useful for the noninvasive monitoring of spinal cord lesion development. Further, MRI was used as a noninvasive navigation tool for proper hydrogel implantation. MRI scans in all 3 planes were used to direct the incision for hydrogel implantation and to adjust the size of the hydrogel.
Astrocytic scarring around the lesion after SCI
The role of astrocytes in normal CNS architecture and function is well established; views of the role of reactive astrocytes, on the other hand, have been changing in recent years. While in the early years it was thought that reactive astrocytes represent an inhibitory mechanism in CNS regeneration, more recent studies have shown that reactive astrocytes may indeed protect the tissue and contribute to spontaneous functional recovery, at least to some extent, during the first weeks after injury [51]. Further, astrocytes clear glutamate and potassium ions from the extracellular space, are a potential energy source, and produce numerous growth factors and cytokines [52,53]. In our previous studies, a minimal number of astrocytes infiltrated the hydrogel implants [17,18,54]. In this study, astrocytes were found infiltrating not only the peripheral parts, but also the central parts of the implant. This is, in our experience, the first time that astrocytes have infiltrated the pores of the hydrogels to such an extent, but only 5 months after hydrogel implantation. They created a loose network in the center of the implant, rather than forming a dense gliotic scar. Astrocytes react to central nervous system lesions [55] or implantations [56,57] by proliferation, hypertrophy, and migration around the lesion site, forming a glial scar. Glial scars are generally considered to hinder axonal regrowth, physically by constituting a barrier and chemically by providing molecular conditions nonpermissive for axonal regrowth [56,58]. On the other hand, implanting a hydrogel with MSCs provides a permissive environment for axonal ingrowth. It is further hypothesized that activated astroglia may benefit the damaged nervous system by participating in several important biologic processes such as the regulation of neurotransmitter levels, the repair of the extracellular matrix, control of the blood–CNS interface, transport processes, and trophic support of other CNS cells [59]. From our study, it is clear that long-term evaluation periods would be necessary to properly evaluate the relationship between the implant and the astrocytes.
Schwann cells myelinate regenerating axons inside the implant
Endogenous Schwann cells originating from the dorsal and ventral roots invade and migrate into the injured spinal cord [60]. In our study, we demonstrated that Schwann cells grow from the spinal root entry zone into the spinal cord and invade the hydrogel. They infiltrate the entire volume of the bioimplant and myelinate the regenerating axons. Our finding is in accordance with the studies of other groups [24]. Further, the implantation of Schwann cells improved functional recovery and supported tissue regeneration after SCI [61,62]. Overall, the presence of Schwann cells inside the lesion, or inside the hydrogel in our case, seems to improve both functional and morphological results in SCI repair.
Implantation of mesenchymal stem cells inside a spinal cord lesion
Preclinical studies have been performed on rats with a SCI, including the use of iron oxide nanoparticles to follow the migration and fate of transplanted cells, and have shown that MSCs transplanted into the injured spinal cord survive, migrate into the host tissue, and lead to axonal regeneration and motor function recovery [25,63 –72]. This has been achieved not only through the implantation of bone marrow stromal cells, but also through the implantation of freshly collected bone marrow-nucleated cells with a relatively small percentage of mesenchymal cells [4,67,68]. Two clinical studies so far have shown the safety of such an approach [26,73]. Despite partial improvement of function in acute patients, larger-scale trials are necessary in order to draw any definite conclusions.
Treatment with cyclosporine significantly improves the survival of MSCs in our grafts (unpublished data); therefore, we used this protocol although there is some evidence that cyclosporine may be neuroprotective; however, this has not been clearly proven, and there are many studies showing that cyclosporine has no effect on neuroprotection [74 –76].
MSCs have been used in experimental SCI repair either alone or in combination therapies. Seeding MSCs on a bio-implant, a hydrogel in our case, is advantageous for several reasons. First, the hydrogel serves as a carrier for the MSCs, which are thus delivered to the site of injury. It serves, therefore, as a tool for local stem cell delivery. Some studies have shown that local treatment with MSCs is more effective compared to systemic application [77]. Further, there are fewer studies showing effective treatment in chronic SCI as compared with acute or subacute SCI. Only one experimental group used allogenic MSCs in the therapy of animals with chronic SCI with success [78,79]. Intralesional application of MSCs 3 months after SCI led to motor function improvement and tissue regeneration. Nonetheless, bridging a chronic lesion, despite these results, is still challenging. One of the reasons could be the fact that in the chronic stage, the epicenter of the lesion is formed by a major cavity, which is difficult to bridge by a cellular implant only. In this case, implanting a construct (hydrogel+MSCs) can bring benefit in 2 ways: the stem cells provide neurotrophic support for the prevention of secondary tissue damage and the promotion of tissue regeneration, while the hydrogel serves as a scaffold and as a bridge. Seeding MSCs on a hydrogel could thus create a “smart bioimplant.”
Even though myelinated axons infiltrated the hydrogel scaffold independently of the presence of MSCs, only the animals treated with both hydrogel and MSCs showed significant functional improvement. This functional improvement correlated with reduced tissue atrophy. We conclude that a hydrogel seeded with MSCs implanted into a chronic spinal cord lesion provides a scaffold for tissue ingrowth. Further, trophic support leads to the prevention of secondary tissue loss, the most probable mechanism leading to functional improvement in chronic SCI.
Footnotes
Acknowledgments
We thank Hana Hronová, Lenka Kohoutová, Alena Veselá, and Pavlína Macková for excellent technical assistance. We thank James Dutt for critical reading of the manuscript. We acknowledge the support provided by the grants AV0Z50390703, 1M0538, LC554, IAA500390902, GACR 309/08/H079, IGA MZ 1A8697–5, and the EC FP6 project RESCUE (LSHB-CT-2005–518233).
Author Disclosure Statement
No competing financial interests exist.