
Abstract
The origin (recipient/donor) of the myofibroblasts mediating fibrosis in sclerodermatous chronic graft-versus-host disease (cGvHD) was investigated. Sclerodermatous specimens obtained from a patient with extensive cGvHD after an HLA-identical sibling bone marrow transplantation were cultured in order to derive tissue myofibroblasts. All proliferating a-SMA+ fibroblastoid cells revealed recipient origin as examined by variable number tandem repeat (VNTR)-PCR. This case report shows that fibrosis in sclerodermatous lesions results from the activation and proliferation of locally-derived recipient fibroblasts rather than from donor-derived fibroblasts or circulating fibrocytes.
C
In December 1998, a 9-year-old boy underwent HLA-matched sibling allo-BMT using busulfan/cytoxan for acute lymphoblastic leukemia (ALL) in second complete remission. After 7 months, he experienced extensive cGVHD with skin, liver, and oral mucosa involvement. He was treated with steroids and azathioprine achieving complete cGVHD remission. After discontinuation of immunosuppressive therapy in November 1999, he gradually developed sclerodermatous lesions that partially resolved after extracorporeal photochemotherapy. In August 2001, he presented with ALL-relapse, received chemotherapy and then conditioning with hyperfractionated total body irradiation (2 Cy × 2 per day for 3 days) and etoposide 40 mg/kg to receive a second transplant from the same donor in November 2001. Sclerodermatous cGVHD was reactivated 3 months post-transplant and despite intensive immunosuppressive therapy from March 2002 to August 2005 it remained refractory. Unfortunately, our patient relapsed in November 2005 and died 2 months later.
Sclerodermatous tissues obtained by biopsy were divided into pieces and subjected to primary culturing of fibroblasts. Tissue pieces were placed on fibronectin-coated plastic plates and cultured in Dulbecco's modified Eagle's medium (Invitrogen, Carlsbad, CA), with 10% heat-inactivated fetal bovine serum (Sigma-Aldrich, St. Louis, MO), 5 ng/mL bTGF (R&D systems, Minneapolis, MN), 50 U/mL penicillin, and 50 μg/mL streptomycin. Proliferating adherent cells were expanded in a humidified incubator containing 5% CO2 at 37°C; cultured cells from various passages were trypsinized and then used for immunophenotyping and genotyping studies. All cells disclosed fibroblastoid morphology (elongated spindle-shaped cells) and stained with α-SMA and vimentin by immunohistochemistry, consistent with the myofibroblast phenotype (Fig. 1A and 1B). However, the expression of a-SMA in all cultured cells could be TGF-β-inducible and does not necessarily correspond to the in vivo findings. None of the cells were positive for CD45, cytokeratin, or factor VIII, indicating no contamination by cells of hematopoietic, endothelial, or epithelial origin. The origin (donor or recipient) of the myofibroblasts grown in culture was identified by polymerase chain reaction (PCR) using the polymorphic variable number tandem repeat (VNTR) marker D1S80, which was previously selected as informative (mismatched) in distinguishing donor cells from those of recipient [8]. The sensitivity of the VNTR-PCR assay is below 1% in the detection of the minor cell population. At the time of the biopsy, chimerism status was studied in peripheral blood. While peripheral blood mononuclear cells displayed only the donor pattern, the cultured myofibroblasts were all of recipient origin independently of culture period and order of passage (Fig. 1C and 1D).
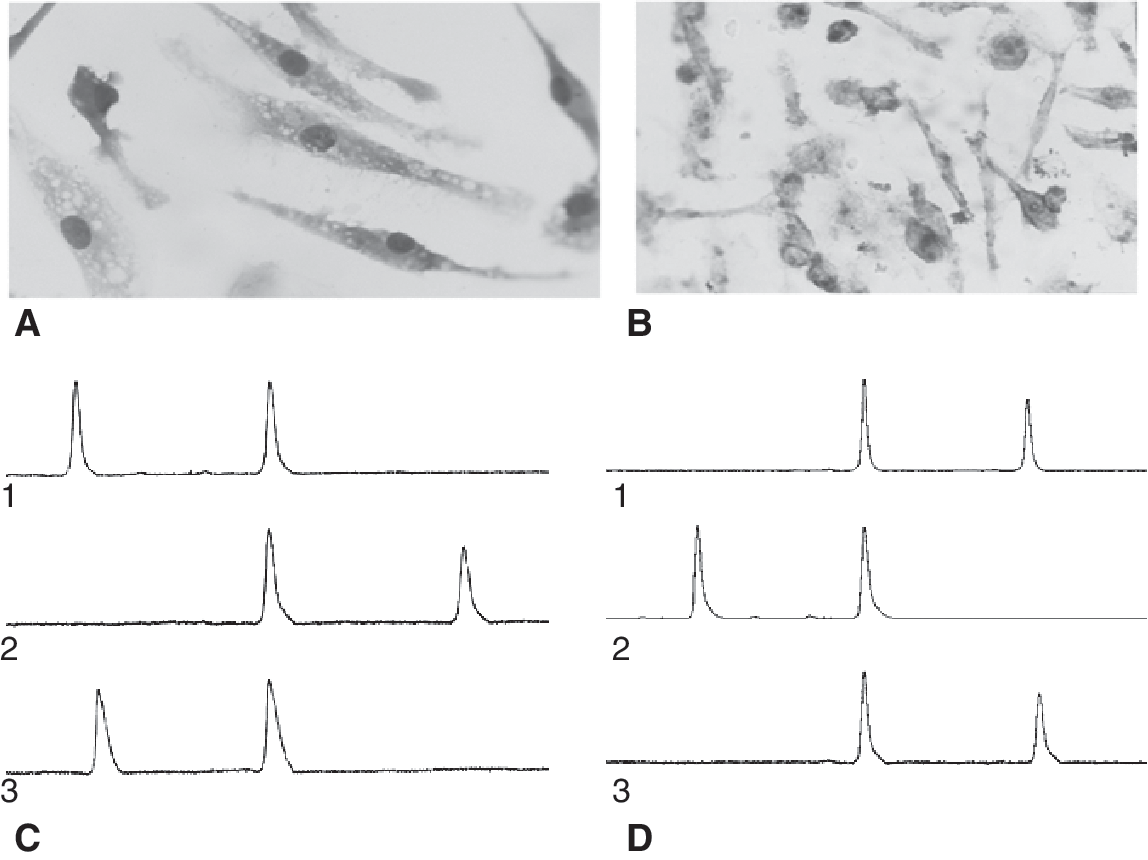
Morphology and analysis of chimeric status of cultured fibroblasts. (
According to a recent study, lacrimal gland specimens obtained from patients with dry eye due to cGVHD revealed 13.4% to 26.7% donor-derived CD34+ fibroblasts; however, in primary fibroblast cultures generated from the same specimens, the frequency of donor-derived fibroblasts ranged between 2% and 4% [9]. In an additional study, myofibroblasts of donor origin (6%) were also found in the conjunctivae of patients, who have undergone allo-SCT, including both patients with and without cGVHD [10]. Both studies suggest the presence of a small number of cells derived from donor hematopoietic cells expressing the phenotype of circulating fibrocytes (CD45+/α-SMA+). However, the findings were not convincing that donor fibrocytes participate in the excessive fibrosis observed in patients with ocular cGVHD, since there was no apparent relationship between the presence of donor-derived fibroblasts and cGVHD. Our findings suggest that fibrosis in sclerodermatous lesions results from the activation, recruitment, and proliferation of locally derived, connective tissue fibroblasts and not from donor-derived fibroblasts or circulating fibrocytes. Although the possibility of donor-derived cells' involvement at early time points of the fibrotic process cannot be excluded, according to our findings recipient-derived local myofibroblasts are involved in fibrosis at least at the late phase of a long progressive disease. Furthermore, the absence of bone marrow-derived fibrocytes from fibrotic lesions does not exclude the possibility of their contribution in the process of fibrosis through a paracrine mechanism. It has been shown recently that in burn patients fibrocytes contribute to fibrosis by secretion of cytokines that induce resident fibroblasts to differentiate into myofibroblasts [11]. Circulating donor fibrocytes may have an effect on fibrosis in sclerodermatous GVHD by a similar mechanism. It would be interesting to evaluate further both the chimeric status of myofibroblasts derived from sclerotic lesions and the relationship between circulating fibrocytes and the clinical course of cGVHD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.