
Abstract
The purpose of this study was to compare anterior cruciate ligament (ACL) regeneration between animal groups subjected to intra-articular injection of fresh whole bone marrow cells (BMCs), cultured mesenchymal stem cells (MSCs), or saline. Partially transected ACLs in Fischer 344/Nslc rats were prepared, followed by injection of BMCs, MSCs, or saline into the articular cavity at 1 week after transection. Donor cells expressing green fluorescent protein were detected in the recipient's transected ACLs at 4 weeks in the BMC and MSC groups, and their ACLs appeared almost normal histologically. Further, there were significantly more mature spindle cells in the BMC group than in the saline group at 4 weeks. Biomechanically, the tensile strength in the BMC group reached near normal levels at 4 weeks after injection. The levels of transforming growth factor-β1 in the ACL tissue and knee joint fluid in the BMC group were increased significantly compared with that of the saline group at 4 weeks as detected by immunohistochemical analysis. In conclusion, intra-articular bone marrow transplantation using fresh whole BMCs is an effective treatment for ACL partial rupture. This therapy is easy to apply in a clinical setting because no culture system is required for collecting MSCs.
Introduction
A
Since the 1980s, intrinsic healing of the tendon has been a focus of research [7]. Synovial cells in the joint may play an important role in ligament healing [8,9]. Further, platelets or several growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-β1 (TGF-β1), and basic fibroblast growth factor stimulate the healing of ligaments in animal models [10 –12]. The administration of extrinsic factors into the joint may enhance the intrinsic healing of the ACL. Mesenchymal stem cells (MSCs) from bone marrow have the capacity to differentiate into various cell types such as tendon, cartilage, bone, and adipose tissue [13]. In addition, MSCs have been reported to accelerate the healing of partially torn ACLs in a rat model [14].
In general, bone marrow transplantation (BMT) is a powerful strategy for the treatment of leukemia, aplastic anemia, and autoimmune disease in humans [15,16]. Further, we have recently shown that whole bone marrow cells (BMCs) are effective in regeneration after osteonecrosis, prevention of systemic osteoporosis, and activation of nucleus pulposus cells in animal models [17 –22]. BMCs consist of MSCs and hematopoietic stem cells (HSCs), and important growth factors are secreted by the several cell types that differentiate from MSCs or HSCs [23,24]. Therefore, both MSCs and HSCs may accelerate the healing of a torn ACL. We hypothesized that healing of the ACL can be enhanced by injection of fresh whole BMCs into the articular cavity of rats with freshly transected ACLs (intra-articular BMT [IA-BMT]). The purpose of the present study was to compare ligamentous healing using IA-BMT between animal groups administered BMCs, MSCs, or saline.
Materials and Methods
Animals
Thirteen-week-old male Fischer 344/Nslc rats weighing 420–530 g were purchased from Shimizu Laboratory Supplies. Fourteen-week-old green fluorescent protein (GFP) transgenic male rats were purchased from Japan SLC. The rats were maintained in our animal facility under specific pathogen-free conditions.
All surgical procedures and the postoperative care of animals were carried out in accordance with the guidelines of the National Institutes of Health for the care and use of primates. The study protocol was reviewed and approved by the Animal Experimentation Committee in our institution.
Preparation of BMCs and MSCs
To collect fresh whole BMCs, bone marrow was aspirated from the femur of the Fischer or GFP rats using an 18-gauge needle connected to a 10-mL syringe (Nipro Co.) containing 0.1 mL of heparin (1,000 U/mL). To remove adherent cells, the fresh whole BMCs were passed through a Cell Strainer (BD Falcon™). MSCs were obtained from bone marrow according to the modified procedure described previously [25,26]. Cells isolated with the use of this technique have a fibroblast-like appearance and are capable of multipotent differentiation [26]. In brief, after anesthesia, bone marrow was aspirated from the femur. The bone marrow was washed once with Dulbecco's modified Eagle's medium (Invitrogen Japan K.K.) and centrifuged at 2,000 rpm for 5 min. The cells were cultured in a flask containing Dulbecco's modified Eagle's medium and 10% fetal bovine serum (Invitrogen Japan K.K.), supplemented with antibiotics, under a humidified atmosphere of 5% carbon dioxide at 37°C for 1 week. The medium in the flask was replaced with the same volume of fresh medium at 3-day intervals. One week later, nonadherent cells were removed extensively, and the adherent cells were then collected from the surface of the flasks using 0.05% trypsin (Invitrogen Japan K.K.).
Murphy et al. reported that the transplantation of 1 × 107 MSCs into the articular cavity induced osteoarthritis or free bodies of scar tissue in a caprine model [25]. Agung et al. and Kanaya et al. reported that the transplantation of 1 × 106 MSCs into the articular cavity in a rat model showed no complications [14,27]. Therefore, in this study, we injected 1 × 106 BMCs or MSCs into the articular cavity.
Experimental protocol
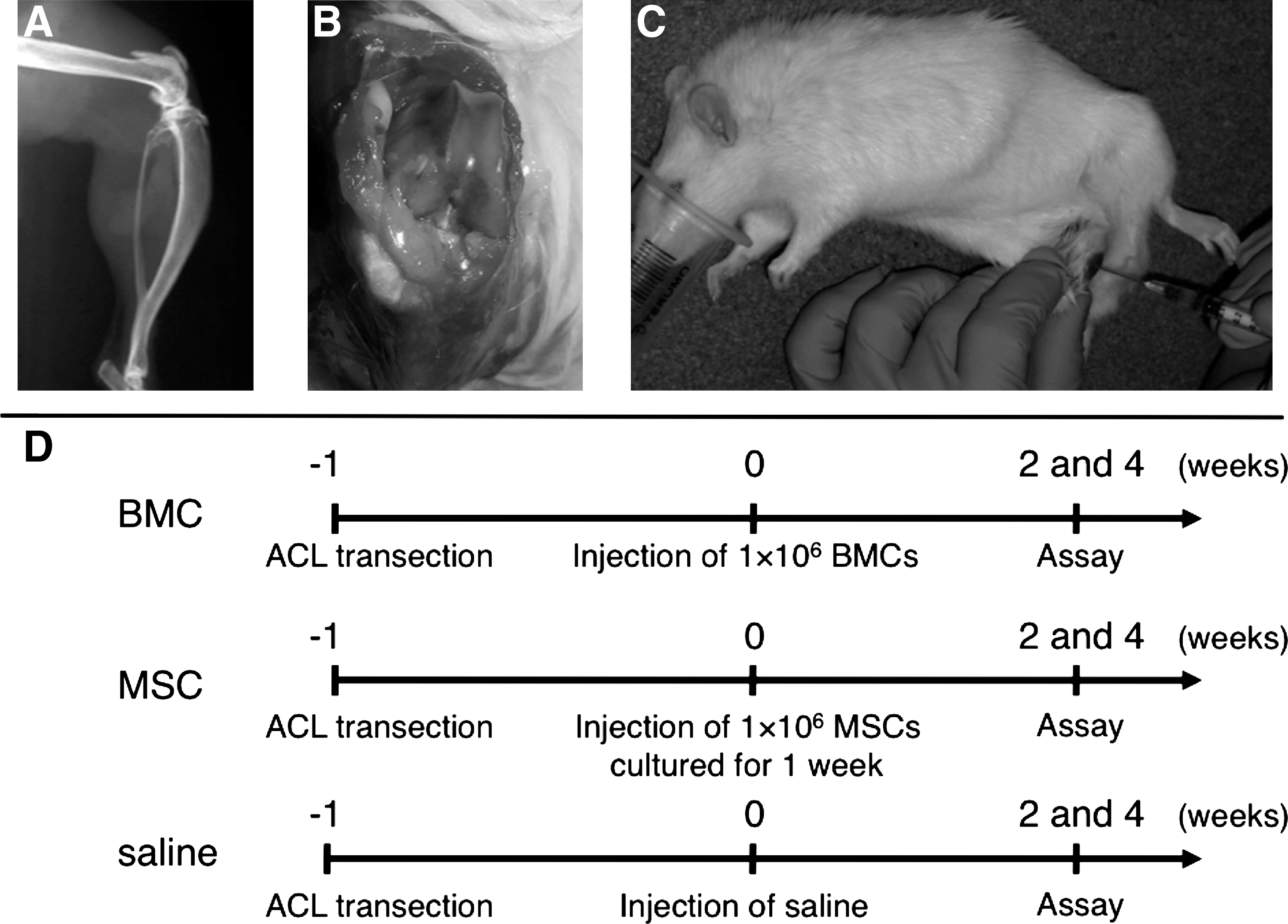
Prior to the start of this study, we evaluated the volume of the rat knee joint space. Soft X-ray photographs of an exact lateral view of the knee after an articular injection of Urografin60 (Bayer Schering Pharma AG) were taken under the following conditions: focus-film distance 40 cm, 2 mA, 40 Vp, and 60 s of exposure. Using these data, we estimated the volume of the rat knee joint space and determined the optimal volume of injection to be 0.05 mL (Fig. 1A).
Experimental protocol.
The rats were anesthetized with 5% fluothane (Halothane; Takeda Pharmaceutical Co., Ltd.) in an anesthetic chamber and then 3% fluothane using a mask. After both knee joints were exposed, the medial halves of their ACLs were transected under a microscope (Fig. 1B). The wounds were then closed in layers with 4-0 nylon sutures and the knee joints were not fixed. One week after transection of the ACLs, the animals were divided into 3 groups as follows (Fig. 1C, D): (1) BMC group, in which fresh whole BMCs (1 × 106 cells/0.05 mL) obtained from 14-week-old Fischer rats or 14-week-old GFP rats were injected into the articular cavity (IA-BMT) at 1 week after transection of the ACL; (2) MSC group, in which MSCs (1 × 106 cells/0.05 mL) obtained from 14-week-old Fischer rats or 14-week-old GFP rats and cultured for 1 week were injected into the articular cavity (IA-BMT) at 1 week after transection of the ACL; and (3) saline group, in which saline (0.05 mL) was injected into the articular cavity at 1 week after transection of the ACL.
Biomechanical tensile strength test
The ACLs of each group and the nontransected ACLs were evaluated biomechanically, and the ultimate failure load was measured at 0, 2, and 4 weeks after injection. Each femur–ACL–tibia complex was prepared after the removal of all other tissues. Both the femur and the tibia were fixated transversely using a C-wire (Zimmer K.K.) of 1.1 mm diameter at 10 mm from the joint line fixed by polymethylmethacrylate resin (Mizuho Co.). The tensile strength of the femur–ACL–tibia complex was tested using an autograph (AG-X; Shimadzu) in an extended knee position (Fig. 2A). Each femur–ACL–tibia complex was tested at a cross-head speed of 10 mm/min. The data were analyzed by TRAPEZIUM 2 software (Shimadzu) (Fig. 2B).

Biomechanical tensile strength test.
In addition, to evaluate the effect of TGF-β1 in healing of the torn ACL, we injected anti-TGF-β1 monoclonal antibody (R&D Systems) into the 3 groups in IA-BMT. Further, as a control, control mouse immunoglobulin G (IgG; R&D Systems) was injected into the 3 groups in IA-BMT. Antibody concentration was determined to be 10 μg/mL, because approximately 10 μg/mL of antibody neutralized 100% of bioactivity according to the manufacturer's protocol. The ACLs of each group were evaluated at 0, 2, and 4 weeks.
Histological evaluation
The ACLs of each group were evaluated histologically at 2 and 4 weeks after injection. The rats were sacrificed, and each femur–ACL–tibia complex was fixed for 1 week in 10% formalin. Bone samples were decalcified using EDTA (Wako Pure Chemical Industries Ltd.) for 2 weeks. The specimens were embedded in paraffin and cut into 4-μm sections in a coronal plane of the long axis of the ACLs. The sections were stained with hematoxylin and eosin or were immunostained for collagen type I. In brief, sections were stained for collagen type I using goat anti-human collagen type I polyclonal antibodies (Southern Biotechnology) at a dilution of 1:400, followed by incubation with biotinylated rabbit polyclonal anti-goat Igs (Dako Co.). The sections were washed in 0.05 M phosphate buffer (pH 7.6) and incubated in horseradish peroxidase–conjugated streptavidin for 10 min at room temperature. The sections were washed again, and a colored reaction product was developed using 3-3′-diaminobenzidine. Sections were then counterstained with Mayer's hematoxylin to demonstrate nuclei. Histological sections were analyzed in a blinded manner by 3 investigators (N.O., M.U., and T.N.), who were not informed of the groups assignment, and were evaluated using the semiquantitative tendon scoring system (modified Bonar scale) [28]. We evaluated (1) tenocyte (spindle cell) morphology and proliferation (grade 0–3) and (2) collagen bundle characteristics (grade 0–3) using the Bonar scale. Moreover, the number of nuclei immunostained for collagen type I was counted manually at 4 weeks after injection. The field was selected in the transected area, and the area of each captured field was always 1 mm2.
In addition, specimens from the BMC and MSC groups were sectioned using a Cryostat CM3050S (Leica Microsystems) and a Cryo Film Transfer kit (Finetec Co.) after freezing with hexane (Wako Pure Chemical Industries Ltd.). GFP luminescence in these sections was observed using a fluorescence microscope. The number of GFP-positive cells were counted manually at 4 weeks after injection. The field was selected in the transected area, and the area of each captured field was always 1 mm2.
Immunological measurement of cytokines in knee joint fluid
The ACLs of each group were evaluated immunologically at 2 and 4 weeks after injection. The rats were anesthetized using fluothane, and the knee joint fluid was collected by inflating and deflating using a 26-gauge needle connected to a 1-mL syringe containing 0.05 mL of saline. TGF-β1 in the knee joint fluid was quantified using an enzyme-linked immunosorbent assay (ELISA) kit (BioSource International, Inc.) according to the manufacturer's protocol.
Reverse transcription–polymerase chain reaction
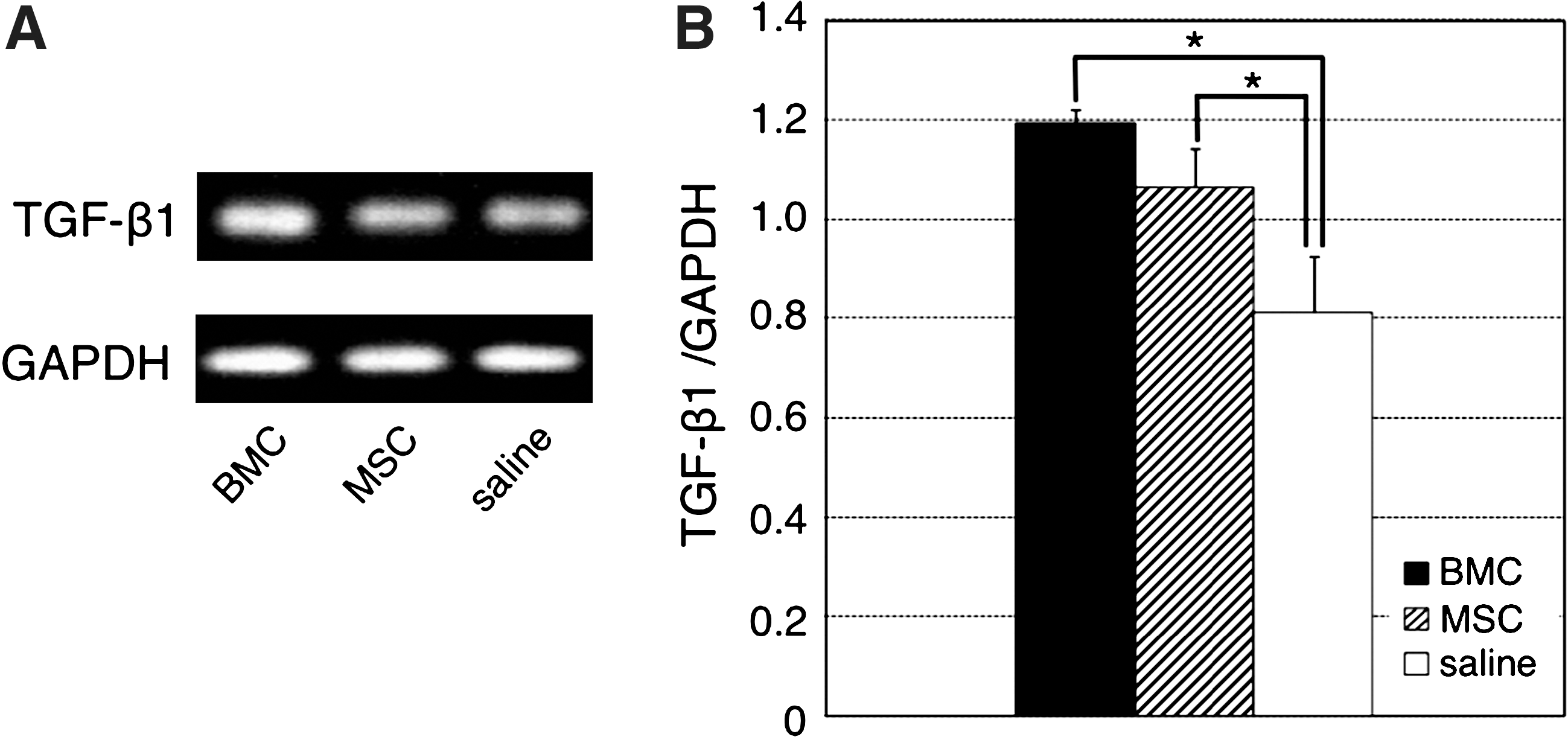
We examined the expression of glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and TGF-β1 mRNA in the ACLs at 2 weeks after injection. Levels of mRNA for ACL phenotypic markers were determined using the sequences of primers for GAPDH and TGF-β1 (Invitrogen Japan K.K.). The primer sequences were as follows: GAPDH, 5′-GGGTGGTGCCAAAAGGGT-3′ and 5′-GGAGTTGCTGTTGAAGTCACA-3′; TGF-β, 5′-TGTACGGCAGTGGCTGAAC-3′ and 5′-ATTCATGTTGGACAACTGCTC-3′. GAPDH and TGF-β1 mRNA was amplified using a pair of primers at 94°C for 1 min, 57°C for 1 min, 72°C for 1 min for 40 cycles, and a final extension at 72°C for 10 min. Polymerase chain reaction products were electrophoresed on a 1% agarose gel (Invitrogen Japan K.K.), stained with ethidium bromide (0.5 μg/mL), and visualized on a UV transilluminator (ATTO).
Statistical analyses
Statistical analyses were performed in the 3 groups using one-way analysis of variance to determine differences in each parameter. Post hoc comparisons were performed by Student's t-test to evaluate the difference between the 2 groups. Differences were considered statistically significant when the P value was <0.05.
Results
Tensile strength test
As shown in Fig. 3, the tensile strength of the femur–ACL–tibia complexes from the BMC, MSC, and saline groups were 26.6 ± 1.6, 24.2 ± 3.5, and 14.9 ± 2.2 N, respectively, at 2 weeks after injection without anti-TGF-β1 monoclonal antibody. At 4 weeks after injection, the tensile strength of the femur–ACL–tibia complexes from the BMC, MSC, and saline groups were 29.2 ± 1.1, 26.8 ± 2.9, and 13.4 ± 2.3 N, respectively. The tensile strength of the BMC group at 2 and 4 weeks was increased significantly compared with that of the saline group. Further, at 4 weeks, the tensile strength of the BMC group was similar to the nontransected femur–ACL–tibia complex. No significant differences were observed between the BMC and MSC groups at 2 and 4 weeks.

Tensile strength of the femur-ACL-tibia complex. The ultimate failure load in the BMC, MSC, saline and nontransected groups, respectively. The results are expressed as the mean ±standard deviation of 6 ACLs. Statistical analyses were performed by Student's t-test: *P < 0.05, saline versus BMC or MSC group. Statistical analyses were performed by Student's t-test: † P < 0.05, with anti-TGF-β1 versus without anti-TGF-β1 in each group. Statistical analyses were performed by Student's t-test: # P < 0.05, nontransected versus BMC, MSC, or saline group. TGF-β1, transforming growth factor-β1.
At 2 weeks after injection and with anti-TGF-β1 monoclonal antibody, the tensile strength of the femur–ACL–tibia complexes from the BMC, MSC, and saline groups were 20.3 ± 1.3, 19.1 ± 1.4, and 14.1 ± 1.3 N, respectively. At 4 weeks after injection, the tensile strength of the femur–ACL–tibia complexes from the BMC, MSC, and saline groups were 21.5 ± 0.7, 20.2 ± 2.4, and 12.8 ± 1.9 N, respectively. At 2 and 4 weeks after injection, the tensile strength of the BMC group was increased significantly compared with that of the saline group. In comparison of with and without anti-TGF-β1 monoclonal antibody, there were significant differences at 2 and 4 weeks after injection in the BMC and MSC groups.
The tensile strength of the femur–ACL–tibia complexes with control IgG at 0, 2, and 4 weeks were 14.6 ± 1.2, 15.5 ± 1.8, and 13.9 ± 2.5 N, respectively. No significant differences were observed between the control IgG and saline groups at 0, 2, and 4 weeks.
Histological findings
The transected area in the BMC group at 2 weeks after injection was sharp and not retracted (Fig. 4A), whereas the transected areas in the MSC or saline groups were severely retracted (Fig. 4B, C). At 4 weeks after injection, the transected areas in the BMC and MSC groups were not retracted (Fig. 4D, E); however, the transected area in the saline group was retracted (Fig. 4F).
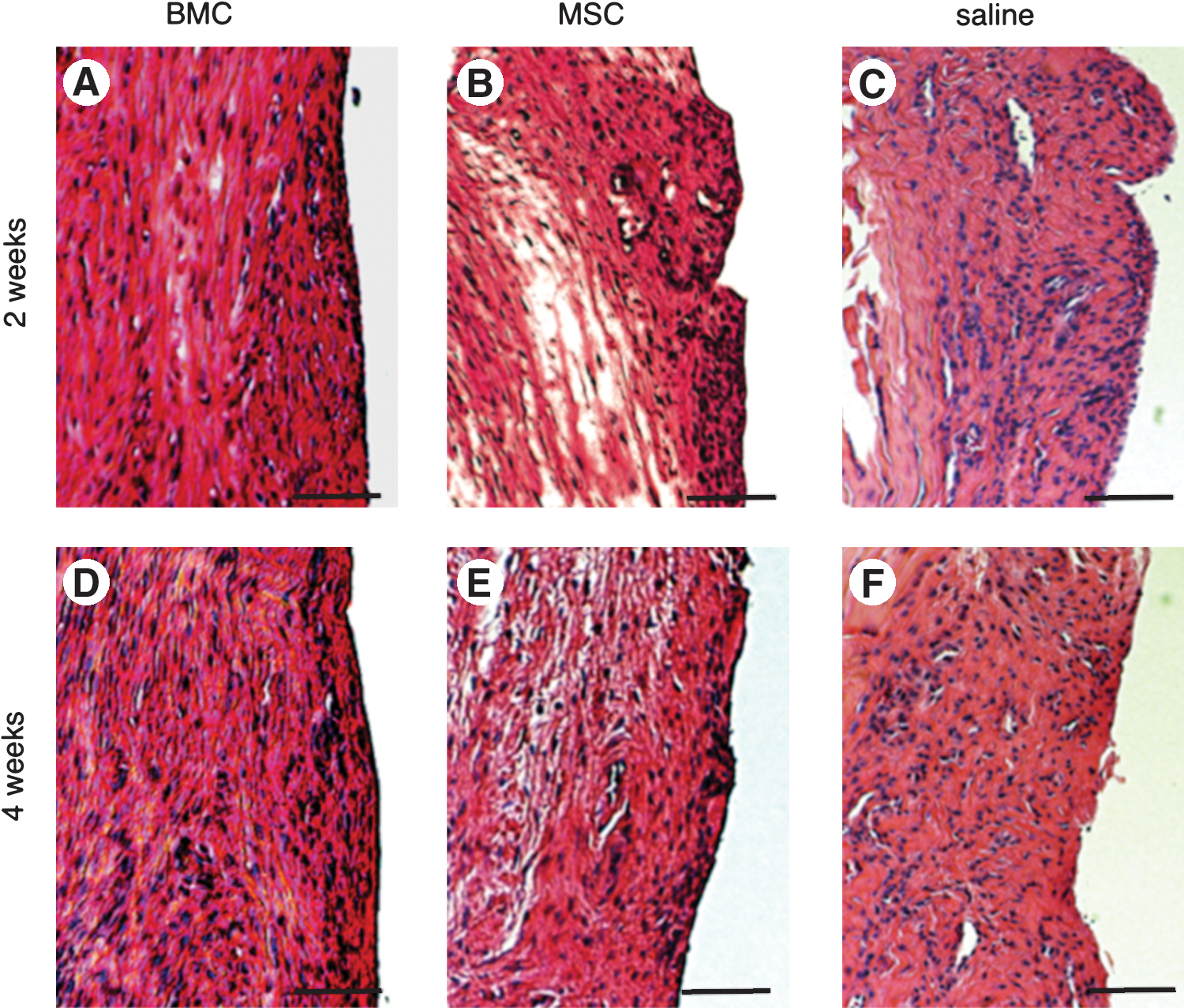
Histological findings (hematoxylin and eosin). Specimen of the transected ACLs from:
The tenocyte scores in the BMC, MSC, and saline groups at 2 weeks after injection were 2.0 ± 0.4, 2.2 ± 0.5, and 2.7 ± 0.6, respectively. Macroscopic examination showed more spindle cells in both the BMC and MSC groups than in the saline group; however, there was no significant difference between the groups in the tenocyte scores (Fig. 4A–C). At 4 weeks after injection, the tenocyte scores in the BMC, MSC, and saline groups were 0.6 ± 0.3, 1.0 ± 0.6, and 2.1 ± 0.5, respectively. There were significantly more mature spindle cells in both the BMC and MSC groups than in the saline group (Fig. 4D–F).
The collagen scores in the BMC, MSC, and saline groups at 2 weeks after injection were 2.2 ± 0.3, 2.3 ± 0.5, and 2.8 ± 0.5, respectively. There was no significant difference between the groups in the collagen scores (Fig. 4A–C). At 4 weeks after injection, the collagen scores in the BMC, MSC, and saline groups were 0.8 ± 0.5, 1.0 ± 0.4, and 2.2 ± 0.5, respectively. There was significantly more collagen arranged in tightly cohesive well-demarcated bundles in both the BMC and MSC groups than in the saline group (Fig. 4D–F).
Immunohistochemical findings
Collagen fibers are considered to be very important elements in ligament healing. Collagen type I is responsible for mechanical strength of the ligament [29]. To quantify the degree of cell proliferation, cells were counted in the transected area at 4 weeks after injection. The number of nuclei immunostained for collagen type I in the BMC, MSC, and saline groups were 38.5 ± 4.3, 32.8 ± 2.3, and 22.3 ± 1.6 cells/mm2, respectively. The number of nuclei in the BMC group was increased significantly compared with that in the MSC or saline group (Fig. 5A–C).

Immunohistochemical staining of collagen type I. Specimen of the transected ACLs from:
Fluorescence photomicrograph
Fluorescence photomicrographs in the BMC and MSC groups at 4 weeks after injection showed GFP-positive cells in the transected ACLs (Fig. 6A, B). These findings indicate that the donor-derived cells migrated into the recipient transected ACLs and differentiated. There were donor-derived GFP cells and host cells in the transected ACLs, and the number of GFP-positive cells in the BMC and MSC groups was 27.1 ± 3.6 and 15.8 ± 2.5 cells/mm2, respectively. The number of GFP-positive cells in the BMC group was increased significantly compared with that in the MSC group.
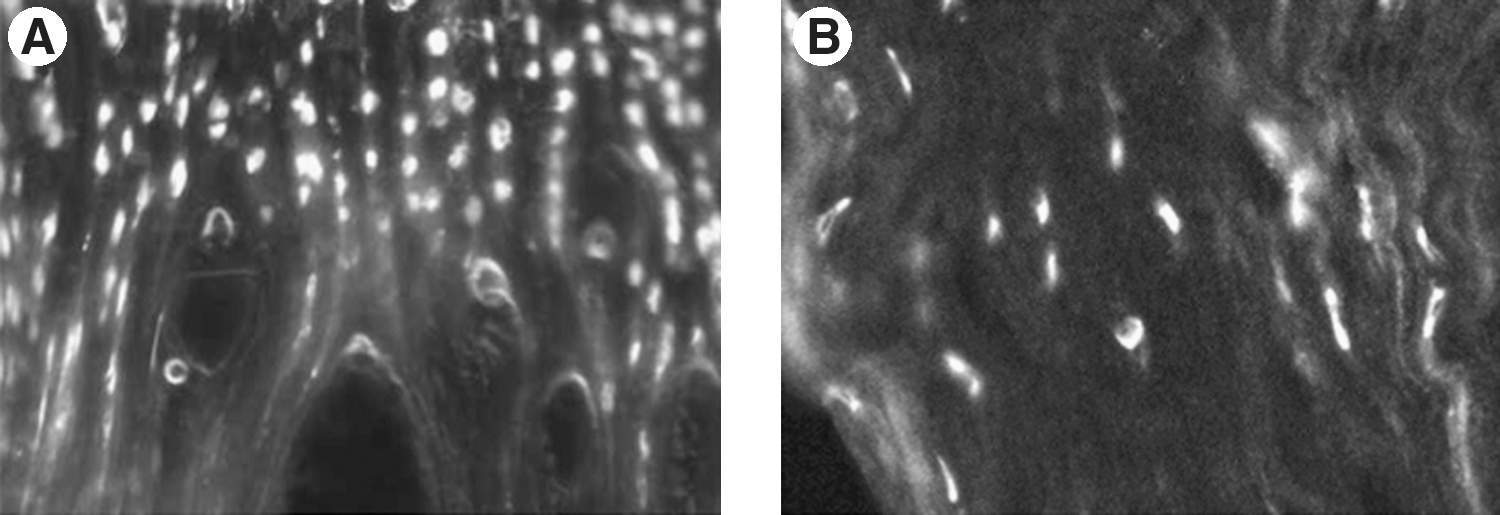
Fluorescence photomicrograph showing green fluorescent protein–positive cells.
Analyses of cytokines in knee joint fluid
As shown in Fig. 7, the values of TGF-β1 levels in the BMC, MSC, and saline groups were 40.8 ± 5.9, 34.1 ± 2.5, and 24.5 ± 2.2 pg/mL, respectively, at 2 weeks after injection. The values of TGF-β1 levels in the BMC group were increased significantly compared with that in the MSC or saline group. At 4 weeks after injection, the values of TGF-β1 levels in the BMC, MSC, and saline groups were 88.1 ± 8.3, 83.4 ± 6.0, and 78.9 ± 4.4 pg/mL, respectively. The values of TGF-β1 levels in the BMC group were increased significantly compared with that in the saline group. However, no significant differences were observed between the BMC and MSC groups.
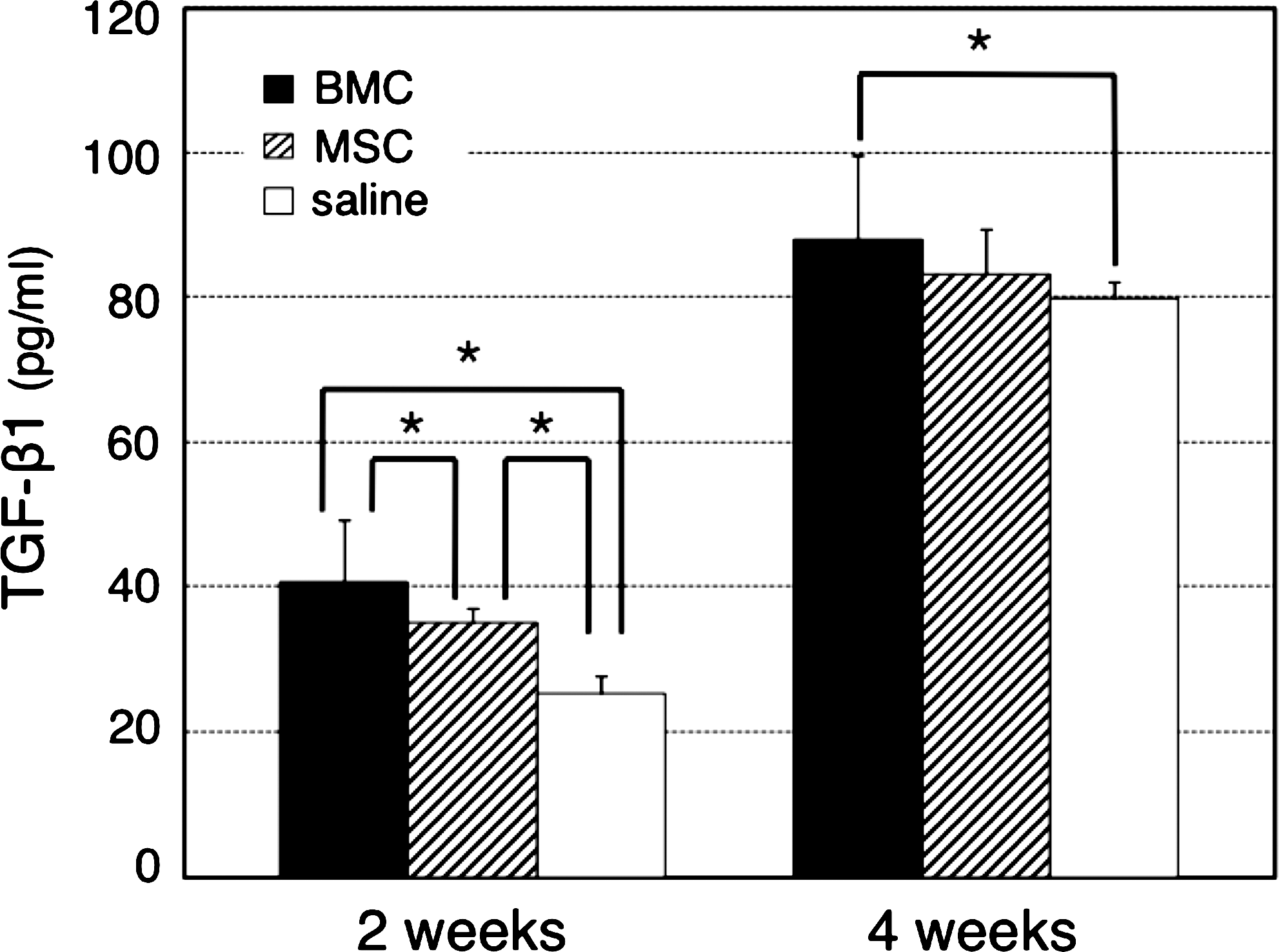
Measurement of TGF-β1 in knee joint fluid. The values of TGF-β1 levels in the BMC, MSC, and saline groups. The results are expressed as the mean ± standard deviation of 6 ACLs. Statistical analyses were performed by Student's t-test: *P < 0.05.
Electrophoretic analyses of reverse transcription–polymerase chain reaction products
At 2 weeks after injection, TGF-β1/GAPDH in the BMC, MSC, and saline groups were 1.19 ± 0.03, 1.06 ± 0.08, and 0.81 ± 0.11, respectively. The expression of TGF-β1 mRNA in the BMC and MSC groups was increased significantly compared with that of the saline group (Fig. 8A, B).
Discussion
ACL ruptures are one of the most frequent ligament injuries. However, it is difficult for a torn ACL to regenerate naturally because the injury may disrupt the blood supply and the IA location of the ACL may compromise the organization of the blood clot necessary for healing [4]. Therefore, surgical treatment has become the first choice for treatment for a torn ACL. Nevertheless, surgical reconstruction may show postoperative complications and a failed ACL reconstruction [6], and new methods are necessary for the treatment of a torn ACL. The healing process in the torn ACL consists of intrinsic healing and extrinsic healing. Intrinsic healing occurs within the tendon itself, as a result of the activity of intrinsic fibroblasts and the increase in the intratendinous blood supply from the synovium [7 –9]. Extrinsic healing is due to several factors from the ligaments, such as the extrinsic peripheral fibroblasts, plasma, inflammatory cells, and extratendinous vascular invasion [11,15,30,31]. However, the ACL does not have sufficient extrinsic healing effects, because it exists in the articular cavity. We hypothesized that to increase the healing ability of a torn ACL in the articular cavity, it was necessary to induce the extrinsic healing effects observed in extra-articular ligaments such as the collateral ligaments.
MSCs from bone marrow are well known to have a capacity to differentiate into various types of cells, such as osteoblasts, chondrocytes, adipocytes, stromal cells, and fibroblasts [13,32 –34]. Further, undifferentiated MSCs produce important growth factors and cytokines that promote the expansion and differentiation of HSCs and modify the response of inflammatory immune cells [35]. Recently, IA transplantation therapies using MSCs for a torn ACL have been reported [14,27]. IA transplantation therapies using MSCs showed excellent outcomes in the regeneration of a transected ACL. However, to obtain sufficient quantities of purified MSCs for successful transplantation, the cells require proliferation in culture for several days. Moreover, clinically, application of this therapy using MSCs on the torn ACL is difficult because of the risks of infection or contamination with bacteria. Therefore, when using MSCs, a safer and quicker culture system is necessary. Currently, whole BMCs, which consist of MSCs and HSCs, are available for systemic transplantation in treatments of malignant lymphoma, leukemia, and aplastic anemia [15,16]. Therefore, in this study, we applied fresh whole BMCs obtained from GFP transgenic animals to the regeneration of the ACLs. Consequently, the donor-derived GFP-expressing cells were detected in the recipient's transected ACLs at 4 weeks after injection in the BMC and MSC groups, although there were both donor-derived GFP cells and host cells in the transected ACLs (Fig. 6A, B). The number of GFP-positive cells in the BMC group was increased significantly compared with those in the MSC group. In the IA transplantation of GFP-positive MSCs, Kanaya et al. reported that the injected MSCs may produce growth factors such as PDGF, basic fibroblast growth factor, and TGF-β, which may represent activated native ACL cells. The native ACL cells may have proliferated and migrated into the injured area of the ACL [14]. Our results suggest that the injected BMCs may behave in the same manner. Further, the injected BMCs, which consist of MSCs and HSCs, may be more effective than the injected MSCs only for the incorporation into ACLs and differentiation. Histologically, at 4 weeks after injection, the BMC group showed more frequent mature spindle cells and tighter collagen bundles, compared with the MSC and saline groups (Fig. 4D–F).
In the process of ligament healing, the gap is filled initially by a blood clot, which is invaded immediately by proliferating fibroblasts from the surrounding connective tissue. Four days after the injury, new collagen fibrils form, and after 2 weeks, these fibrils bridge the gap. Finally, the ligament shows rows of fibroblasts within parallel bundles of extracellular matrix composed primarily of collagen type I fibers [29]. These collagen type I fibers are important elements for the mechanical strength of a ligament. In this study, at 4 weeks after injection, the number of nuclei in the BMC group was increased significantly compared with that in the MSC and saline groups (Fig. 5A–C). These findings suggest that IA-BMT with fresh whole BMCs results in the migration of donor-derived cells into the recipient's ACLs (Fig. 6A, B), which generates more mature fibroblasts and collagen fiber bundles. In particular, collagen type I fibers for mechanical strength of the ligament were generated more frequently. Consequently, the tensile strength of the femur–ACL–tibia complexes treated with the fresh whole BMCs increased immediately and reached similar levels to normal at 4 weeks after injection (Fig. 3).
The blood clots that form after tissue damage contain not only platelets, but also several other cell types, which release a variety of growth factors, including PDGF and TGF-β1 [36]. These growth factors have been reported to stimulate the healing of the ACL in vivo [10,11]. In particular, TGF-β1 accelerates the proliferation and matrix synthesis of ligament fibroblasts of the ACL in vitro [30,37 –39]. Further, TGF-β1 is secreted not only by fibroblasts, but also by several cell types that differentiate from HSCs [24]. In this study, we analyzed the values of TGF-β1 levels in the knee joint fluid at 2 and 4 weeks after injection. The TGF-β1 levels in the BMC group were increased significantly compared with that in the MSC and saline groups at 2 weeks after injection (Fig. 7). In addition, we analyzed the expression of TGF-β1 mRNA in the ACLs at 2 weeks after injection. The expression of TGF-β1 mRNA in the BMC group was increased more than that in the MSC group and significantly more than that in the saline group (Fig. 8). These findings suggest that IA-BMT with fresh whole BMCs enhances the expression of TGF-β1 in the ACLs and knee joint fluid in the articular cavity, resulting in the acceleration of both intrinsic healing in the ACLs and extrinsic healing from the articular cavity. Further, we inhibited TGF-β1 activity using an anti-TGF-β1 monoclonal antibody and examined the healing of the torn ACL (Fig. 3). In the BMC and MSC groups, the tensile strength with inhibition of TGF-β1 activity was decreased significantly over that without inhibiting TGF-β1 activity. These findings suggest that TGF-β1 plays important roles in the healing of a torn ACL. IA-BMT can encourage TGF-β1 to activate immediately, which suggests that IA-BMT has the crucial advantage for the treatment of a torn ACL.
We hypothesize that IA-BMT with fresh whole BMCs, which consists of MSCs and HSCs, may be effective in the acceleration of ACL healing (Fig. 9), because (1) fibroblasts that differentiate from MSCs secrete TGF-β1 and synthesize collagen type I, (2) hematolymphoid cells that differentiate from HSCs secrete important growth factors and cytokines for extrinsic healing, and (3) microenvironments in the articular cavity are changed from a poor environment to an adequate environment for healing. However, before we can apply IA-BMT to ACL ruptures in humans, a number of problems need to be addressed. First, the clinically damaged ACLs in traumatic injury are different from the experimental partial-transected ACLs examined in this study. We suggest that IA-BMT is available for partially torn ACLs or extended ACLs, and not for completely torn ACLs. If the damaged ACLs are a complete tear, they require conventional therapy including IA-BMT and surgical reconstruction. Second, we must determine the optimal density and volume of BMCs for IA-BMT in humans, because we performed IA-BMT in a rat model. Third, we did not evaluate other structures, such as cartilage and the meniscus, in the articular cavity. However, clinically, long-term outcomes of the microfracture techniques for traumatic chondral defects were reported by Steadman et al. Therefore, we suggest that major side effects may not occur using IA-BMT [40].
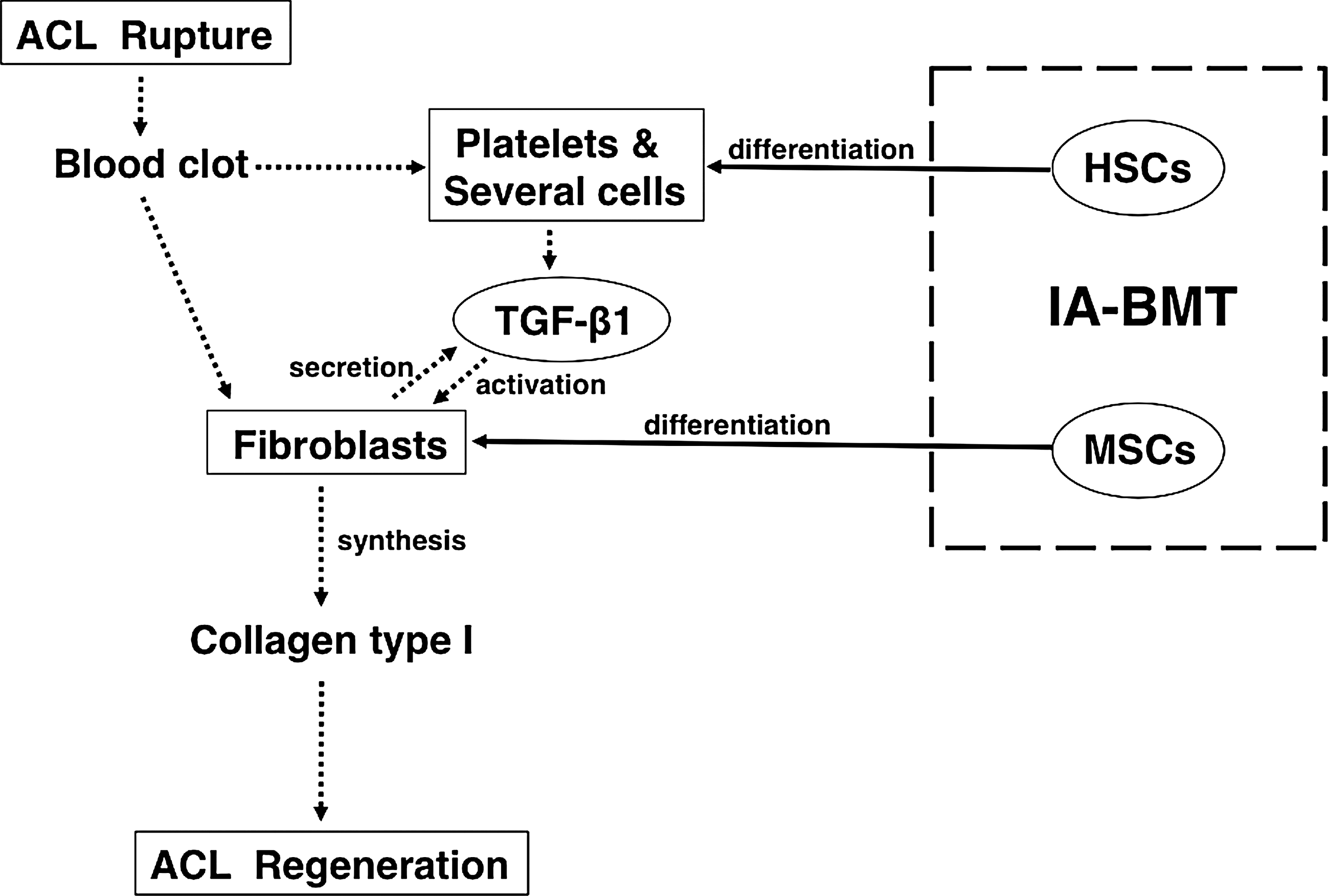
Mechanisms underlying the treatment of ACL healing by IA-BMT with fresh whole BMCs. For ACL healing, we consider that fresh whole BMCs, namely MSCs and HSCs, are used, because the combination has significant advantages over MSCs only. The dotted arrows show the cascade of events, leading to ACL healing in general. The solid arrows show the effects of IA-BMT with fresh whole BMCs. HSCs, hematopoietic stem cells.
In conclusion, IA-BMT with fresh whole BMCs is an effective treatment for ACL partial rupture in rats. Our results suggest that IA-BMT with fresh whole BMCs, consisting of MSCs and HSCs, may be clinically advantageous for a partially torn ACL in humans.
Footnotes
Acknowledgments
This study was supported by a grant from “Strategic Research Base Development Program for Private Universities”: matching fund subsidy from MEXT (Ministry of Education, Culture, Sports, Science, and Technology), and the Brain Medical Research Center Project of the Ministry of Education. The funds were used to pay for all aspects of study, including the animals, chemicals, and supplies.
Author Disclosure Statement
The authors have nothing to disclose.