
Abstract
Hyperkinetic pulmonary arterial hypertension (PAH) severely influences the success of operation for congenital heart disease and deteriorates the prognosis of disease. Adipose-derived stromal cell (ADSC) is a good alternative multipotent stem cell for regeneration medicine. PAH rat models were established by arteriovenous shunt and ADSCs were isolated, cultured, and labeled in vitro. Twelve weeks after shunt operation, rats received an injection of 5 × 107 ADSCs. Two weeks after transplantation, hemodynamic abnormality induced by the shunt flow and the hypertrophy of right ventricle were reversed, which was confirmed by invasive measurement and echocardiography examination. The PAH rats receiving cell transplantation demonstrated decreased remodeling of small arteries in the lung; immunohistochemistry analysis showed augmented expression of hepatocyte growth factor (HGF) and increased number of pulmonary small arteries. Western blot and real-time reverse transcriptase–polymerase chain reaction indicated that the protein and mRNA levels of HGF and endothelial nitric oxide synthase increased, respectively, in the lung after cell transplantation. Our results suggested that ADSC transplantation can ameliorate PAH induced by shunt flow by enhancing the expression of HGF and subsequently promoting angiogenesis in the injured lung tissue.
Introduction
P
Treatment of PAH has achieved great improvement over the past decades [2]. All the updated treatment strategies including inhalation of NO, application of nitrate drugs, prostacyclin, and other oral agents improve symptoms and the life quality of PAH patients but still have drawbacks and limitations [3,4]. When obstructive remodeling, namely the irrecoverable pathological destruction, occurred in pulmonary distal even proximal vessels, vasodilation treatment mentioned above seemed no longer efficient. This devastating disease ultimately deteriorated the gas exchange and pulmonary function. Eventually, heart and lung transplantation was the only treatment option for the patients with PAH [5]. Thus, the development of effective therapies for patients with PAH is critical.
Recently, therapeutic angiogenesis has emerged as one of the most promising therapies. Rapid revascularization for compensating the injured and occlusive vessels might benefit the restoration of pulmonary physiological function. Transplantation of bone marrow stromal cells (BMSCs), bone-marrow-derived mononuclear cells, and endothelial progenitor cells (EPCs) from peripheral blood (also from bone marrow or umbilical cord blood) have been efficient methods to attenuate lung injury in various animal models via cell-based therapeutic angiogenesis [6 –8]. However, BMSC transplantation requires a large amount of bone marrow under general anesthesia, which may impose a heavy load on patients with other disorders, whereas EPC expansion on a large scale not only needs a large volume of blood but also requires a complicated technology. These limit the practical application of BMSCs and EPCs.
Adipose-derived stromal cells (ADSCs), an alternative stem cell to BMSCs and EPCs, have attracted the interests of many researchers with its advantages such as minor invasion and easy culture [9 –11]. Implantation of ADSCs could induce angiogenesis in ischemic tissues by participating in the formation of vessels or via secretion of angiogenic growth factors such as hepatocyte growth factor (HGF) [12 –14]. Ono et al. indicated that the loss of endogenous HGF may be a feature of the pathogenesis of pulmonary hypertension and that HGF supplementation may minimize pathological lung conditions, even in advanced pulmonary hypertension [15]. Transplantation of ADSCs could ameliorate pulmonary emphysema through selectively enhancing expression of endogenous HGF in the injured lung tissues, which lead to alveolar and vascular regeneration [16]. Further, HGF stimulates the production of NO in vascular endothelial cells through endothelial nitric oxide synthase (eNOS) activation [17], and the reduced expression of eNOS in the lung is closely associated with PAH patients [18]. Therefore, ADSC transplantation might be a better choice for treatment of PAH than BMSCs or EPCs and it is possible to attenuate PAH with ADSC transplantation through secretion of HGF. As far as we know, it is the first time that ADSCs were introduced into the treatment for PAH.
In this study, a model of PAH induced by arteriovenous shunt was established in rats according to previous methods [19]. ADSCs were isolated and cultured in vitro and then transplanted into the model rats to test the hypothesis that ADSC autologous transplantation could attenuate pulmonary hypertension, reduce the remodeling of the small arteries, and reverse the hemodynamics abnormality induced by PAH. Further, the underlying mechanism was also investigated.
Materials and Methods
Animal model preparation
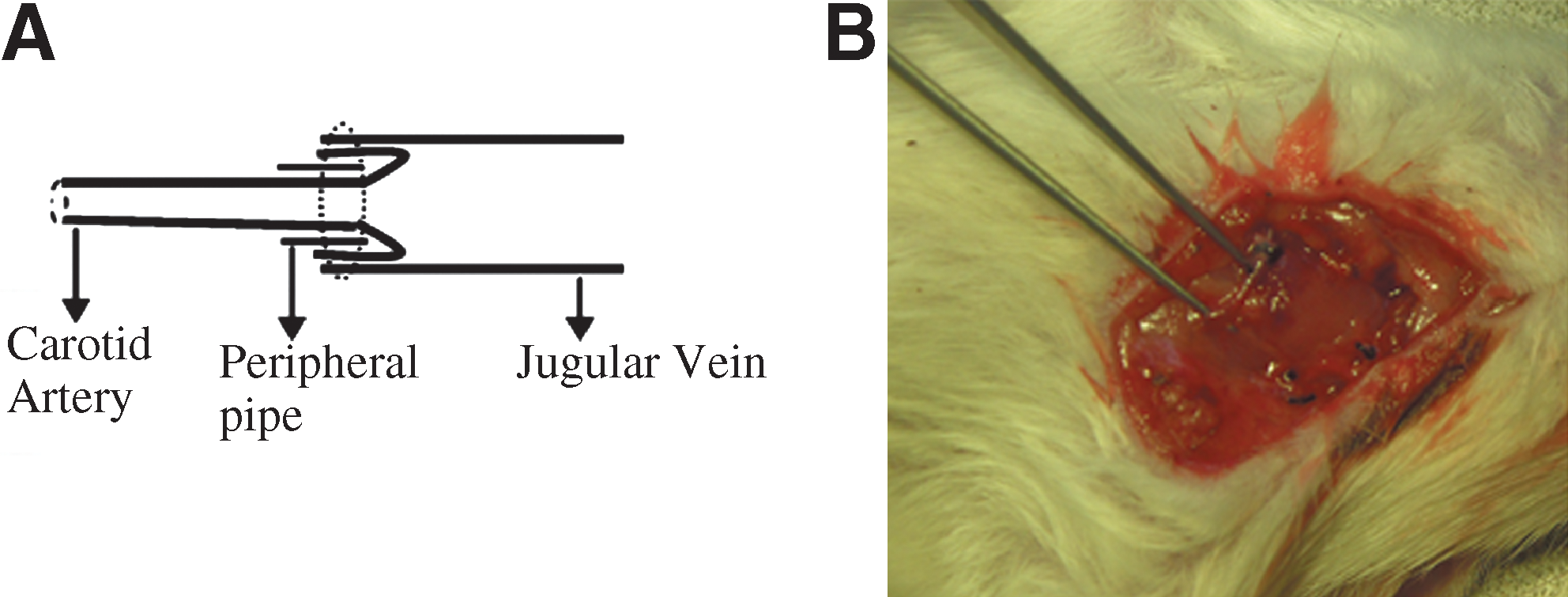
Male Wistar rats (n = 140, weighing 123 ± 11 g) were provided by the Laboratory Animal Center of Shandong University. Animals received humane care and the experiments were performed in accordance with the guidelines of Animal Care and Use Committee of Shandong University. The rats were anesthetized with 0.25% pentobarbital sodium (40 mg/kg, intraperitoneal injection). An incision of 2 cm was made in the left side of neck after a simple skin preparation. After left jugular vein and left common carotid artery were freed, heparin sodium (5 mg/kg) was injected intraperitoneally. The left jugular vein and common carotid artery were cut off and the distal ends of the vein and the artery were ligated. The proximal ends of the artery and vein were connected in a cuff style (Fig. 1A). Once the arteriovenous shunt was completed, pulsation and bulging of the proximal part of the jugular vein were observed (Fig. 1B). The incision was closed after being washed with gentamycin (4,000,000 U). Animals were fed in single cage for 3 days and administrated aspirin (10 mg/kg/day) for anticoagulation in the first 2 weeks after operation. Sham operation was performed by isolating the vessels only from rats.
Animals were separated into the sham group (sham operation group), blank group (without any treatment after shunt surgery), cell group [5 × 107 cells in 0.5 mL Dulbecco's modified Eagle's medium (DMEM) were injected per rat through right jugular vein on postoperative week 12], and DMEM group (injection of 0.5 mL DMEM). Five rats in each group were euthanized for the evaluation of PAH on the 4th, 8th, and 12th postoperative weeks. Data of the rats undergoing shunt operation on postoperative week 12 were regarded as the baseline level for cell treatment. The residual rats in each group were euthanized at 2 weeks after cell engraftment.
Isolation and characterization of ADSCs
Four weeks after surgery (body weight of rats at that time was 206 ± 13 g), ADSCs were isolated from the inguinal fat pad by enzyme digestion method and cultured according to previous reports with little modification [10]. Briefly, the adipose tissues were minced into small fragments and incubated with collagenase type I [Invitrogen; prepared in phosphate-buffered saline (PBS) containing 2% penicillin/streptomycin (Sigma) and 20% bovine serum albumin] in water bath (37°C, 90 min) with interval shaking (per 15 min) and pipetting (per 30 min) to digest the tissue. Then, the activity of collagenase was neutralized by adding equivalent DMEM (Gibeco) containing 10% preheated fetal bovine serum (FBS; Gibeco) to the tissue sample. After centrifugation (2,000 rpm for 5 min), the mature adipose cells on upper layer were removed and the pellet as the stromal vascular fraction was resuspended in the red blood cell (RBC) lysis buffer (10 min on ice) for lysing the RBCs. Cell suspension was centrifugated for another 5 min (1,500 rpm) to remove supernatant containing the cell debris, and the cell pellets were plated in DMEM containing 10% FBS and 1% penicillin/streptomycin after a series of filtration through different strainers (150, 100, and 75 μm). Cell cultures were maintained in a humidified tissue culture incubator (37°C, 5% CO2) and fed 3 times per week.
Once adherent cells were at >80% confluence after the initial plating (passage 0, P0), generally within 7–10 days, the cultures were passaged with 0.25% trypsin–0.01% EDTA (Gibco) at a plating density of about 2,000 cells/cm2 (P1). To test the multidirectional differentiation potency of the ADSCs, inductions of adipocyte, osteoblast, and endothelium cells were conducted by feeding the ADSCs with adipogenic differentiation medium (DMEM containing 10% FBS, 0.5 mM isobutylmethylxanthine, 200 μM indomethacin, 10 μM bovine insulin, and 1 μM dexamethasone), osteogenic medium [DMEM supplemented with 10% FBS, 10 mM b-glycerophosphate, 0.1 μM dexamethasone, and 50 μM ascorbic acid (all from Sigma)], or endothelial cell growth medium (EGM2-MV; Clonetic), respectively, according to previous methods [10,20]. Adipogenic differentiation lasted for 7 days and the adipocytes were stained with Oil Red O. Osteogenic induction was maintained for 21 days and alkaline phosphatase staining was performed to assess osteogenic differentiation. After 7 days of induction in EGM2-MV, immunocytochemistry was performed to confirm the ability of ADSCs to differentiate into endothelial cells with primary antibody VIII factor (Santa Cruz; 1:50 dilution, 4°C overnight) and secondary antibody-labeled with fluorescein isothiocyanate (FITC).
To determine phenotype characterization, cells were detached with trypsin and were washed with PBS containing 0.2% FBS. Approximately 1 × 105 cells were incubated for 30 min with monoclonal antibodies labeled with FITC or phycoerythrin. Appropriate isotype control combinations were also performed. Antibodies against stem cell antigen-1, CD31, CD45, CD105, and CD29 were from BD Pharmingen. Cells were analyzed on a fluorescence-activated cell sorter instrument (FACS Calibur; BD Biosciences) and data acquisition and analysis were performed using Cell Quest Pro.
Cell labeling and transplantation
One day prior to injection, the confluence cells were labeled with the fluorescent marker CM-DiI-C7001 (5 μM/mL; Molecular Probes, Invitrogen) according to manufacturer's instructions for tracking the cells in vivo. Cells were rinsed, trypsinized, counted, and resuspended in 0.5 mL DMEM for injection. The utilization of DiI as a label for identifying progenitor cells in vivo has been well documented [21 –23]. The labeled ADSCs were also maintained in culture to confirm that the fluorescence did not diminish visibly over time or with cell division. Cells for transplantation were between passages 2 and 3.
Echocardiography
The animals were offered echocardiography examination on 4th, 8th, and 12th weeks after surgery and 2 weeks after cell transplantation (14th week after operation) for detection of the shunt patency and the cardiac function. Animals were anesthetized and immobilized on the bench board. Pulsed Doppler was performed to detect the patency of arteriovenous fistula and pulmonary artery Doppler signals. Two-dimensional or M-mode echocardiograms were used to monitor the cardiac function and the changes in the RV using commercially available equipment (Vevo 770™; Visualsonics). M-mode tracings were recorded at 100 mm/s, on which left ventricular (LV) chamber size, the thickness of the ventricular septum (VS), and the LV posterior wall were measured. Each measurement was repeated for 3 times and the mean value was calculated.
Measurement of pulmonary artery pressure
The hemodynamic data were measured by catheterization. Animals were anesthetized, and first of all, the patent shunt was confirmed by reopening on the left side of neck. Then, a 3F polyethylene catheter was inserted into the right jugular vein and advanced into the RV and to the main pulmonary artery under fluoroscopic guidance. The other catheter was inserted into the right common carotid artery to monitor the systemic pressure (SP; including diastolic SP, systolic SP, and mean SP). These 2 catheters were linked to a transducer and the pulmonary arterial pressure (PAP; including diastolic PAP, systolic PAP, and mean PAP) and SP were simultaneously recorded on a multichannel physiologic recorder (Powerlab8/30; AD Instruments Pty Ltd.). The displayed digits were recorded for 3 times per animal and the average pressure was regarded as the respective indicators.
Preparation of heart and lung tissues
After measurement of catheterization, rats were sacrificed with an overdose of pentobarbital sodium. The lower lobe of left lung was resected and fixed with 4% paraformaldehyde for morphology analysis after paraffin embedding. A part of the upper lobe was removed and embedded in Tissue Freezing Medium (OCT Compound; Sakura) to obtain frozen slice, to detect the engrafted cells or for immunohistochemistry. The residual lung tissues were put into liquid nitrogen for polymerase chain reaction (PCR) and western blot. The heart was weighed after the liquid was blotted for comparison of the weight of heart/body. Then, the heart was divided into the RV and LV+VS, and the weight ratio of RV/(LV+VS) was calculated to evaluate the hypertrophy of RV.
Morphology and immunohistochemistry analysis
The paraffin slice was stained with hematoxylin–eosin and the changes of the small arteries in the lung were observed under optical microscope (Olympus BX51). The vessels between 50 and 200 μm in external diameter (ED) were chosen randomly under low-power fields for the analysis of medial hypertrophy. ED and medial thickness (MT) were measured, and the remodeling of arterioles was calculated as percent MT (% MT = 2 × MT/ED × 100) as described previously [24]. For immunohistochemistry test, the slice was treated with hydrogen peroxide, blocked with 5% bovine serum albumin, and then incubated with the primary antibodies (rabbit anti-HGF and anti-factor-VIII polyclonal antibodies; Santa Cruz Biotechnology) overnight at 4°C. After the uncombined primary antibody was washed, the slice was incubated with horseradish peroxidase–conjugated goat anti-rabbit IgG for 30 min at 37°C. The primary antibody was substituted by PBS for negative control. Peroxidase activity was visualized by a color reaction with diaminobenzidine and a positive result was represented by brown color. The slices were counterstained with hematoxylin and mounted. The protein levels were quantified by Image Pro Plus 6.0 system. The number of factor-VIII–positive arteries that were >50 μm in diameter was counted under a microscope for 10 randomly selected fields per specimen. The arterial density was determined as the average number of factor-VIII–positive arteries along terminal bronchiole per mm2. The pathologist reviewing the sections was blind to the experimental group. FITC-conjugated goat anti-rabbit secondary antibody was also used for immunofluorescence analysis.
Real-time reverse transcriptase–PCR analysis
Total RNA was drawn from the lung tissue using TRIzol Reagent (Invitrogen) and quantified. Then, the total RNA was reverse transcribed to cDNA by using M-MLV reverse transcriptase (Bio-Rad). An aliquot of the resulting cDNA was amplified by real-time reverse transcriptase (RT)-PCR using SYBR Green I (TaKaRa Biotechnology) as a double-stranded DNA-specific dye according to the instructions. The sequence-specific primers of HGF are as follows: forward, 5′-TCAGCACCATCAAGGCAAGG-3′; reverse, 5′-CAGGAACAATGACACCAAGAACC-3′. Primers of eNOS were as follows: forward, 5′-TGGCTGTCTGCATGGACCT-3′; reverse, 5′-TGGTSACTTTGGCTAGCTGGT-3′. For β-actin, the primers were 5′-ACCCGCGAGTACAACCTTCTTGC-3′ (forward); 5′-TTGCACATGCCGGAGCCGTT-3′ (reverse). The programs were designed for 40 cycles in a PCR instrument (Lightcycler 2.0; Roche). Each sample was repeated for 3 times and the levels of mRNA were expressed relative to the levels of internal reference, β-actin.
Western blot
Protein was drawn from 20 mg lung tissues on ice by treatment with lysis buffer and phenylmethanesulfonyl fluoride (PMSF) (both from Beyotime). The protein supernatants were centrifuged at 10,000 rpm for 10 min (4°C) to remove the tissue fragments of the sediments. Concentrations of protein were determined by the Bio-Rad protein assay instrument and the protein was boiled with loading buffer. Equal amounts of protein from all the lung tissues were dissolved in SDS-PAGE sample buffer, separated in SDS-PAGE, and transferred onto polyvinylidene fluoride membrane. The membranes were incubated with the respective primary antibodies (rabbit-anti HGF and rabbit-anti eNOS both from Abcam Co.) overnight at 4°C after being blocked with 5% fat-free milk for 2 h. The blots were incubated with secondary antibodies conjugated to horseradish peroxidase for 1 h at room temperature with continuous shaking. After washing, the protein blots were detected using an enhanced chemiluminescence kit (Millipore) and exposed to X-ray film. The recognized bands were quantified by Fluor Chem 9900 (Alpha Innotech) and β-actin was used as an internal reference.
Enzyme-linked immunosorbent assay
Conditioned medium was collected from ADSCs (between passages 2 and 5) cultured in normoxia (21% O2, 5% CO2) or hypoxia (1% O2, 5% CO2) for 24 h. Concentrations of HGF proteins in the cell supernatant were determined by enzyme-linked immunosorbent assay (ELISA, Rat HGF ELISA kit; R&D) according to the manufacturer's protocols. Before cell transplantation, 2 mL blood was drawn through the right jugular vein for determination of plasma HGF. At the end of catheterization, blood was also collected for analysis of HGF plasma levels.
Statistical analysis
SPSS 13.0 for windows was used for all statistical analysis. Variables were presented as mean ± standard deviation. Comparisons between 2 groups were made by Student's t-test. For >3 groups, one-way analysis of variance with a post hoc test of LSD test was used for the statistical analysis. P < 0.05 was considered as significantly different.
Results
Morphology and characterization of ADSCs
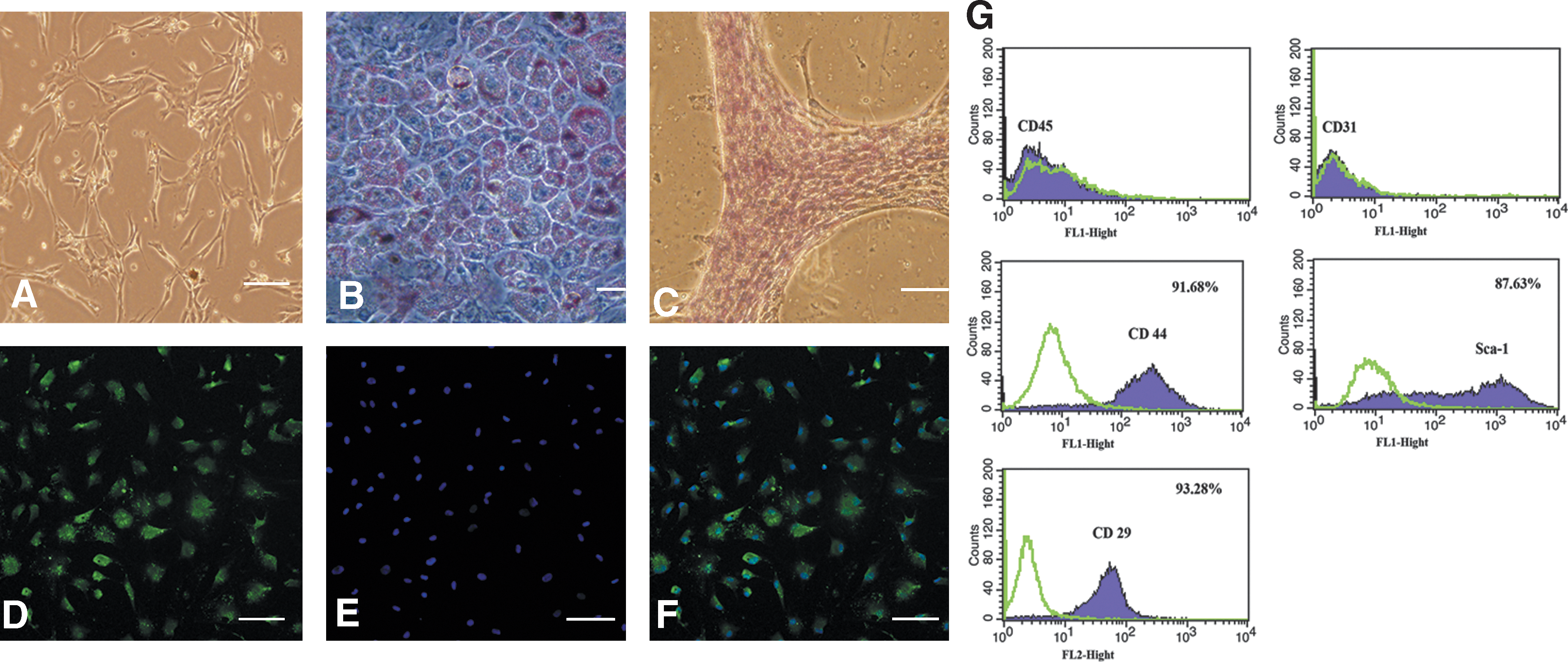
ADSCs obtained from the inguinal adipose exhibited a fibroblast-like morphology (Fig. 2A), had the ability to self-renew and adhere to plastic, and extensively expanded in culture without loss of differentiation potential. These cells could be induced into mature adipocytes, which were confirmed by microscopic observation of intracellular lipid droplets after Oil Red O staining (Fig. 2B). ADSCs also differentiated into osteoblasts, which were evaluated by alkaline phosphatase staining (Fig. 2C). After 7 days of culture in EGM2-MV medium, immunocytochemistry revealed that these cells showed a positive signal for factor-VIII in vitro (Fig. 2D–F). Fluorescence-activated cell sorter analysis showed that the cultured ADSCs were positive for stem cell antigen-1, CD29, and CD105, but negative for CD31 and CD45 (Fig. 2G) as reported previously [16,25].
Labeling rate and the result of injected cells
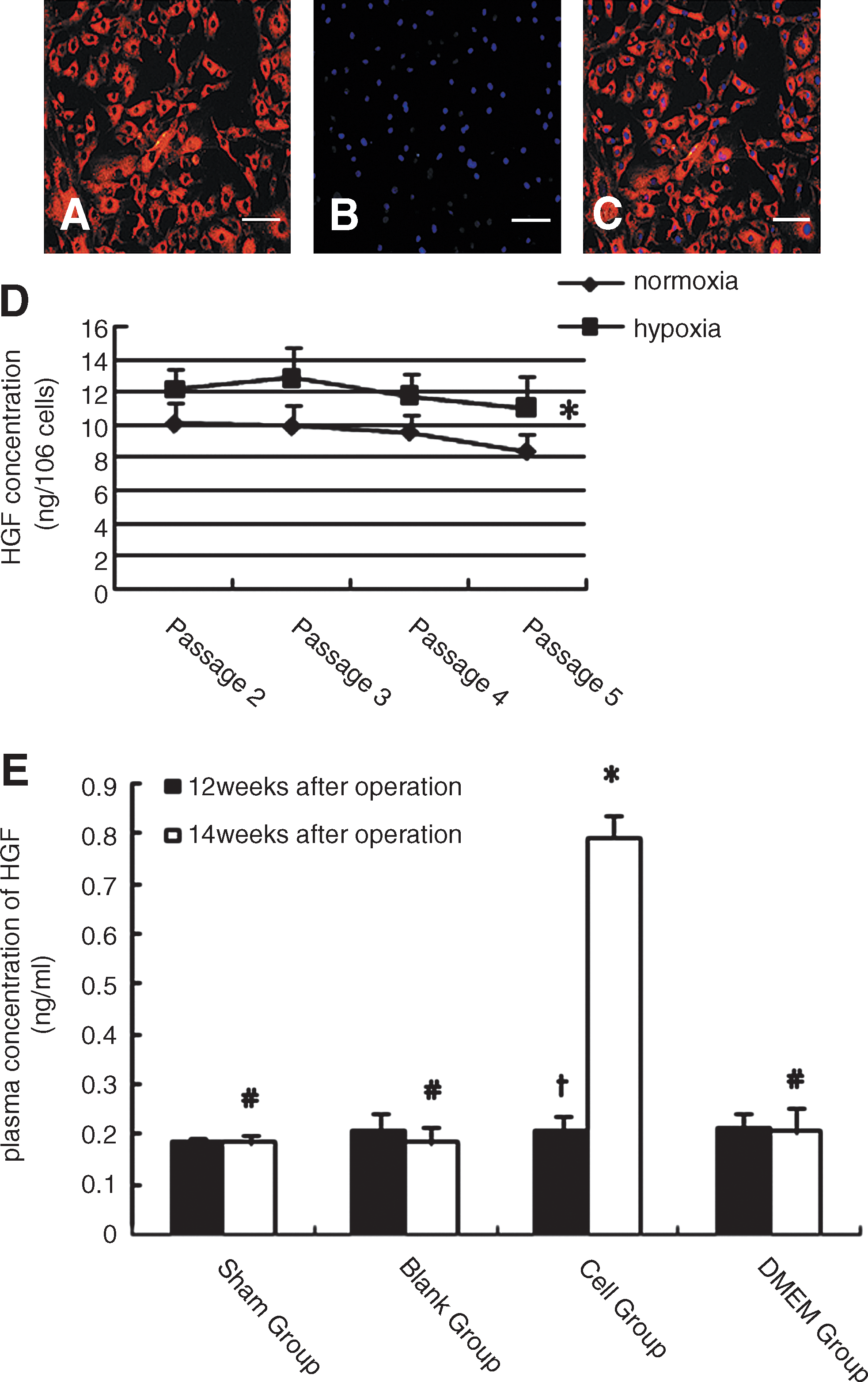
Cells labeled with CM-DiL (C7001) were assessed by fluorescence microscopy and the high labeling rate was maintained for several passages. More than 99.5% cells were labeled under each low-power visual field (Fig. 3A–C).
High labeling efficiency of ADSCs with CM-Dil in vitro before transplantation.
No animal died or suffered from other disorders after cell transplantation, suggesting that the cell therapy could be accepted without any adverse response. The frozen slice analysis revealed that the engrafted cells in the lung almost located in the surroundings of the capillary vessels and alveolar wall after 2 weeks.
HGF levels in conditional medium and plasma
ELISA curves demonstrated that ADSCs could secrete HGF under FBS-supplemented condition. Higher level of HGF was detected in cells between passages 2 and 5 under hypoxia condition than under normoxia condition. In addition, the lower the passage, more release of HGF was detected. ELISA results for cell supernatant suggested that hypoxia could enhance the release of HGF in ADSCs (Fig. 3D).
Before cell transplantation, the plasma level of HGF in the sham group was a little lower than that in other groups in which the rats suffered shunt surgery, but there were no statistical difference among all the groups (Fig. 3E). Two weeks after cell transplantation, HGF concentration was much higher in the cell group than the baseline level. In contrast, HGF levels in the blank and DMEM groups were a little lower than their baseline levels (12th week after surgery), but the differences were not statistically significant. No evident changes in the sham group were observed.
Engraftment of ADSCs improved the hemodynamic abnormality in PAH rats
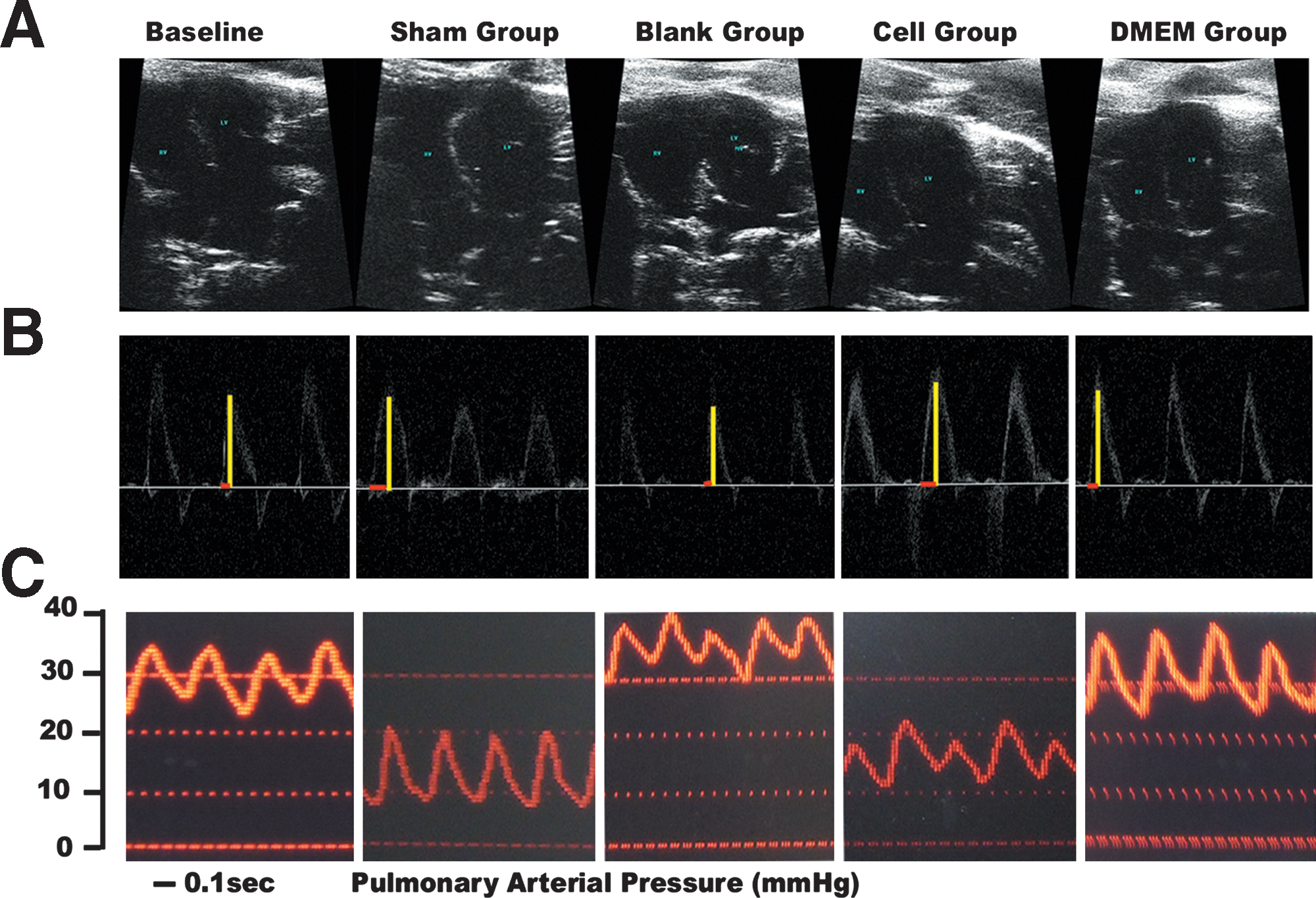
Five rats died during and after surgery because of anesthetic or operation accident. Eight rats undergoing surgery were excluded from the experiment because occlusion of the shunt was found during the echocardiogram exam at 4 weeks after operation. The anterior wall of RV was thickened with prolonged time after operation in the rats suffering shunt surgery, which was confirmed by echocardiographic examination (data not shown). After cell engraftment, the thickness of RV free wall in the cell group (n = 16) was slightly thicker than that in the sham group (n = 19) (0.946 ± 0.204 mm vs. 0.891 ± 0.056 mm, P > 0.05), but became thinner compared with the baseline level (before cell treatment) (0.946 ± 0.204 mm vs. 1.133 ± 0.217 mm, P < 0.05). In the blank group (n = 17) and DMEM group (n = 15), the RV anterior wall became thicker compared with the cell group (1.134 ± 0.112 mm vs. 0.946 ± 0.204 mm, P < 0.05; 1.121 ± 0.124 mm vs. 0.946 ± 0.204 mm, P < 0.05, respectively) and changed slightly compared with the baseline level (1.134 ± 0.112 mm vs. 1.133 ± 0.217 mm, P > 0.05; 1.121 ± 0.124 mm vs. 1.133 ± 0.217 mm, P > 0.05, respectively). The thickness ratio of RV free wall to the LV posterior wall (RV/LV) in the blank and DMEM groups was greater than that in the cell group (0.493 ± 0.071 vs. 0.426 ± 0.187, P < 0.05; 0.489 ± 0.068 vs. 0.426 ± 0.187, P < 0.05, respectively). Compared with baseline level, the thickness ratio of RV/LV decreased (0.426 ± 0.187 vs. 0.494 ± 0.144, P < 0.05) after cell transplantation. In the apical 4-chamber view, the enlargement of RV or the deviation of VS to LV was also ameliorated in the cell group (Fig. 4A). The high pulmonary arterial resistance was improved by cell implantation, which was also confirmed echocardiographically. The pulmonary artery acceleration time (the time from the beginning to the peak of the velocity envelope during pulsed Doppler interrogation of the pulmonary valve) was shorter in the baseline level, blank group, and DMEM group than in the cell and sham groups (generally, the high the PAP, the shorter will be the pulmonary artery acceleration time [24]). The shape of the pulmonary arterial blood flow in Doppler was like a dagger in the blank and DMEM groups (Fig. 4B). This was the specific wave in PAH. The dagger-like waves shown before cell treatment were changed into normal waves like in the sham group, suggesting the reversion of high resistance in pulmonary artery after cell transplantation.
Echocardiographic representations.
Measurement of catheterization revealed that in the cell group, mean pulmonary pressure was lower than the baseline level (Fig. 4C). There was no difference in the SP expressed by carotid arterial pressure among these groups. The weight ratio RV/(LV+VS) in the cell group was lower than that in the blank group, DMEM group, and baseline level, but almost at a same level as in the sham group. There was no difference in the rate of heart/body weight among these groups (Table 1). All the results mentioned above suggested that shunt flow induced high pressure or high resistance of pulmonary arteries. The increased PAP, the enlargement and hypertrophy of RV were reversed after ADSC transplantation.
P < 0.05 versus sham group.
P < 0.05 versus baseline.
DMEM, Dulbecco's modified Eagle's medium; dPAP, diastolic PAP; LV, left ventricle; mPAP, mean PAP; PAP, pulmonary arterial pressure; RV, right ventricle; sPAP, systolic PAP; VS, ventricular septum; mSAP, mean systemic arterial pressure.
ADSC transplantation ameliorated the remodeling of the arteries in PAH and augmented the expression of HGF in the lung
As predicted by the hemodynamic data, hematoxylin–eosin staining demonstrated that the obliterative remodeling of the small arteries occurred in the lung after shunt surgery and cell transplantation could attenuate the remodeling of the arteries (Fig. 5A, C). Before cell treatment, the small arteries in PAH rats showed an obviously medial hypertrophy and hyperplastic response in pulmonary arterioles. Further, lung consolidation could be observed in some areas of the slices under light microscope, which might be caused by inflammation, an important factor in the development of PAH. Two weeks after cell transplantation, the concentric hypertrophy of the arterioles was attenuated. The reduced remodeling in the arteries might be caused by the cytokines, of which HGF played an important role.
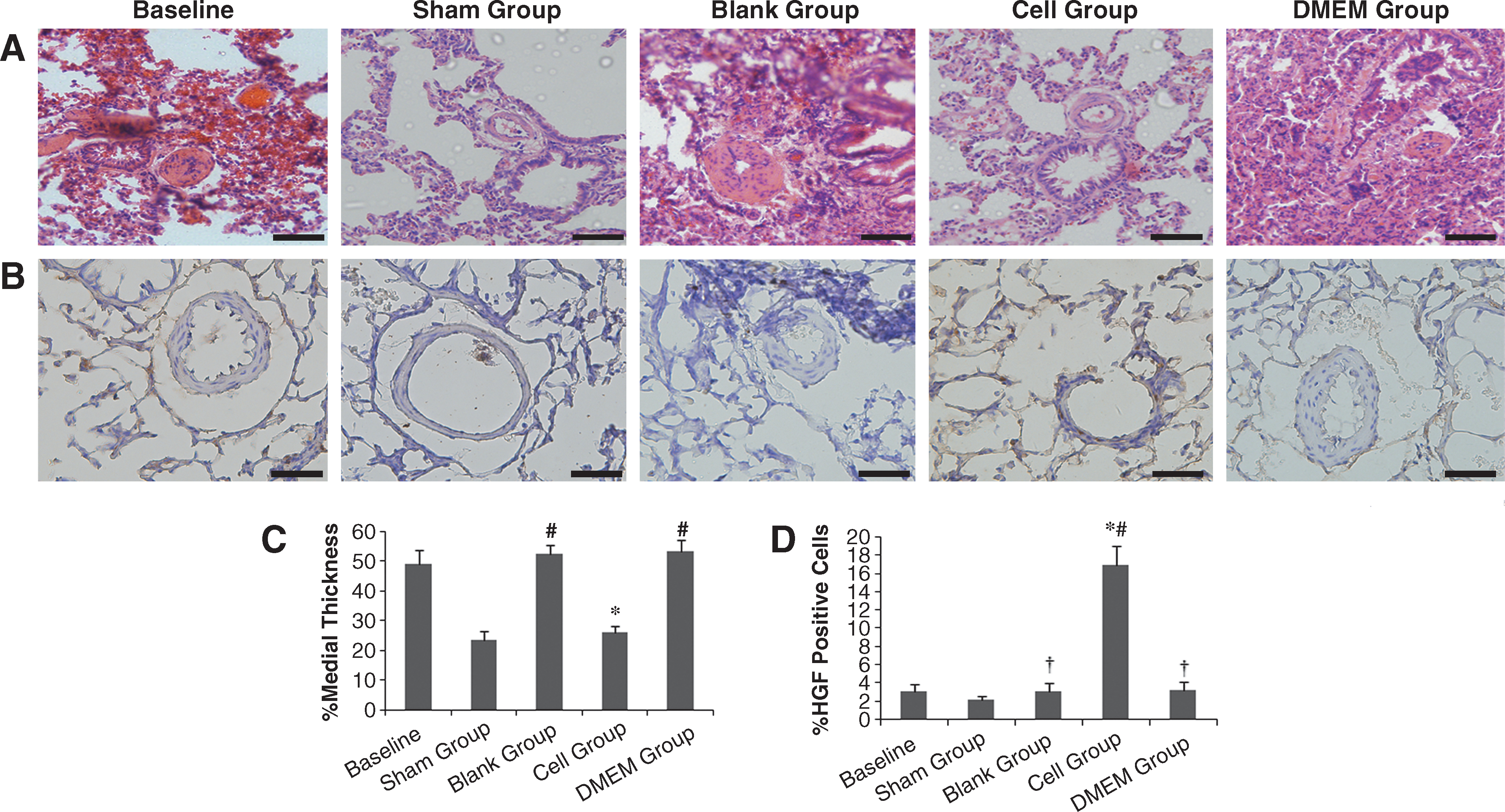
Cell transplantation significantly reduced the remodeling of pulmonary arterioles compared with the baseline, blank group, and DMEM group.
HGF in the lung was extensively identified in the cytoplasm at 2 weeks after cell injection. In the sham group, no obviously positive cells were found, suggesting that there was little expression of HGF in the normal lung tissue. Semiquantitative evaluation of the immunohistochemistry slices indicated that the implantation of ADSCs enhanced the expression of HGF in the injured lung compared with the baseline level as well as the sham group. In the blank and DMEM groups, the expression of HGF was lower than that in the cell group (P < 0.01) but a little higher than the sham group (P > 0.05; Fig. 5B, D). To determine whether the engrafted cells could secrete HGF in vivo, immunofluorescence was performed using rabbit-anti HGF as primary antibody and FITC-labeled goat-anti rabbit IgG as secondary antibody. The immunofluorescence results showed that the transplanted ADSCs secreted HGF even in vivo (Fig. 6A–E). Factor-VIII immunofluorescence staining showed no obviously positive signal in the implanted labeled cells. Factor-VIII immunohistochemistry analysis demonstrated obviously higher capillary density in the cell group than in the blank and DMEM groups, which indicated increased number of small arteries in the lung caused by cell transplantation (Fig. 6F).
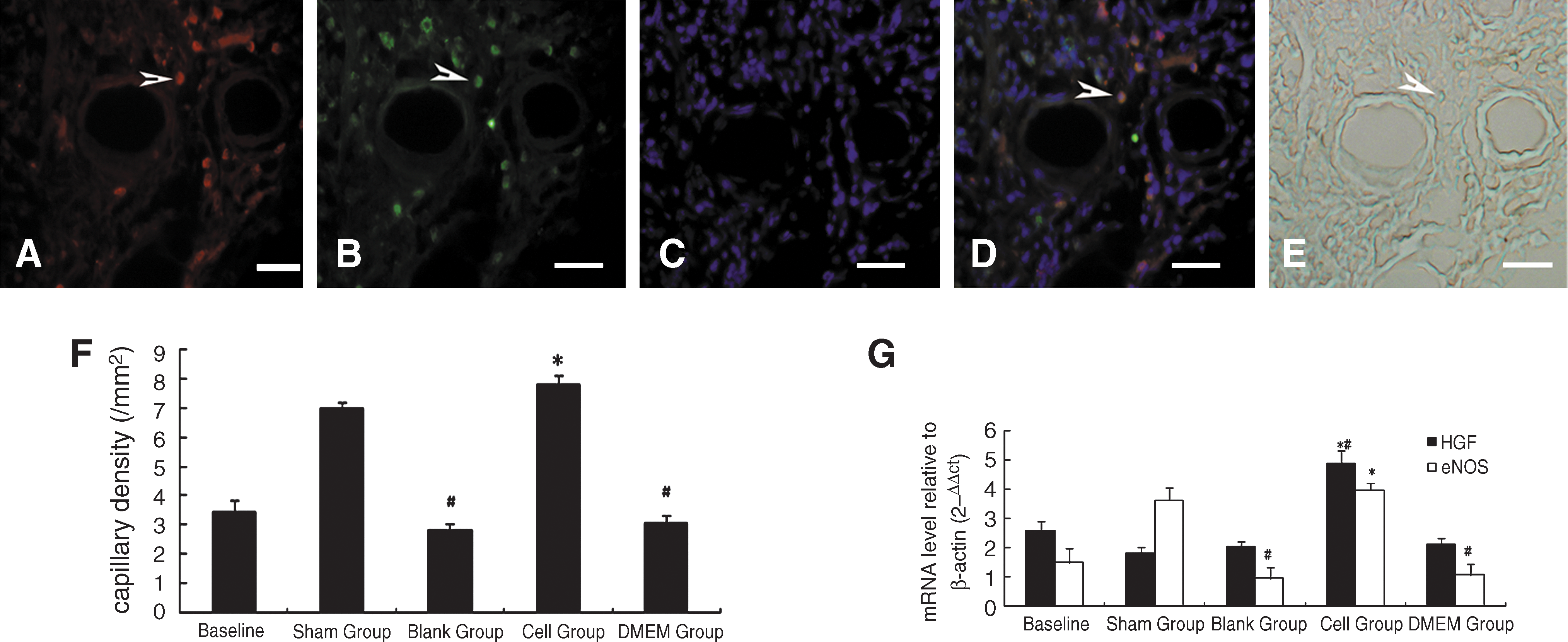
Immunofluorescence images suggested that the engrafted ADSCs secrete HGF in vivo (× 60).
Because eNOS was regarded as a key factor in the pathology of PAH, it was selected to reveal the relationship between the increased HGF and the pathological changes in PAH. We investigated whether ADSC transplantation could increase the mRNA levels of HGF and eNOS. Real-time RT-PCR analysis showed that HGF mRNA abundance increased obviously in the cell group. In contrast, there were slight HGF expressions in the blank and DMEM groups as well as in the baseline level. Notably, the eNOS mRNA levels positively correlated to HGF mRNA levels after cell transplantation (Fig. 6G).
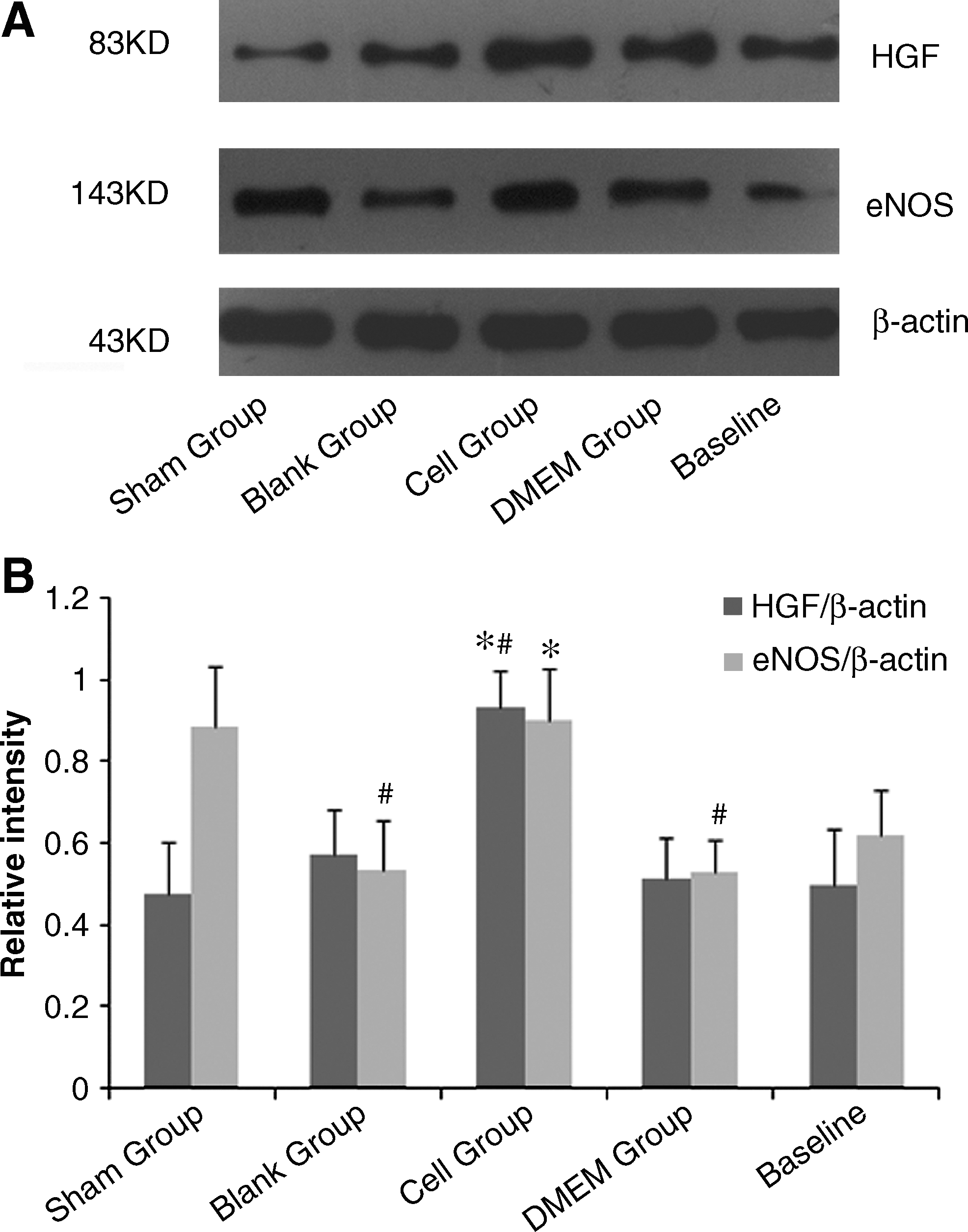
As the results of real-time RT-PCR, western blot analysis also displayed the enhancement of HGF expression and the increased expression of eNOS in the cell group. Strong bands were detected in the cell group and weak bands were shown in the baseline level (Fig. 7A, B). All the results suggested that autologous ADSC transplantation increased the expression of HGF in the PAH lung and subsequently elevated the eNOS expression, which led to the attenuation of the PAH.
Discussion
In present study, we have demonstrated that autologous transplantation of ADSCs ameliorated PAH via HGF augmentation and angiogenesis promotion. The following evidences supported the conclusions: (1) the injected ADSCs could be observed in the lung tissue and the HGF-positive signal was detected in the transplanted cells. (2) ADSCs secreted HGF in vitro, especially in a hypoxia environment. Transplantation of cells demonstrated an increased HGF expression in the lung with PAH. (3) Decreased pulmonary resistance, reversed remodeling of the arteries, and hemodynamic improvement were noticed after cell transplantation. (4) A significant increase in the number of factor-VIII–positive capillaries was observed after cell transplantation.
Using a rat as the experimental subject, an arteriovenous shunt was made in the neck to intimate left-right shunt in congenital heart disease. We constructed a successful model of pretricuspid valve shunt. During the operation, the artery was connected to vein in a cuff style so that the folded intima of artery faced the intima of vein to ensure low occurrence of thrombosis. Small animal echocardiographic examination not only provided the patency of the shunt but also showed the changes of the cardiac function and the frequency spectrum of blood flow, which indirectly reflects the resistance of pulmonary artery. Our preliminary experiment showed that a successful PAH rat model induced by shunt could be established at 3 months after surgery and the pathological changes in pulmonary arterioles could be observed even after the first month (data not shown). In our study, although the establishment of PAH needs a relatively long time, pathological analysis indicated that arteriovenous shunt might be a feasible model of PAH in small animals, with low mortality, less invasion, and relatively high patency rate.
Cell-based therapy opened a new therapeutic avenue for treatment of PAH. ADSCs derived from adipose tissues are capable of differentiating into several mesodermal lineages including endothelial cells and have demonstrated many advantages over other adult stem cells [26]. The cells were isolated and cultured in vitro for extensive expansion. It retains stem cell phenotypes and mesenchymal pluripotency even at high passages [9]. In our study, cells of passage 2 or 3 were transplanted to obtain more vigorous self-renewal. Further, the younger the cell, the more HGF was secreted in vitro. In addition, cells under hypoxia condition tend to release more HGF than those under normoxia condition. In this report, the cells were injected to locate in the lung, to play their role. Injection through jugular vein ensured that most of the transplanted cells could retain in the lung. There were 2 explanations: first, through this way, the lung was the first organ the cells encountered except for the heart, whereas through tail vein more cells would retain in the liver; second, the lung injury could “trap” the cells into the lung tissue through some cytokines such as stromal derived factor (SDF), which was produced under hypoxia condition or injury by the local tissue. In our early experiment, we also tested the distribution of the implanted cells in some organs by this injection pathway, such as in liver, spleen, kidney, and lung, at different time points. The preliminary results indicated that most cells were retained in the lung and few were observed in other organs at an early stage (24 h after injection; data not shown). At a late stage (14th day after injection), only 68% of injected cells could be found in the lungs and few cells were detected in the liver. After cell transplantation, no death or other dysfunction happened in the rats, suggesting that the cells could be accepted without side effects. There was no histological abnormality detected in the lung tissue and other organs, which was in coincidence with a previous report [27]. In the frozen slice of the lung, transplanted cells could be observed in the perivascular site, but there was no obvious vascular-like structure constructed by these transplanted cells. This phenomenon was in conformity with Kazuhisa's [14] study. To explore the concealed mechanisms, we focused on HGF, which was the cytokine most secreted by ADSCs, exerting organotrophic and protective effects on the injured lung. Other cytokines released by ADSCs, such as vascular endothelial growth factor, are also known to act in a synergistic manner with HGF in angiogenesis [28]. Further, immunofluorescence analysis of HGF showed that these cells could secrete HGF in vivo. Western blot and real-time RT-PCR also demonstrated the enhanced expression after cell transplantation. The significant increase of HGF after cell treatment might be caused by the enhanced secretion of engrafted cells under hypoxia condition.
It is known that HGF exists in the plasma at a low level in normal body, which was confirmed in the rats of the sham group. After shunt surgery, there was a little higher concentration of HGF than the sham group, and this could be explained as the compensation mechanism responding to the injury condition. However, the elevated level of HGF was far from its effectual bioactivity.
HGF as a potent mitogen has demonstrated the ability to promote angiogenesis after trans-pulmonary arterial transfection of HGF gene into the lung, to increase capillary density and blood perfusion, and to decrease vascular resistance when blood flow was increased [29]. In our study, the benefit of augmented HGF was also confirmed in the injured lung induced by hyperkinetic blood flow. It has been proved that HGF increased the endothelial NO generation and phosphorylation of eNOS [17]. In addition, dysfunction of the endothelia resulted in decreased production of NO, which was important in the development of PAH. Therefore, the expression of eNOS was investigated after cell transplantation to determine whether HGF augmentation could recover the injured endothelium and evoke the generation of eNOS. As we predicated, results showed an increased production of eNOS with the enhancement of HGF at 2 weeks after cell implantation. We thought that transplantation of ADSCs not only induced angiogenesis but restored the shunt-induced endothelial dysfunction in the lung via the secretion of HGF.
The limitation of this study was the short time frame of investigation of the effect of ADSC transplantation on PAH. Further, the side effects of cell transplantation should also be concerned in further studies.
Conclusions
ADSC transplantation ameliorates the PAH induced by shunt flow. Transplanted ADSCs improved the hemodynamics of PAH through secretion of HGF, subsequently restored endothelial dysfunction, and induced angiogenesis in the injured lung. Transplantation of autologous ADSCs might be a promising therapy for PAH.
Footnotes
Acknowledgments
The authors thank Shanying Huang (pathologist) for providing kind instructions on histological analysis. The authors also thank Yun Ti and Zhihao Wang for performing the animal echocardiography examination.
Author Disclosure Statement
No competing financial interests exist.