
Abstract
Diseases of the digestive tract are complex and encompass a broad spectrum of different pathogeneses (inflammatory, ischemic, neoplastic, and functional deficit). The digestive tract is not a sterile environment, and its organs are composed of tissues with different embryologic origin and different morphologic and functional complexity. As a consequence, the management of these diseases is often challenging. Stem cell (SC) therapy has yielded some promising results in preclinical studies, and, recently, some approaches have been tested clinically. Indeed, during the last 5 years, the number of clinical trials with SCs for treatment of digestive tract diseases has increased 10-fold. The most advanced programs involve liver failure, Crohn's disease, and fistulous disease and are now in phase III of development. If progress continues and the preliminary results are confirmed, SC therapy will become a clinical reality in the near future.
In this review we examine the basic concepts of the SC therapy, analyze the potential benefits of SCs in diseases of the digestive tract, and summarize current experience in the field and the future perspectives.
Introduction
S
The aim of this review is to analyze the potential benefits, the state of the art, and the perspectives regarding SC therapy for digestive tract diseases, an emerging topic in SC therapy. There are not many reviews covering this issue published. Some promising results have been obtained in animal models and some approaches have been tested clinically with encouraging findings, but the practical utility of these cells in humans has yet to be established.
SC Properties of Therapeutic Potential
In view of their differentiation and proliferation properties (both in basal situations and through lesion-induced activity, with a certain capacity for regeneration) resident SCs participate in the homeostasis of the organism. Clear examples can be found for resident SCs of the epithelial and mucous surfaces (including gastrointestinal), blood, liver, etc. This capacity has been used in a clinical setting for the last 40 years in hematopoietic SC (HSC) transplantation in hematologic diseases. More extensive applications have been suggested by the following recent findings: Presence of SCs in practically all adult organs, especially the brain [2], heart [3], and skeletal muscle [4]. Evidence of greater plasticity (differentiation potential) than previously thought. Adult stem cells (ASs), either in vitro or in vivo, can differentiate into cells from other germ layers (transdifferentiation) as shown in several studies with bone marrow (BMSC) [5,6], adipose-derived SC (ASC), and skin SC [7,8]. Therapeutic cloning showing that differentiated cell nuclei can be reprogrammed to behave as totipotent. Such behavior has not yet been achieved in humans, and the limited success of cloning in animal models makes it a less attractive approach for the future. The possibility of obtaining pluripotent cells [known as induced pluripotent stem cells (iPS)] by reprogramming adult cells culturing them under appropriate conditions. iPS cells can differentiate into different cell types (including hematopoietic cells, cardiac myocytes, skeletal muscle, and adipocytes) [9,10], and in animal models, they contribute to tissue formation. Moreover, these cells are not subject to the moral and ethical problems of human embryonic SCs (ESCs) study and use.
In summary, SCs can be obtained from adult tissues directly as ASs, by therapeutic cloning or through iPS cells and can be applied autologously to avoid possible rejection (with or without prior differentiation).
With regard to digestive tract diseases, initial studies suggested that AS plasticity represented their principal mechanism of action. In liver injury, there is literature supporting use of both HSCs (eg, see refs. 5 and 11) and MSCs (eg, see ref. 12), although the evidence is probably more compelling for MSCs [13]. Many groups have suggested that fusion of ASs with endogenous hepatocytes is the dominant mechanism by which new hepatocytes are produced [14]. Irrespective of the mechanism, the number of hepatocytes produced is likely to be very low in the vast majority of situations and so the production of new hepatocytes will have little clinical impact [13]. In the gastrointestinal tract, data suggest that certain BMSCs can either fuse with intestinal epithelial cells or become transformed into epithelial cells [15,16] with a variable participation of both mechanisms.
Apart from their differentiation and proliferation properties, SCs carry out other important potentially therapeutic functions: Regulation of other cells by molecular signal mediators or through cell-to-cell interactions. For example, MSCs inhibit local immune response, prevent excessive fibrosis and apoptosis, and induce mitosis of the progenitor cells [17]. Applied to digestive diseases, SC infusions are thought to stimulate the reduced proliferation capacity of endogenous hepatocytes through a paracrine mechanism. The proposed mechanisms are release of proliferative cytokines, enhanced breakdown of scar tissue, or promotion of angiogenesis [13]. For stimulation of proliferation, there is much more evidence for effects with HSCs [18] than with MSCs. For antifibrotic effects, the literature supports both HSCs and MSCs and endothelial progenitor cells [19]. Immunomodulation: This has been observed mainly with BMSCs and ASCs, which can inhibit certain B-, T-, and natural-killer-cell functions and may affect dendritic cell activity [20]. Further, such cells exhibit low immunogenicity, even in HLA incompatible hosts, due to expression of low-moderate levels of HLA-I, low levels of HLA-II, and low levels of costimulatory molecules [21]. Proangiogenic: SCs participate in the formation of new vessels [22] either by direct differentiation or through mediator release. Homing to damaged tissues. For instance, human MSCs are found essentially in radiodamaged tissues in animal models of radiation injury [23,24].
Choosing Type of SC for Treatment of Digestive Diseases
Unfortunately there is no such thing as an ideal SC showing optimal results for general use. The specific aims should be studied for each indication to choose the most appropriate cell type. We now briefly describe the main properties of the different SC types that have been considered for preclinical and clinical applications in digestive tract disease, with focus also on those cells located in digestive tract.
Embryonic stem cells
Although ESCs may seem suitable as they are pluripotent and practically immortal, there are three main problems that do not arise with ASs: the risk of tumor formation (teratomas appear when applied in vivo, as with iPS cells), the immunologic barrier (except therapeutic cloning), and difficulties and the cost involved in their production. Therefore, they tend to be used in research as a source of basic knowledge, whereas almost all clinical trials are carried out with ASs, which also avoid the associated ethical problems.
Adult stem cells
SCs from BM (BMSCs): BM contains several AS types; the most used are HSCs, BM-derived mesenchymal stem cells (BM-MSCs), and endothelial precursor cells. But there are other additional cell populations like side population (SP), with mainly myogenic potential, multipotent adult progenitor cells (MAPC, pluripotent), etc.
Adipose-derived mesenchymal SCs (ASCs): These cells, obtained from the stromal-vascular fraction (SVF) of lipoaspirates, were first described for humans in 2001 [25]. They are being increasingly used due to their similarities with BM-MSCs, ease of preparation, and high yield.
MSCs possess substantial differentiation and replication potential (at least in vitro) and antiproliferative and anti-inflammatory activity (in vivo and in vitro), which, together with their privileged immunologic properties, make them safe for allogeneic use. They are also easy to transfect and tolerate cryopreservation well.
Gastrointestinal SCs (GISCs): These multipotent SCs, housed in specific niches within gastric glands and intestinal crypts give rise to various cell types in the gut through committed precursor cells [26]. These gastrointestinal SCs have been identified in small bowel [27] and also in the colon (at the bottom of each crypt) [28] and stomach [29]. BM-derived cells could play an important role in this niche (differentiating into intestinal subepithelial myofibroblasts) as has been seen in male BM transplants in female mice and in female patients with graft versus host disease receiving male BM transplant [30].
Finding good markers for these cells has proved very difficult. The most widely accepted one is Lgr5, which allows identification of cript base columnar cells of small bowel [28]. Such cells are also frequently positive for Ki67 and occasionally express the M-phase marker phospho-histone H3. With long-term culture, single lgr5+ SCs generated crypt–villus organoids that included all differentiated cell types and maintained the basic epithelial architecture [31]. Colon SCs were more often quiescent than their small-intestinal counterparts [28]. In the stomach, Lgr5 cells are able to generate long-lived organoids resembling the mature pyloric epithelium [32]. Lgr5 and 6 are unique markers in that they can be used to discriminate SCs from their immediate daughters [33]. Other candidate markers, such as Musashi or CD133 [34], are expressed to a lesser extent in crypt axis. Doublecortin and calcium/calmodulin-dependent kinase-like-1 is a marker of precursor cells able to form spheroids [35], but different to stem. OlfM4 is expressed robustly by gastrointestinal SCs in mouse and human [36].
Liver SCs: The liver has cells that can give rise to either hepatocytes or cholangiocytes known as liver progenitor cells (LPCs), facultative liver SCs, or oval cells in rodents. They become activated during liver injury combined with an inability of hepatocytes to repopulate liver. Their presence correlates with chronic liver disease severity. There are three putative locations: canals of Hering, the interlobular bile ducts, and periductular sites. Several types of stromal cells could be their partner cell, for example, hepatic stellate cells and portal myofibroblasts [37]. The origin of LPCs remains controversial [13], with some groups suggesting that they may arise in part from BM-derived SCs [38], whereas others defend their hepatic origin [39]. Circulating cells can contribute to hepatic mass by direct differentiation (which seems to occur at a very low rate) or by cell–cell fusion. A recent article identified these cells in normal rat liver; they express typical hematopoietic (CD34, CD45, Sca-1, cKit, and Thy-1) [40] as well as some endodermal markers. Similar cells have been identified in human liver sorting Thy-1-positive cells [41]. The actual origin of LPCs is still under investigation; they could be native to the liver, or arise from extrahepatic SCs [42] or even from parenchymal liver cells by an epithelial to mesenchymal transition [43]. The real role of these cell populations under physiological or pathological conditions in humans is not well understood and much work is directed toward clarifying this issue. The regeneration capacity of the liver without the participation of these cells is well known as we will discuss later.
Induced pluripotent SCs
These cells were first described in 2006, obtained by retroviral transduction of 4 transcription factors (Oct3/4, Sox2, c-Myc, and Klf4) into murine fibroblasts [9,10]. In 2007 they were obtained from human skin fibroblasts. During 2009, researchers excluded different transcription factors from the protocol, used transposons and less differentiated cells (such as MSCs) for reprogramming [44,45].
Conclusions about stem cell sources for digestive diseases
In theory, none of these sources would be clearly preferable for general use in diseases of the digestive tract given that the specific embryogenesis for each organ would need to be taken into account. General considerations about accessibility aside, no type of cell has been shown to be superior for this multilayer repopulation. Analysis of studies of the digestive tract highlight in particular the use of BM cells (HSC and BM-MSC) and adipose tissue, the former because they have traditionally been used in other applications and the latter because of the ease with which they are obtained. Table 1 compares these cell types.
ASCs, adipose-derived stem cells; BM-MSCs, bone-marrow-derived mesenchymal stem cells; HSCs, hematopoietic stem cells; SCs, stem cells; G-CSF, granulocyte colony-stimulating factor.
Particular Characteristics of Digestive Diseases of Significance for SC Therapy
In recent decades, advances in surgical and anesthetic techniques, antibiotic therapy, cancer therapies, and perioperative care have improved outcomes in digestive surgery. Despite these advances, clinical challenges remain and SC therapy may play an important role in certain situations that can be divided into the following categories.
Inflammatory-infectious disease
The immunomodulatory capacity of some types of SC might alter the course of inflammatory or infectious disease. One possible application would be perianal fistulizing disease, which, despite complex surgery, recurs frequently (22%–45% for advancement flap technique) and which is also associated with non-negligible risk for incontinence [46].
Another application could be chronic idiopathic inflammatory bowel disease, which shows only limited response to surgery, with appreciable failure rates, short-term complications, and recurrences.
Another broader application could be suppression of the rejection of abdominal solid organ transplantations given that there has been recent success at reducing acute graft-versus-host disease by injection of BM-MSCs [47].
Radiation damage
Acute or chronic intestinal damage occurs in 10%–20% of patients who have undergone abdominopelvic radiotherapy. It often results in severe mucosal atrophy with enteric dysfunction and a risk of germline translocation. Few therapeutic options are available for such damage and outcomes are poor with a low quality of life for patients.
Neoplastic disease
Tumors remain a controversial topic in SC therapy; fully conclusive studies to confirm whether SCs might be tumorigenic or modify the course of neoplastic disease are lacking. There are articles in the literature that support both possibilities, although most rule out the tumorigenic potential of ASs reported for ESCs. Neoplastic disease is, nevertheless, usually considered an exclusion criterion in SC therapy trials.
Recent in vitro and in vivo studies have investigated the behavior of ASCs in the presence of tumor cells; these have found migration toward the tumor and, in some cases, acceleration of tumor growth [48,49] but also death of neoplastic cells [50,51], so the clinical significance of these findings is unknown. Some authors have explored the possibility of using this migratory capacity as a delivery vehicle for drugs or cytotoxic genes [52].
Currently, the most realistic application in digestive neoplastic disease would be transplantation of hematopoietic progenitors as rescue from BM ablation caused by adjuvant treatment [53,54].
Ischemic disease
This is characterized by the low availability of specific treatments. The most beneficial potential effect would be proangiogenesis. SCs might have an important role, as in treatment of critical ischemias of limbs [55] and myocardial [56] and cerebral ischemic disease [57].
Functional deficit
Functional deficits are characteristic of diseases such as liver cirrhosis, neuronal loss associated with achalasia, Hirschprung's disease, gastroesophageal reflux, and anal incontinence. The potential for differentiation would be the most useful property in such situations. Their paracrine role might also be of use, modulating the niches of resident SCs [58,59].
Correction of functional deficit remains, however, an ambitious objective; currently, most differentiation studies are in vitro observations under controlled conditions. Differentiation has hardly been observed in vivo, and there are even authors who suggest that fusion phenomena are responsible for what is observed [60,61].
There are some particularities about liver disease that need to be commented at length. Liver regeneration is a process that has been widely studied. Hepatocytes originate from replication of existing hepatocytes, differentiation of LPCs, or from BM cells. Replication of the main epithelial compartments (hepatocytes and cholangiocytes), followed by proliferation of mesenchymal cells (hepatic stellate cells and endothelial cells), is the quickest and most efficient way for liver regeneration and repair as shown in studies of liver resections and hepatocyte cell transplantation [62]. Hepatocytes, which are quiescent in normal livers, have an enormous (compared with another organs cells) but limited capacity to proliferate [63] under certain conditions. This property resembles SC, but the proliferative potential is lesser and hepatocytes do not express telomerase. When the mature epithelial cell compartments are damaged or inhibited in their replication, the reserve LPC compartment is activated [64]. There is evidence that the replicative activity of hepatocytes diminishes in advanced cirrhosis in humans and in chronic liver injury in mice, reaching a state of replicative senescence, perhaps as a consequence of telomere shortening [62,65,66]. These cells could participate in liver regeneration after acute injury and chronic disease, and probably also in hepatic carcinogenesis [67 –69]. The contribution of BM-derived cells to the generation of hepatocytes remains uncertain; the number of hepatocytes produced by this route is very low, and cell fusion may be an important mechanism [11,70]. BM cells are perhaps more important as a source of nonparenchymal cells such as Kupffer cells and endothelial cells as reported by Ng et al. [71] (the vast majority of recipient-derived cells present in transplanted livers were macrophages or Kupffer cells). On the other hand, in end-stage chronic liver disease, liver architecture is extensively disrupted because the parenchyma is replaced by fibrosis with poor blood supply. In this context, engraftment and differentiation of transplanted cells is a major challenge.
Thus, liver SC therapy has been guided by the most recent findings of human liver physiology and pathology, and several SC types have been used in preclinical and clinical studies as will be discussed later.
Surgical complications
The following surgical complications may be amenable to SC therapy.
Sepsis of abdominal origin
This process remains an important cause of death. Frequently, the initial damage is perpetuated by immunological mechanisms even when the source of infection is under control. The property of SCs that might be most important in this field would be their immunomodulatory function.
Anastomotic dehiscences
Many surgical procedures of the digestive tract (colonic, esophageal, etc.) are associated with high morbidity and mortality due to anastomotic complications, resulting from technical problems, poor vascularization, infection, or local inflammation. The immunomodulatory and angiogenic properties of SCs might help reduce the incidence of these complications.
Peritoneal adherences
These are the main causes of intestinal obstruction in individuals from developed countries and a frequent cause of infertility and abdominal-pelvic pain. Pathological inflammatory mechanisms often play a fundamental part in their origin by generating an imbalance between fibrinolysis and fibrinogenesis leading to excessive fibrin deposits. The immunomodulatory properties of SCs may therefore be beneficial.
Clinical and Preclinical Experience in Cell Therapy for Digestive Diseases
Currently, SCs are considered drugs and, as such, are subject to strict regulations. The European regulatory agencies consider SCs as Advanced Therapy Medicinal Products (EU Directive no. 1394/2007). In the United States, SCs are classed as a Human Cell, Tissue, and Cellular and Tissue–based product regulated by The Center for Biologics Evaluation and Research. SC therapy therefore has to undergo clinical development as would any drug. The clinical development program includes preclinical studies, quality controls, manufacturing recommendations, and carefully designed and controlled clinical trials. After the preliminary results in animals showing potential benefits, autologous application has been offered to single patients with some diseases in special conditions, even before some important issues (such as the exact mechanisms of action) have been fully clarified. Consequently, the field of SC therapy for digestive tract diseases developed in parallel at an experimental and clinical level. Nevertheless, most studies to date have been in animal models and, as of May 2010, few approaches have been tested in controlled clinical trials. We will now briefly analyze some of the most relevant animal and clinical studies.
Animal Studies Published with Digestive Disease Application of SC Therapy
A schematic representation from the most noteworthy experimental studies in animal models is shown in Fig. 1.
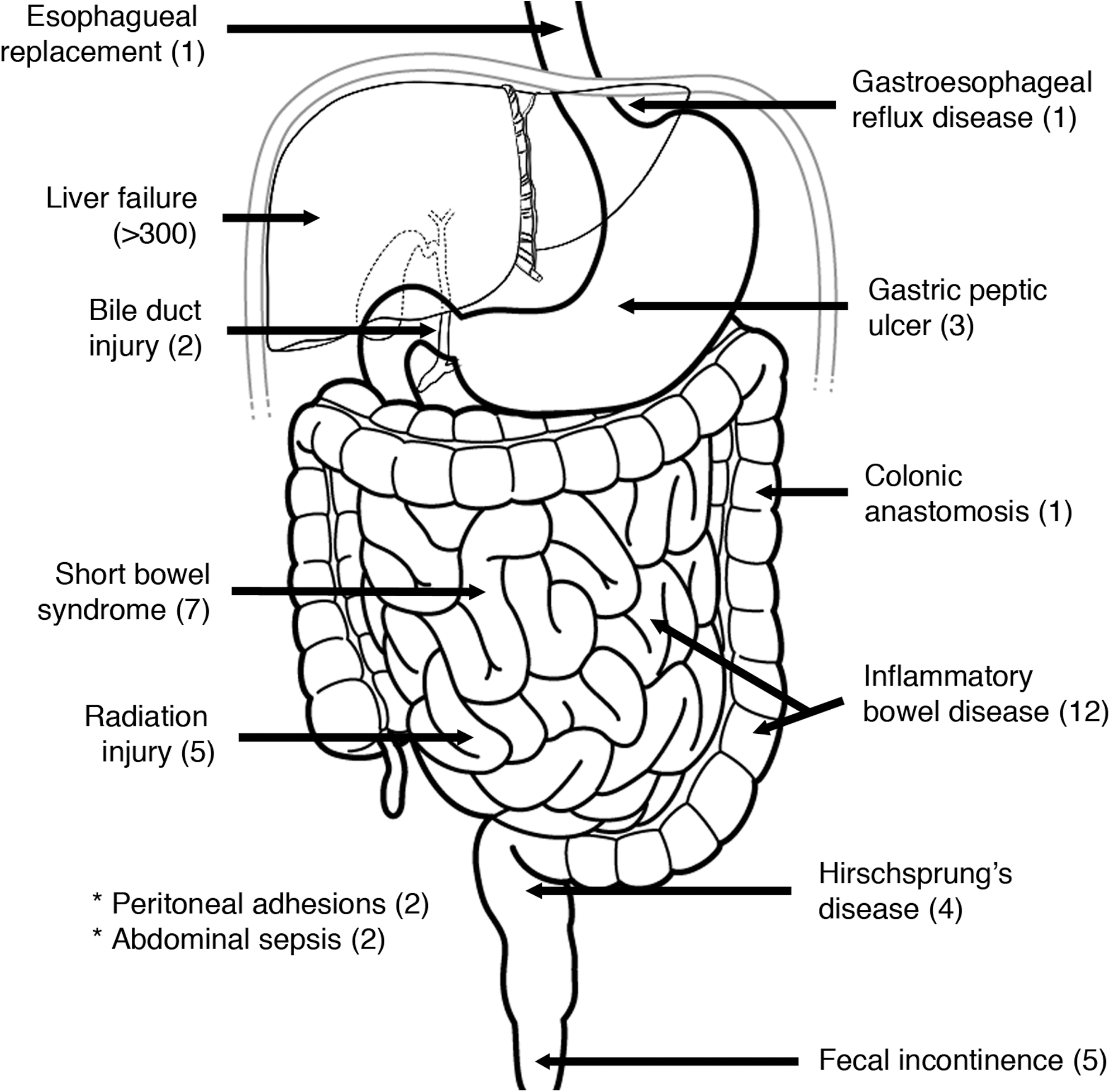
Schematic view of digestive tract diseases investigated in experimental (animal models) stem cell therapy. Approximate numbers of published articles by June 2010 are indicated in parentheses.
Esophagus and stomach
Esophageal replacement
Use of biomaterials composed of SCs seeded on new biopolymers has been studied as a replacement option, so far only in experimental models [72].
Gastroesophageal reflux
Preclinical studies using muscle and BM-MSCs [73] have sought to restore the lower esophageal sphincter in a minimally invasive process with good results. Nevertheless, recently published articles reveal that BMSCs could take part in esophageal adenocarcinoma formation and Barret's esophagus [74]. Clinical studies would therefore need to be conducted with caution in this field.
Gastric peptic ulcer
In animal models the use of BM-MSCs (administered by direct injection) has been studied, with faster healing observed, probably due to secretion of proangiogenic factors [vascular endothelial growth factor and hepatocyte growth factor (HGF)] [75,76].
Gastric ethanol-induced ulcers
One study examines the involvement of BM-derived cells in the regeneration of the stomach after gastric ulcers produced in rats with absolute ethanol. The authors concluded that those cells are involved in the regeneration of the stomach [77].
Liver
Cirrhosis is the liver disease for which most preclinical studies have been undertaken. Significant clinical–pathological improvements have been achieved after application of HSCs, BM-MSCs, ASCs, ESCs, and LPCs by systemic injection via the portal vein or the hepatic artery. Other processes tested include acute liver failure and metabolic disorders. Below, we discuss applications of different types of SC.
Use of LPCs [78]
We highlight the studies by Yasui et al. in which LPCs were transplanted into analbuminemic mutant rats; serum albumin level increased for up to 10 weeks [79]. Li et al. used LPCs predifferentiated in vitro; they were engrafted into mice with chronic liver injury induced with carbon tetrachloride. At 1 and 6 months after transplantation LPCs comprised 2% and 0.4%, respectively [80].
Use of HSCs [81]
The first reports on obtaining hepatocytes in vivo from HSCs were published in the late 1990s [11]. The effectiveness of this formation could range from 0.01% [82] to >10% [11] depending on the study and whether a selective growth advantage was present. Lagasse et al. [83] showed that HSCs could rescue mice from the lethal disease of hereditary tyrosinemia. An extensive literature review supports a paracrine effect or fusion as the mechanism of action [84], whereas other authors propose transdifferentiation [85].
Use of MSCs
Infusion of normal or preselected hepatocyte-like MSCs intrasplenically or intravenously into immunodeficient mice after liver damage with carbon tetrachloride rescued animals from hepatic failure and increased the extent of engraftment by >5% of recipient liver mass [86]. Use of previously differentiated MSCs in vitro with HGF improved liver function tests, mortality, and fibrosis [87]. In rats with D-galactosamine-induced liver injury, a 90% reduction in hepatocyte apoptotic events and an increase in the number of proliferating hepatocytes was seen only with MSC culture medium [88]. Several mechanism of action have been proposed, the extent of engraftment varies across studies, and there are also studies that did not find any beneficial effect on liver function or fibrotic scores [89].
Use of ESCs
The vast majority of authors have used ESC-derived hepatocytes with improvement in liver function or survival in different models of animal liver failure [90] or in models of bioartificial liver [91]. The percentage of engrafted donor cells ranged from 3% to 30% and the formation of teratomas has been reported in different studies [92,93]. In the study by Basma et al. [93] an unstable cell state or immunological rejection was proposed because after cessation of the toxin that produced liver failure the originally engrafted and proliferated cells were almost completely lost. The problem with ESCs is that very few differentiated cells are usually identified and that cellular heterogeneity is high. Several groups are therefore working on differentiation protocols and improvements in culture media. Efficient hepatic differentiation protocols have also been reported for human ESCs [93,94].
Use of fetal liver progenitor cells (hepatoblasts)
These cells are thought to be highly proliferative, less immunogenic, and more resistant to cryopreservation and ischemic injury. These cells are defined by their capacity to generate hepatocytes and cholangiocytes in vitro and after transplantation in vivo. Their purification has been difficult as fetal liver is also the temporary site of hematopoiesis, but these cells are capable to repopulate normal rodent adult liver [95].
Bile ducts
Limited SC research has been done in this field. One study, in a canine model, applied multipotent cells from the amniotic membrane, to repair lateral lesions and sections of the common bile duct with no evidence of stenosis [96]. Lin et al. [97] proposed the use of BMSCs for treatment of bile leak after hepatobiliary surgery, but so far this has not been tried in any experimental model.
Small intestine
Full-thickness regeneration has been the final goal of several studies. With techniques of tissue engineering, investigators have managed to produce autologous small intestine using small samples of intestinal tissue containing SCs (organoids) [98 –100] or working in the identification and purification of SC populations located in the bowel [101]. A good review of this topic was published by Gupta et al. [102]. Hori et al. [103] achieved small intestine regeneration by MSC seeding on collagen sponge graft in dogs, although the newly formed intestine lacked muscle layer. Nakase et al. [104] approached this drawback by seeding the graft with smooth muscle cells. Successful regeneration was also shown in an animal model of intestinal excision and repair using an MSC-enriched collagen-agarose 3-dimensional patch on a human or swine aortic fragment [105]. Although this is a promising approach, further studies are needed before it is used in clinical practice.
Major progress has been made in the field of epithelial regeneration after radiation injury. There are some interesting studies on this topic; Semont et al. [106] reported that infused BM-MSCs could be engrafted into irradiated intestine and contribute to its regeneration. Okamoto et al. [107] reported that BM-derived cells could promote the regeneration of damaged epithelia in human intestinal tract and that BM-derived epithelial cells significantly increased in number. The location rate of BMSCs in the intestinal mucosa is generally low, ranging from 0.17% to 2.7% [106,108]. Zhang et al. [109] analyzed MSCs modified by CXCR4 (the receptor for SDF-1); the extent of engraftment into irradiated intestine was significantly increased, and intestinal permeability and histopathological damage was ameliorated.
Large intestine
Attempts to regenerate the enteric nervous system in Hirschsprungs' disease of the colon by neural progenitor cell transplantation have been made. It was found that enteric nervous progenitors are present in the embryonic and adult gut [110]; as the disease affects only one colon segment, autologous use is possible. Scientists have isolated and cultured those progenitors to obtain neurospheres. Transplanted into aganglionic bowel, the progenitor cells migrated, differentiated, and restored the normal contraction rate [111]. This treatment has not yet been applied in humans.
We wish to highlight some studies of fecal incontinence, which is of great social relevance given its high incidence. There are studies with BM-MSCs (murine model) for surgical damage and surgical repair [112], with muscle SCs for cryolesion in rats [113], with predifferentiated muscle SCs (myoblast) transplanted to mice after surgical damage (this study concluded that myoblasts were most efficiently obtained from juvenile rats) [114] and with human umbilical cord matrix and BM-MSCs from rabbit in rabbits [115]. Our group is working with animal models of this condition with ASCs.
Surgical complications
Anastomotic dehiscences
Anastomotic leak is one of the major complications during the early postoperative period after colorectal surgery, with high morbidity and mortally rates. In the Stem Cell Therapy Laboratory of “La Paz” Hospital, we investigated whether ASCs might help reduce the incidence of anastomotic dehiscences in colorectal surgery. We wrapped surgical sutures in ASCs so that, on passing the suture through the tissue, the ASCs were deposited at the critical point to reinforce the anastomosis. These are denoted as “biosutures” or “stem-cell-coated sutures”.
The animal model used was colic anastomosis with free stitches in rats. It was observed that the sutures became coated in cells within 24 h of culture and that they could be used in the same way as conventional sutures. There were no differences between the 2 groups (biosutures vs. conventional sutures) in the incidence of dehiscence, dilation, obstruction, histological inflammatory pattern, and rupture pressure; the frequency of adherences was significantly lower in the biosuture group at 4 and 7 days but not later, while anastomotic resistance was maintained [116].
Sepsis of abdominal origin
In a recent study, BM-MSCs were applied intravenously in an animal model of abdominal sepsis before and just after its induction [117]. A decrease in mortality of up to 50% and an improvement in organic functions were seen. Similar results were achieved with ASCs [118].
Peritoneal adherences
In view of the immunomodulatory properties of some SC types, several studies with animal models have been undertaken to assess whether SCs can be used to prevent the formation of peritoneal adhesion [119,120]. Our group is also working in this line of research.
Crohn's disease
Several studies have been performed in experimental models. Of note, for example, are three murine models, one of which uses murine and human ASCs [121], another applies BM-HSCs topically [122], and another compares HSCs and MSCs [123]. In nearly all these studies, an improvement can be seen. How the improvement occurs is still unknown; investigators have focused on the regenerative, trophic [124], and immunoregulatory [125] potential of SCs. More studies are, however, necessary to confirm the efficacy and identify possible indications. Two good reviews on this topic are provided by Dryden et al. [126] and by Lanzoni et al. [127].
Ongoing and Published Clinical Trials with SCs in Digestive Disease
In the last 3 years, there has been a 15-fold increase in the number of clinical trials with SCs, whereas in the last 5, the number of trials for digestive diseases has increased 10-fold. In May 2010, in the
The disease, type of SCs used, and phase of development of the trial are indicated.
Liver failure, Crohn's disease, and perianal fistulas are the three main digestive diseases for which SC therapy is being tested. SC applications in most of these indications are currently under clinical development. A schematic representation from the main ongoing or completed clinical trials is shown in Fig. 2.
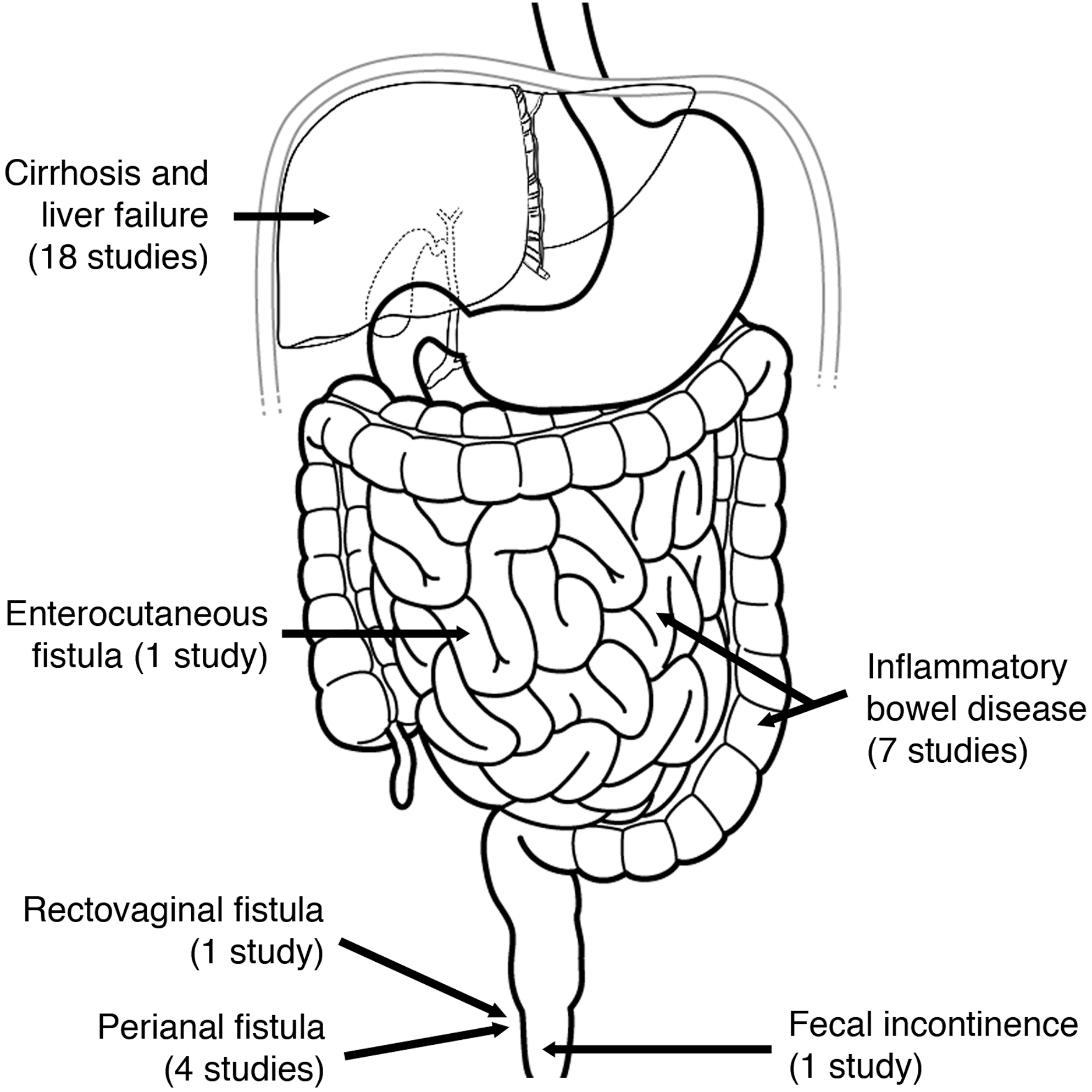
Schematic view of digestive tract diseases under investigation in ongoing stem cell therapy clinical trials registered at
Below, we highlight some of the most noteworthy aspects of the clinical trials already published and those that are ongoing.
Liver failure
The results of almost 20 trials and several case series can be found in the literature. We discuss some of these published trials below.
No clinical trials have been completed using LPCs or ESCs.
The simplest studies only mobilize cells from BM with granulocyte colony-stimulating factor (G-CSF) infusion; for example, in the trial from Gaia et al. [128] mobilized cells were applied to 8 patients and clinical and biological improvement was observed [Child-Pugh and Model for End-stage Liver Disease (MELD) scores] without adverse events. There are some methodological weaknesses with this trial: the short duration, the lack of a control group, and the lack of knowledge about which SCs were responsible of the clinical improvement.
In a more complex approach, BM cells are mobilized and collected (with or without ex vivo manipulation). Of note is a phase I study with 5 patients who were administered CD34+ HSCs (3 via the portal vein and 2 via the hepatic artery) obtained by leukapheresis after mobilization with G-CSF without encountering any adverse effects [129]; after follow-up of 60 days, bilirubin improved in 3 of 5 patients and albumin in 4 of 5; ascites even resolved in 1 of these patients. A subsequent publication documented the long-term outcomes after 12 months. It is encouraging that all patients were still alive with improved biochemistry (reduction in serum bilirubin levels and albumin levels increase) [130].
Other trials have used cells obtained from BM with or without ex vivo selection or manipulation: The first randomized controlled trial in this area used unselected cells. Patients were randomized to receive autologous BM cell therapy (mononuclear cell preparations infused into hepatic artery, 15 patients) or placebo (15 patients) in a unblinded fashion. Follow-up lasted 12 months. The authors found a partial improvement in liver function, primarily in the first 3 months after BMC therapy. Beyond this period, liver function seemed to return to baseline levels. That improvement was quantified using the Child-Pugh score (14% group difference after 30 days, P = 0.017), albumin levels (significant increase, particularly in the first 90 days with an increase of 16% compared with baseline, P = 0.034, although this difference had diminished at 12 months), total bilirubin (stabilized during the first 90 days after BMC therapy but increased in controls; bilirrubin increase significantly during all the follow-up in the control group [P = 0.011], whereas it remained unchanged in the treated patients) and MELD score (significantly increased after 12 months in the control group but stable in the treated patients with a maximum group difference of 14% at 60 days, although this difference was not significant). There was no correlation between the total number of cells infused or the number of CD34+ or CD45+ cells and albumin levels. The authors did not detect any major side effects; 1 patient developed third-degree atrioventricular block, but in authors' opinion this event was not related to BMC infusion [131]. These results are the first to support a significant benefit from SC therapy in this area. Given that the major effect was detected in the Child-Pugh score (which is very subjective in some of its items), we think that more studies with more robust outcome measures are needed. In a phase I study, autologous HSCs (CD34+) were infused into the hepatic artery, but the study had to be terminated due to severe contrast-related nephrotoxicity [132]. After 6 months of follow-up, 1 patient had improved albumin, whereas another had improved prothrombin (with deterioration in bilirubin, creatinine, and MELD score), and a third had improved albumin, prothrombin, and MELD score. The authors concluded that this route of administration might not be safe. In another phase I study, autologous expanded BM-MSCs were infused via a peripheral vein [133]. After 12 months of follow-up, no adverse events had been reported and it was observed that 2 patients improved their liver function and MELD score during the entire follow-up, one improved initially before returning to baseline values and other showed no changes; all showed improvements in quality of life. A phase I–II study [134] infused autologous expanded and predifferentiated to hepatocytes (with HGF, dexamethasone, and oncostatin M) BM-MSCs to 8 patients (6 via the portal vein and 2 via a peripheral vein) with a follow-up of 3 months. There were no adverse effects and MELD, prothrombin international normalized ratio, and creatinine improved significantly; albumin and bilirubin also improved, but not significantly.
A related application is increase liver mass before major liver resection in patients with large tumors. A German group attempted to compare the effectiveness of portal vein embolization (PVE) and CD133+ BM SC administration to the remnant liver (via portal vein, before PVE), compared with PVE alone. Six patients with a future liver remnant volume below 25% underwent BMSC administration (group I) and 7 patients received only PVE (group II). They concluded that the combination of PVE with CD133(+) BMSC administration significantly increased hepatic regeneration compared with PVE alone [135].
This indication currently has the largest number of ongoing trials, all in phase I and II. All of them are using autologous cells (Table 2). In some, the BM-MSCs are predifferentiated to hepatocyte progenitors in vitro (clinicaltrials.gov identifier NCT00420134) and some have a control group (identifier NCT00976287). Although not strictly concerning liver failure, as an exception, allogeneic BM-MSCs are being used for treatment of homozygous familial hypercholesterolemia (clinicaltrials.gov identifier NCT00515307).
Critical analysis
The majority of the published clinical trials show some improvement in clinical or laboratory scores and provide safety data. There are some methodological concerns such as the small number of patients in each study, the variation in cell products and application routes, the lack of a control group in most studies, the limited information provided about additional therapies received by these patients, and the mixed causes of chronic liver disease. In studies concerning MSCs, it is important to consider whether the authors fulfil the three minimal criteria established to define exactly which cells isolated from human BM and other mesenchymal tissues are MSCs [21]; further standardization of the most appropriate methods of isolation and expansion of these cells is needed.
Although cell therapy for chronic liver disease may soon become clinically viable, there are some important issues, essentially concerning safety, that need special attention: The best evidence for engraftment and generation of functional liver parenchyma has actually been obtained for mature adult hepatocyte transplantation. More than 100 patients with innate metabolic failures or with postresection liver failure (as a definitive treatment) and also with fulminant liver failure or chronic liver failure with acute decompensation (as a bridge to liver transplantation) have received such therapy [136,137]. The results have been promising. The major limiting factors are the quality (frequently cells are derived from grafts deemed unsuitable for transplantation), engraftment, survival (results tend to ameliorate 3–6 months postinfusion), and function of transplanted hepatocytes. Thus, much effort is required to perfect the in vitro differentiation protocols of progenitors/SCs to functional hepatocytes before transplantation. As mentioned above, there are 2 main proposed mechanisms of generating functional hepatocytes from transplanted cells: cell fusion [14] and transdifferentiation [12], with more data pointing to the first mechanism. Fusion also creates questions with regard to safety because it induces phenomena like aneuploidy related to tumor formation. Nevertheless, the efficacy of both mechanisms in generating functional liver tissue when transplanting nondifferentiated SCs or even predifferentiated hepatocyte-like cells is very small [13,138,139]. Further, special consideration should be given to the unresolved issue of SC carcinogenesis. Several studies have suggested that poorly differentiated hepatocellular carcinoma originates from hepatic oval cells and BMSCs or at least that progenitor cells participate in the process [68,69], and there are also some reports of malignant transformation of MSCs after prolonged in vitro culture [140]. Another interesting study relates SC fusion with an altered premalignant cell and aneuploidy with carcinogenesis [141]. However, more studies are needed to clearly define this potential causal relationship. Certain subtypes of SCs might even contribute to liver fibrosis. There is also growing evidence of the role of SCs in the fibrogenic process [142], Russo et al. [143] found that the contribution of BM to parenchymal regeneration was minor (0.6%) and the BM contributed significantly to hepatic stellate cells (68%) and myofibroblasts (70%) in a mouse model of cirrhotic liver. These BM-derived cells did not arise through cell fusion. The authors suggested that care should be taken in those clinical trials applying BMSCs in liver cirrhosis because they seem an important promoter of the fibrosis processes and thus can worsen the disease.
In conclusion, we believe that more animal data on safety, which types of SCs to use, the best dosage, the most efficient application route, and therapeutic mechanisms involved are urgently required. Large randomized controlled clinical trials are necessary before firm conclusions can be drawn on the benefit of SC in chronic liver disease. Nowadays, SC application should be considered only under in the strictly regulated clinical trial setting while awaiting for the results of ongoing trials.
Crohn's disease
The most noteworthy advances have probably been achieved with this disease. The presumed mechanism of action of the cells has been commented previously. In the clinical setting, the two most important ones are the capacity to reset the native immune system by HSC transplantation and the inmunomodulatory properties of MSCs. In the case of HSCs, the preconditioning regimens could eliminate T-cell reservoirs and after HSC transplantation, de-novo hematopoiesis would generate naive cells. HSC allotransplanted patients probably experience a graft-versus-autoreactive response and the immune system gets almost completely replaced [127].
First, we are going to analyze the published studies: with regard to luminal disease, preliminary support for this application came from retrospective analyses of hematological transplantations. Thus, for example, in a case series, remission was observed in 4 out of 5 patients with Crohn's disease and leukemia after allogeneic BM transplantation [144] (mean follow-up 4.5–15.3 years; these 4 patients had not received immunosuppressants for at least 6 months) and in another case series [145], remission of symptoms occurred in all patients (6 with Crohn's disease and 4 with ulcerative colitis) after myeloablative treatment and allogeneic BM transplantation (follow-up 3–117 months; one patient had a mild self-limiting recurrence and another died of infectious complications; all patients except 2 maintained immunosuppressive therapy at the end of follow-up).
Based on these results, trials began with HSCs as the primary treatment of the disease; of note was a phase I study by Oyama et al. [146] with infusion of autologous HSCs from peripheral blood, after mobilization, expansion, and conditioning in 12 patients with refractory Crohn's disease. After 6 months, 11 had remission [Crohn's Disease Activity Index (CDAI) <150], and after 18.5 months of follow-up only 1 patient had experienced recurrence. Another trial successfully used peripheral HSCs unselected for CD34 in 4 patients (mean follow-up, 16.5 months) [147].
Subsequently, the interest in using MSCs began to grow. Most trials are ongoing although some have started to report results. For example, 1 trial applied expanded autologous BM-MSCs intravenously and recorded an improvement in CDAI in 4 out of 6 patients (mean decrease from 334 to 226 in 6 weeks) [148]. Onken et al. carried out a phase II trial with expanded allogeneic MSCs (Prochymal™), which were administered in 2 doses 7 days apart in patients with moderate–severe refractory Crohn's disease (CDAI >220). The investigators observed a statistically significant decrease in mean CDAI after 28 days (from 341 to 236) with a mean decrease of 62 points in 7 days; all patients improved their CDAI, and clinical remission was achieved in 3 of 9 patients (inflammatory bowel disease questionnaire [IBDQ] <170) [149] without any noteworthy adverse events. In a 12-month study of 8 patients, 7 adverse events with an unlikely causal relationship with the MSC procedure were reported [150]. No tumors or formations of ectopic tissue were found.
There are currently 3 ongoing phase III trials, two with allogeneic BM-MSCs (NCT00482092 and NCT00543374) and one with autologous HSCs (NCT00297193). The first two are being conducted by Onken et al. and are double-blind, controlled, and multicenter trials: the first one seeks to assess relapses, clinical improvements, or improvements in quality of life, and the second one contemplates reinfusion if an effect occurs and studying its duration. Both were stopped in March 2009 because an interim analysis showed an excessive response in the placebo group as reported by Osiris Therapeutics Inc. in a press release. This is commented in a report in Nature Biotechnology [151]. The press release clarifies that stopping recruitment was not due to any safety concerns. In another recent press release (May 5, 2010), Osiris Therapeutics Inc. announced that enrolment in this clinical trial had resumed, but only to the placebo and best-performing Prochymal dose arm, according to the prespecified trial design [152]. In trial NCT00297193, HSCs are first mobilized, then myeloablation is done, and finally the cells are supplied at 4 or 59 weeks (to determine whether the effects are due solely to mobilization agents).
Critical analysis
We can find similar methodological concerns to those discussed in the studies that have been published on liver disease: the small number of patients, the variation in cell products, and lack of published controlled studies. It is also striking that the two allogeneic studies needed to be stopped due to methodological concerns. We therefore believe that more animal studies are required and that large randomized controlled clinical trials are necessary to obtain firm conclusions.
Fistulizing disease
The only fully surgical indication in clinical development is complex perianal fistulizing disease (including rectovaginal fistulas). The use of autologous ASCs is the most widely studied.
First, we are going to analyze published studies: in 2002, the first intralesional inoculation of autologous ASCs was done to try to seal a recurrent and refractory rectovaginal fistula in a patient with Crohn's disease [153]. The fistula is currently closed.
Two clinical trials have been reported: the phase I study was a prospective, single-center, uncontrolled, open-label study. Five patients with Crohn's disease were included [154]. These patients had 8 complex fistulas (enterocutaneous, rectovaginal, or perianal) refractory to medical-surgical treatment. ASCs resuspended in ringer lactate or fibrin glue (Tissucol® Duo; Baxter) were applied. After follow-up of 12–30 months, treatment was successful in 6 fistulas. The most important result was the demonstration that the procedure was feasible and safe (no adverse effects or tumors appeared) [155]. The phase II study was an open-label, randomized, multicenter study. Fifty patients with complex perianal fistulizing disease were included, 14 with and 35 without Crohn's disease. Autologous ASCs were compared to fibrin glue. Fistula closure was observed in 17 of 24 in the ASC group (71%, 46% after the first and 25% after the second dose) compared to 4 of 25 (16%, 8%, and 8%, respectively) with the relative risk of cure being 4.43 (1.74–11.27; P < 0.001). These results were similar regardless of whether the patients had Crohn's disease or not. After 1 year, 17.6% of the patients in the experimental group had experienced recurrence. Both treatments were well tolerated with no adverse events related to ASC therapy. Therefore, ASCs combined with fibrin glue were considered effective and safe. This procedure probably helps to conserve (or maybe improve) anal continence as the fistulous tract is not resected [156].
Other studies along similar lines have been published: there is a study comparing intralesional application of SVF cells with expanded ASCs in enterocutaneous fistulas in patients with Crohn's disease. SVF was applied to 4 patients (1 cure after 8 weeks) and this was compared with the outcomes of 4 fistulas in the phase I study (3 cures after 8 weeks) [157]. SVF cells with fibrin glue have been also tested for occluding a tracheomediastinic fistula; this study showed closure of the orifice after 3 months and strong neovascularization (maintained at 1 year) and disappearance of the mediastinal cavity without neoplastic cells apparition in bronchoalveolar lavage or adverse effects related to treatment [158].
In addition, there are four ongoing trials from this same group; the phase III trial with perianal fistulas (to extend the studies of efficacy and adverse events), subdivided into patients without inflammatory bowel disease (FATT I, clinicaltrials.gov identifier NCT00475410) and those with Crohn's disease (FATT II). Both are prospective, multicenter, randomized, active-controlled, single-blind studies. The FATT I trial compares administration of autologous ASCs and fibrin glue with instillation of fibrin glue only and recruitment is finished. Although the data are not yet published and are under revision, the trial was complicated by the unexpected finding that the clinical outcomes of patients in control group were better than anticipated, making it harder to show the effectiveness of autologous ASCs. After the first case of successful treatment of Crohn's disease-associated rectovaginal fistula using allogeneic ASCs [159], a phase I–IIa study on feasibility and safety of the use of allogeneic ASCs in rectovaginal fistulas (ALOREVA, clinicaltrials.gov identifier NCT00999115) was started. Finally, another study has been recently approved for tracheo-esophageal fistulas.
Critical analysis
The most substantial limitations are the small number of patients and the need for long-term follow-up of patients in these randomized controlled clinical trials. BM mononucleated cells or SVF therapies use cells without MSCs selection or expansion in vitro, and represent different strategies of cellular therapy because they contain a heterogeneous mixture of inflammatory cells and cytokines in addition to a modest population of SCs. It is important to take into account that several phase III studies with MSCs (for the treatment of graft vs. host disease, Crohn's disease and perianal fistula) have encountered methodological difficulties (eg, patients receiving control treatment performed better than anticipated) even though phase I/II studies had shown beneficial effects.
Fecal incontinence
The debilitating nature of this condition has stimulated an intensive search for new treatment options. Based on growing knowledge and promising results of the above-mentioned preclinical studies, a clinical trial focusing on safety was recently initiated for autologous ASCs applied to the anal sphincter (clinicaltrials.gov identifier NCT01011686).
An observational pilot study has also been published in which anal incontinence due to obstetric external anal sphincter disruption was treated by injection of autologous myoblast cells directly into the external anal sphincter in 10 women refractory to conventional nonsurgical therapy. The authors concluded that the injection was safe, well tolerated, and significantly improves symptoms of anal incontinence [160].
Celiac disease
One study has tested high-dose chemotherapy followed by autologous HSCs infusion in one kind of celiac disease that is unresponsive to available therapies and that carries a high risk of enteropathy-associated T-cell lymphoma. The authors concluded that the treatment is feasible and safe and might result in long-term improvement. They treated 7 patients and found a significant reduction in the number of aberrant T cells in duodenal biopsies associated with improvement in clinical and biochemical markers without major nonhematologic toxicity or related mortality [161].
Diabetes mellitus
Although this disease is not usually treated surgically, it deserves special mention. In recent years, several phase I and II trials have studied the possibility of restoring pancreatic endocrine function with SCs, mainly autologous HSCs and BM-MSCs (NCT00644241, NCT00807651, and NCT00971503).
Future Perspectives
Over the last decade, cell therapy with SCs for nonhematological diseases has grown exponentially. Experimental studies have generated sufficient knowledge to allow the jump to clinical research in the context of clinical trials and compassionate use.
Recognition of SCs as a therapeutic agent and the legislation developed in several countries regulating their use will ensure that they will probably arrive to the market (provided the phase III studies confirm the promising results shown to date) in a safe and properly controlled way. Nevertheless, there are several main problems still to be resolved and these are hindering more extensive SC application. More animal data on safety, what SCs to use, the best dosage, the most efficient application route, and therapeutic mechanisms involved are urgently required. SC isolation must be standardized between different laboratories and properly defined to produce a consistent product according to Good Manufacturing Practice. With regard to safety, the interaction between cancer and SCs, despite the numerous preclinical studies carried out so far, remains controversial and must be resolved. SC migration toward neoplastic foci is feared to induce cancer progression, although some progress has been made using this feature for local delivery of chemotherapy drugs to the cancer site, thereby reducing systemic toxicity. Currently, existing neoplastic disease is considered a major contraindication for cell therapy in the context of most ongoing clinical trials. As soon as this issue is resolved, the number of possible applications would probably increase.
In the field of digestive tract diseases, several phase I–II clinical trials have been reported and there are currently numerous ongoing phase II–III trials, mainly in liver disease and inflammatory bowel disease, that may soon reveal the real benefit (or not) of the SC application. Nevertheless, large randomized controlled clinical trials are necessary before firm conclusions can be drawn. If current trends persist, the number of digestive diseases treated with SC will increase exponentially in the next decade.
Up until now, autologous transplantation has been the preferred to avoid the immune rejection and ethical problems. However, this can delay the SC procedure due to the time needed to sample and purify the cells and certain patients, with emergency conditions, may be excluded. The new insights in this field uncover the theoretical possibility for allogeneic use of mesenchymal SCs, based on the immune tolerance they induce. Thus, an increasing number of studies are being performed with allogeneic cells. If similar results were obtained, SC banks could be created.
On the other hand, simplification of cell expansion with closed systems, currently under development, will help make these therapies more accessible and less costly. The creation of international SC banks could facilitate access for developing countries.
Basic research continues in its endeavors to obtain certain types of cells that are able to integrate into and function within the organ, thereby participating in the complex homeostasis of an organism. If this could be achieved, the jump from reparative to regenerative therapy could be made. Today, this may seem like science fiction, but the results obtained today would also have seemed so a few years ago.
Footnotes
Acknowledgments
The authors of this article would like to express their gratitude to the following: Dr. Greg Morley for his invaluable linguistic corrections and Dr. Irene Sanz Gallego and Dr. Paula Barba Recreo for their continuous support during drafting of this review.
Author Disclosure Statement
No competing financial interests exist for any of authors of this review with any commercial entity that has a known interest in the subject of this article.