
Abstract
Retinal degeneration is a devastating complication of diabetes and other disorders. Stem cell therapy for retinal degeneration has shown encouraging results but functional regeneration has not been yet achieved. Our study was undertaken to evaluate the localization of stem cells delivered to the retina by intravenous versus intravitreal infusion, because stem cell localization is a key factor in ultimate in vivo function. We used lineage-negative bone marrow–derived stem cells in a model wherein retina of mice was induced by precise and reproducible laser injury. Lin-ve bone marrow cells (BMCs) were labeled with a tracking dye and their homing capacity was analyzed at time points after infusion. We found that Lin-ve BMCs get incorporated into laser-injured retina when transplanted through either the intravitreal or intravenous route. The intravenous route resulted in optimal localization of donor cells at the site of injury. These cells incorporated into injured retina in a dose-dependent manner. The data presented in this study reflect the importance of dose and route for stem cell-based treatment designed to result in retinal regeneration.
Introduction
T
The present study was designed with the objective of investigating the recruitment of Lin-ve bone marrow cells (BMCs) at the site of laser injury in retina when delivered through intravenous and intravitreal routes at varying doses and time points.
Materials and Methods
Animals
All the experiments in this study were performed according to the Institutional Animal Ethics Committee Guidelines. Animals used in this study were 6–8-week-old C57BL/6J female mice and efforts were made to minimize the number of animals and suffering. Animals were maintained in a 12-h light/dark cycle (LD 12:12) and fed on chow diet with free access to drinking water.
Study design
Animals were broadly divided into 3 groups—Group 1: intravitreal transplantation; Group 2: intravenous transplantation; and Group 3: laser injury control. In Group 1, Lin-ve BMCs were transplanted through intravitreal route in mice with laser-injured retina at 3 different doses (50,000, 100,000, and 200,000 cells; n=6 eyes for each dose) and all animals were sacrificed after 4, 11, and 21 days of cell transplantation. In Group 2, Lin-ve BMCs were intravenously transplanted (100,000 cells through tail vein route) in mice with laser-injured retina. The animals were sacrificed at 4, 11, and 21 days (n=6 for each time period). To study the role of injury in donor cell incorporation, 100,000 Lin-ve BMCs were intravenously transplanted in mice with or without laser injury (Group 3, n=6). The uninjured contra lateral eye served as control for laser injury.
Establishment of laser injury model of mouse retina
Argon green laser (532 nm; Iris Medical) was used to induce injury in retina. Briefly, mice were anesthetized with a cocktail of xylazine (10 mg/kg) and ketamine (100 mg/kg) and placed in front of a laser photocoagulator. Pupils were dilated with tropicamide (1% solution), and lignocaine (2% solution) was applied as local anesthetic to the eyes. Laser was imparted to the retina to produce 8 spots around the optic nerve in circular fashion, 2 each in a quadrant, maintaining a distance of 2 disc diameter from optic disc and employing 200 mW and 532 nm with a pulse of 100 ms, generating 100 μm spots.
Fluorescein angiography and fundus photography
Fluorescein angiography was performed after laser injury to visualize the laser spots on 7th day. Fluorescein dye leakage was observed at the sites of laser damage and images of laser injury spots were captured with a fundus camera.
Tissue sectioning
Mice were sacrificed with an overdose of anesthesia (ketamine–xylazine cocktail). The eyeballs were enucleated and either processed fresh or fixed with 4% p-formaldehyde solution overnight at 4°C. For sectioning, eyeballs were embedded in optimal cutting temperature compound (OCT) medium (Jung, Leica Microsystems) and 6-μm sections were obtained with a cryostat (CM 1510 S cryostat; Leica). The sections were laid on poly-
Histopathological analysis of laser-injured retina
Cryosections were stained with hematoxylin and eosin and examined under a microscope to study the morphological changes as a result of laser injury in the retina.
Immunohistochemistry
Immunostaining of rhodopsin was also performed to examine the laser-induced damage to photoreceptors. The sections were incubated with 5% goat serum for 1 h at room temperature followed by incubation with primary antibody (anti-mouse rhodopsin, 1:100; Santacruz) for overnight at 4°C in a humidified chamber. The next day, sections were washed 3 times with phosphate buffered saline tween-20 (PBST) buffer [0.01 M phosphate-buffered saline (PBS), 1% bovine serum albumin (BSA), and 0.05% Tween20] followed by incubation with secondary antibody for 2 h at room temperature (fluorescein isothiocyanate–labeled goat anti-rabbit IgG; Jacksons Immunoresearch). The sections were mounted with antifade mounting medium (FluorSave Reagent; Calbiochem), coverslipped, and examined under a fluorescence microscope (Leica DM-1000).
Isolation and enrichment of BMCs
Mouse femurs and tibias were flushed with culture medium (Invitrogen) to obtain BMCs. BMCs were depleted of RBCs using RBC lysis buffer (Gey's solution). Cells were then incubated with primary antibody (biotin-conjugated lineage antibody cocktail) (anti-CD45, CD5, TER-119, CD11b, and GR-1) for 10 min at 4°C followed by incubation with streptavidin-conjugated magnetic beads for 15 min at 4°C (Lineage Depletion Kit for mouse; Miltenyi Biotech). Unbound antibodies were washed away from cells with MACS buffer [PBS (pH 7.2) and 0.5% BSA]. The magnetic cell sorting (MACS) column was placed in the magnetic field of QuadroMACS separator and rinsed with 0.5 mL MACS buffer before loading cells. Cells were loaded into MACS column (MS column; Miltenyi Biotech) and allowed to pass through the column and the effluent was collected as a fraction enriched with Lin-ve cells. The cell number for transplantation was adjusted with a hemocytometer. The method used was the same as recommended by the commercial kit and as used by previous studies [19,20].
CFDA-SE labeling of BMCs
Carboxyfluorescein diacetate succinimydal ester (CFDA-SE) (Vybrant CFDA cell tracer kit; Invitrogen) was used to track the recruitment of transplanted cells in laser-injured retina. Briefly, 2 mL of CFDA-SE solution (5–10 μM) was added to 2 mL cell suspension and incubated for 15 min at 37°C with dye. After 2 washings, these were reincubated with PBS for 30 min at 37°C. The cell number was adjusted for transplantation.
Transplantation of Lin-ve BMCs
Intravitreal injection
About 2 μL of Lin-ve BMCs with 3 different doses (50,000, 100,000, and 200,000 cells; n=6 per dose group) were intravitreally injected using Hamilton syringes (Hamilton Company) immediately after laser injury. As a control, normal saline was injected into the contralateral eye of the same animal.
Intravenous injection
About 100,000 Lin-ve BMCs suspended in 100 μL PBS were injected with a 1-mL syringe fitted with a 27-gauge needle into the tail vein immediately after laser injury.
All transplantation procedures were carried out under anesthesia as per Institute of Animal Ethics Guidelines.
Quantitative analysis of donor cells in laser injury
CFDA-SE–labeled donor Lin-ve BMCs incorporated into laser injury were counted in both intravitreal and intravenous groups. Cell counts were performed on fluorescence images of cryosections of the laser-injured retina by a blinded observer. The whole eyes were serially sectioned for counting donor cells (n=6 eyes each for intravitreal and intravenous groups).
Results
Validation of laser injury by fluorescein angiography and fundus photography
Laser-injured mouse eyes were imaged with a fundus camera to score the leakage of fluorescein dye injected through the intraperitoneal route on 7th day after injury (Supplementary Fig. S1a, b; Supplementary Data are available online at
Rhodopsin immunolabeling
Rhodopsin is a transmembrane protein present in the outer segments of rods and serves as an excellent immunohistochemical marker for rod cells in mammalian retina. Immunostaining intensity and pattern of rhodopsin in laser-injured eyes of mice, in comparison to the control eyes, confirmed the disruption of photoreceptors in these animals. Laser injury led to disruption of photoreceptor outer segments, resulting in a typical kink, which was immunolocalized by application of rhodopsin antibody (Supplementary Fig. S1e, f). This disruption was lacking in mice eyes that were not laser injured and there was no immunolocalization of rhodopsin like the one seen in laser-injured mice.
Enrichment of Lin-ve BMCs
BMCs isolated from mouse femurs and tibias were enriched for Lin-ve cells by MACS. Lin-ve BMCs were stained with CFDA-SE and its incorporation was verified by fluorescence assisted cell sorting (FACS) analysis (Supplementary Fig. S2a, b).
CFDA-SE–labeled Lin-ve BMCs were injected in the vitreal space of laser-injured eyes at 3 different doses, that is, 50,000, 100,000, and 200,000 cells/animal, which were sacrificed 21 days later. Cryosectioning of eyes revealed the incorporation of donor CFDA-labeled cells in various layers of the host retina. Donor cells were observed in the photoreceptor layer (Fig. 1a, c) as well as in the ganglion cell layer (GCL) (Fig. 1b, d) of injured retina.
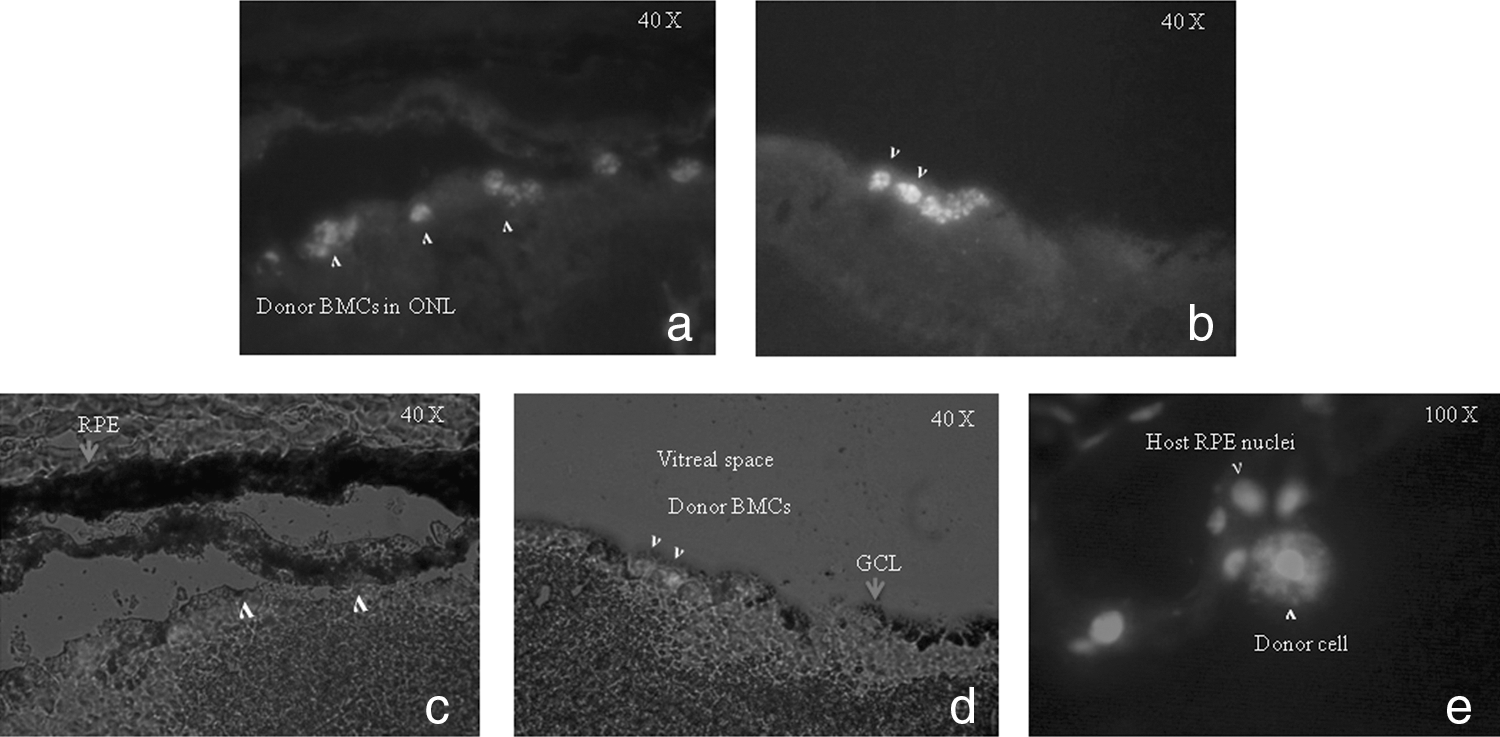
Incorporation of donor Lin-ve BMCs transplanted via intravitreal route in laser-injured retina. About 100,000 donor BMCs labeled with CFDA-SE (indicated by >) were intravitreaously transplanted in mice immediately after retinal laser injury. Cryosectioning of enucleated eyes at 21 days revealed incorporation of donor cells (indicated by arrows) in the photoreceptor layer
The effect of dose on the incorporation of donor cells was studied by transplanting different doses of donor cells in the vitreous of laser-injured retina. The donor cells were found to reach the injury site at all the doses used in this study. Donor cells were observed in the injured retina with a dose of 50,000 cells (Fig. 2a) and 100,000 cells (Fig. 2b). However, the highest dose of 200,000 cells resulted in clumping of cells in the vitreous (Fig. 2c) with relatively poor migration in the outer retina. We observed that donor cells in the 200,000 dose group remained in the vitreal space as long as 21 days posttransplantation. The total number of cells observed in the host retina as well as in individual layers was counted to compare the effectiveness of different doses.
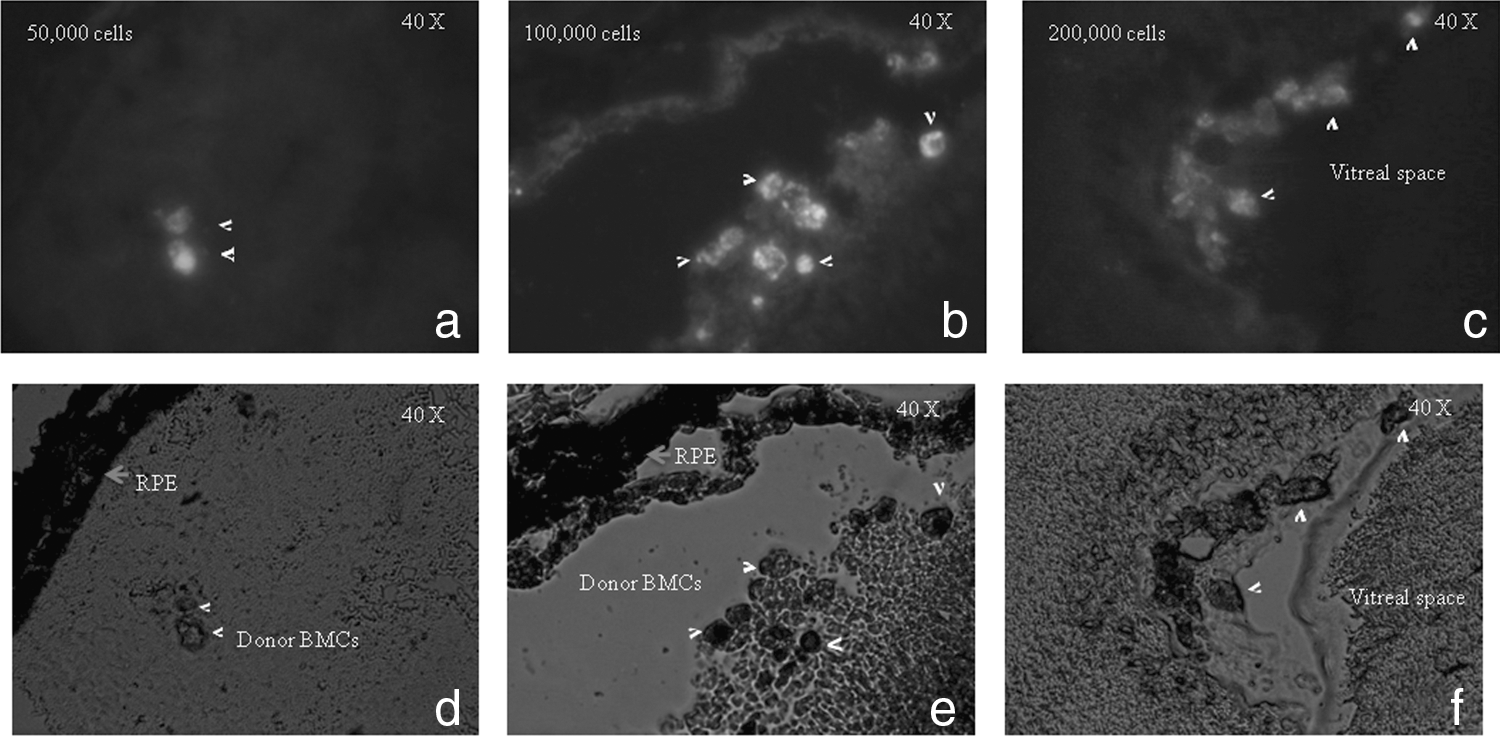
Dose-dependent incorporation of donor cells in laser-injured retina (indicated by >) at 21 days with 3 different doses of Lin-ve BMCs (50,000, 100,000, and 200,000) transplanted via intravitreal route.
Incorporation of donor Lin-ve BMCs by intravenous route
Approximately 100,000 Lin-ve BMCs were immediately transplanted after laser injury via tail vein route in mice. These cells were found to be incorporated in RPE and photoreceptor layer, where they survived up to 21 days (Fig. 3b). RPE is seen as an autofluorescent layer that can be easily differentiated from other layers of retina. Donor cells in the 11 days group were mostly found to be clustered around laser injury site (Fig. 3a, d). However, the donor cells were found to be aligned along the host photoreceptor layer by 21st day (Fig. 3b). A low-magnification image of the same section as in Fig. 3a, b shows donor cells clustered into laser injury site (Fig. 3e). In our study, it was not possible to identify the localization of the injected stem cells in the specific areas of the retina.
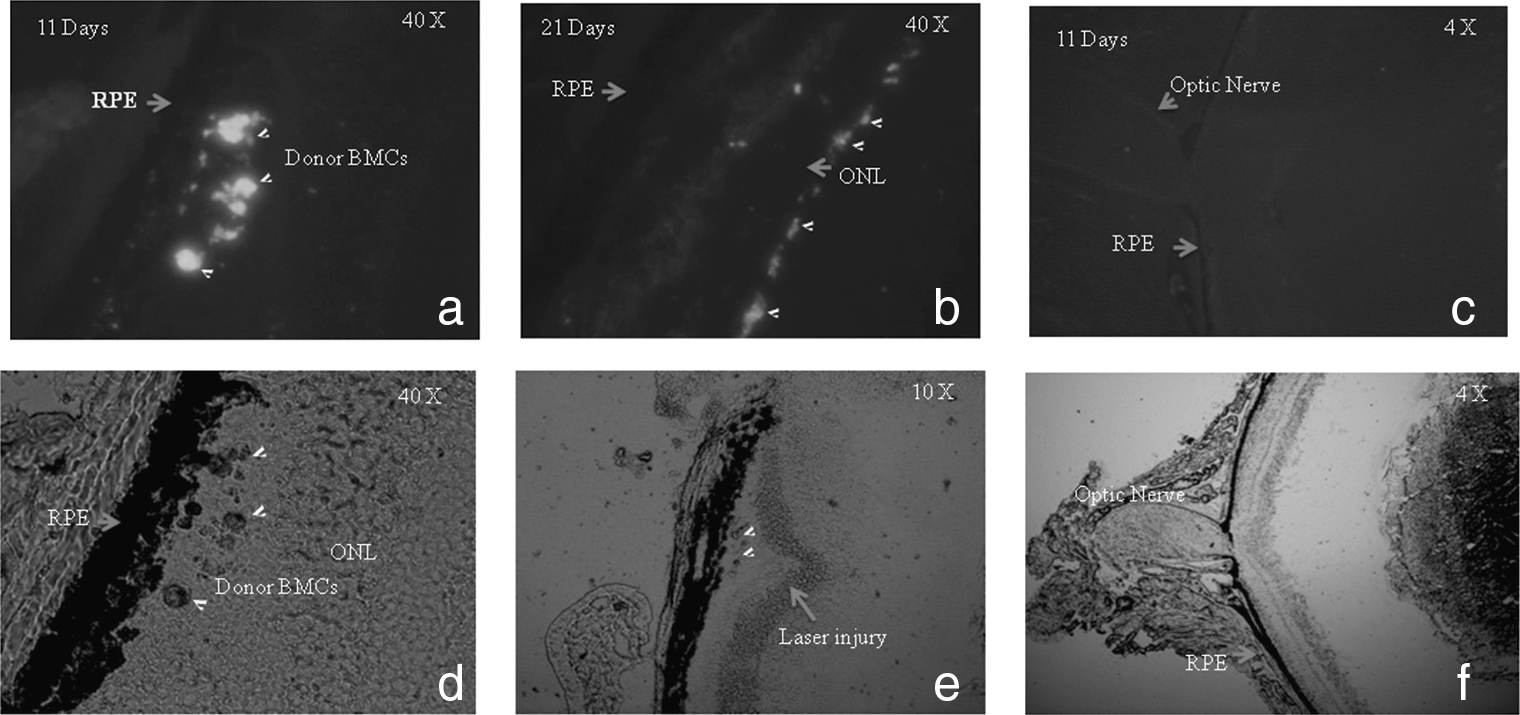
Incorporation of Lin-ve BMCs in injured retina by intravenous route. About 100,000 cells labeled with CFDA-SE were immediately transplanted after injury through tail vein and animals were sacrificed on 11th and 21st days. Donor cells were observed to be incorporated in the laser-injured retina at both time points and showed widespread incorporation and alignment along host ONL at 21st day
A comparative quantitative analysis of total number of donor cells incorporated per eye via intravenous and intravitreal routes was made for the 100,000 cells dose group for the 21 days group. The intravenous route showed better incorporation of donor cells (802±35 cells) than the intravitreal route (253±16 cells; Fig. 4). The donor cells survived up to 21 days in injured retina when transplanted either through intravenous or intravitreal route.
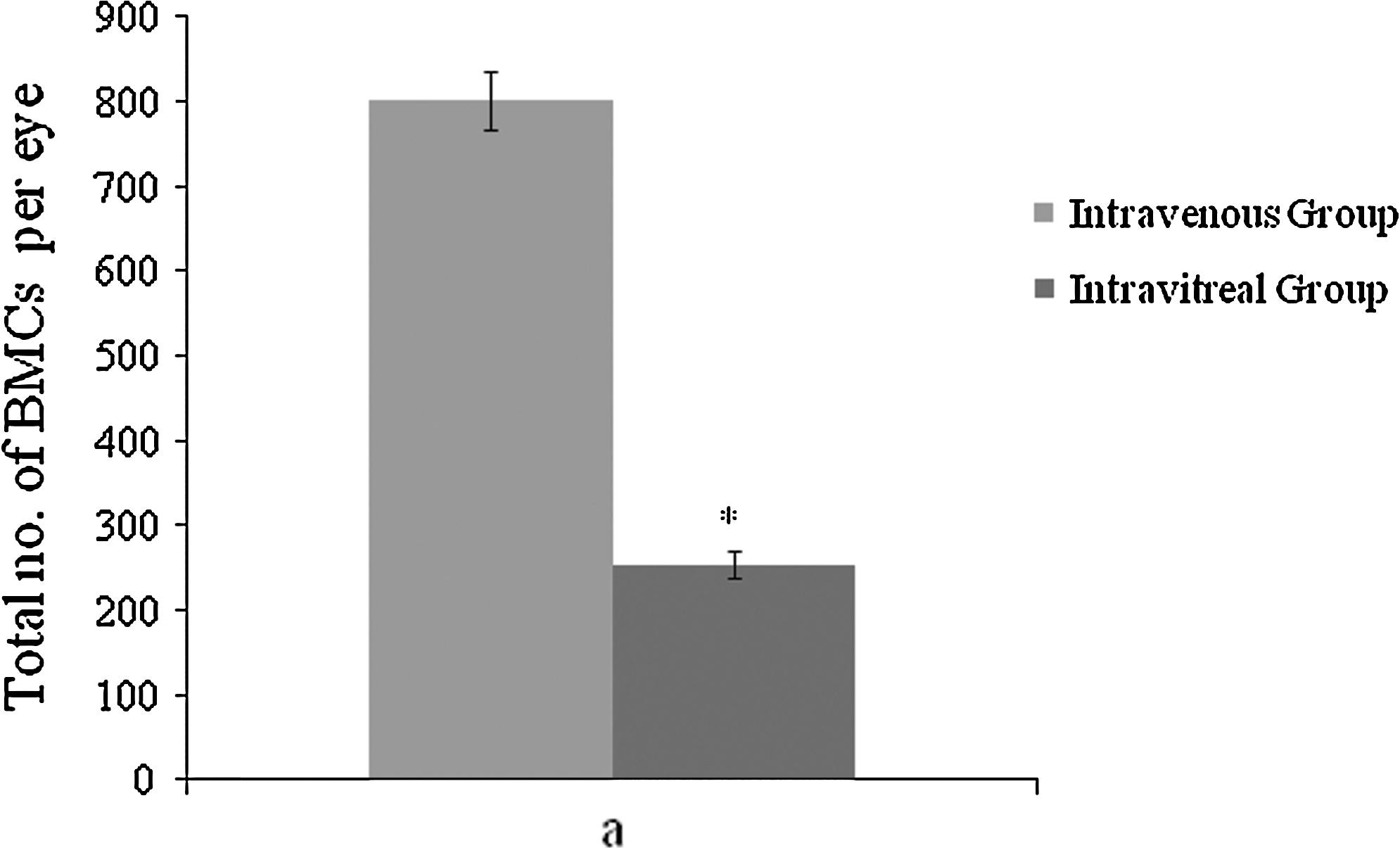
Quantitative analysis of donor BMCs in laser-injured retina. CFDA-labeled Lin-ve BMCs were transplanted through intravenous and/or intravitreal route (100,000 per animal) and cells were counted in serial sections throughout the retina at 21 days of transplantation. The total number of BMCs counted in intravenous transplantation group was found to be significantly higher than the intravitreal group (P<0.001 for intravenous group vs. intravitreal group; n=6). The data are presented as mean±standard error of the mean. Statistical analysis was performed using Student's t-test. P<0.05 was considered significant. *Statistically significant difference between two graph bars.
Role of injury in incorporation of transplanted Lin-ve BMCs
To evaluate the impact of injury on the donor cell incorporation in retina, CFDA-labeled donor Lin-ve BMCs were injected through tail vein in mice with laser injury in 1 eye only. The other eye of the same animal was not injured with laser. Donor Lin-ve BMCs were found to incorporate in the injured retina (Fig. 3a), whereas the uninjured fellow eye of the same animal did not show any incorporation of transplanted Lin-ve BMCs upto 11 days (Fig. 3c).
Discussion
Laser injury model of retina has been previously used by many workers [14,21 –25] and the mechanism and pathophysiology of laser-induced damage has been also well studied [18,26 –28]. The laser-induced damage is known to occur by photocoagulation due to heat energy liberated during interaction of laser with pigments such as melanin and hemoglobin in retina. As the BMCs have been earlier shown to migrate to site of injury [8,14], we tested whether Lin-ve BMCs exhibit equally good recruitment and survival when transplanted via intravenous and intravitreal routes upon laser injury in retina. Our results show that Lin-ve BMCs incorporated and migrated into various layers of laser-injured retina and survived up to 21 days upon transplantation by both the routes. This is consistent with reports wherein stem cells or retinal progenitors have been shown to integrate into various layers of degenerating retina of transgenic mice [4,9] or injured retina [7,15,29,30] and survive for even longer periods in retina [4,30] when compared with our analysis at 21 days.
The mammalian retina becomes somewhat resistant to transplanted cells after its complete development. Injury results in a microenvironment that is conducive for the recruitment, differentiation, and survival of stem cells. Ahmad and colleagues demonstrated that ocular stem cells do not incorporate in adult retina or uninjured retina but they do so when they are transplanted in animals with retinal injury [8,30,31]. Our study corroborates these reports as we did not observe any incorporation of transplanted cells in uninjured eye in this study. Wang et al. [32] as well as Castanheira et al. [33] have rather recently postulated the use of stem cell therapy for retinal degeneration and showed the incorporation of MSCs in injured retina of rats. Neither group showed any evidence of retinal regeneration, and neither groups' work led to any therapeutic advance. Both studies have, however, led to increased interest in this promising therapy for this devastating consequence of diabetes, a disease that is rampant in developed countries, and seems that it shall be for the foreseeable future. The need for retinal regeneration shall increase as diabetes continues to increase among members of a well-fed world.
The recruitment of BMCs to laser injury sites was observed in our study with both the routes studied, although tail vein administration showed superior homing of transplanted cells. The intravitreally transplanted BMCs settled in GCL, photoreceptor layer, and the RPE. Previous workers have also reported similar incorporation pattern of donor cells in mechanical and transgenic injury models [1,7,8]. BMCs transplanted in the vitreous cavity have to pass through different layers of retina while migrating toward the injury site in the RPE–photoreceptor junction, resulting in residual population of these cells in the GCL as observed in our study. According to recently published evidence from Jiang et al., a substantial number of retinal progenitors were subretinally injected, where they may well exist in vivo migrated into the ONL. In addition, a subpopulation of these cells develop morphological features reminiscent of mature photoreceptors, express photoreceptor specific proteins including synaptic protein, and appear to form synaptic connections with bipolar neurons [34]. Even though this observation has little bearing on our results, it underlines the importance of delivery routes in stem cell translational studies.
We have observed that the homing pattern of donor cells was notably different between 11 and 21 days intravenous groups. A widespread migration was observed in the 21 days group with a characteristic alignment of donor cells in a lateral fashion along the host photoreceptor nuclear layer. Such an arrangement of donor cells was not seen at 11 days posttransplantation. Donor cells in the 11 day group were found to be clustered around the injury site. The intravenous route provides easy access to RPE, the junction between choriocapillaris and outer retina. This partly explains why transplanted BMCs enter retina faster through choroidal vasculature, which is adjacent to RPE, the site of injury. Choroidal vasculature possesses the fastest blood supply than any other organ (about 1400 mL/min in humans), representing a focal point for transplanted BMCs to home to the injury site. Although it can be argued that our results did not provide new information facilitating stem cell treatment of retinal degeneration, to date no study has provided. No study to date has succeeded in even approaching retinal regeneration by stem cell or any other therapy. We have to start somewhere to reach this elusive goal. Thus, defining the route and dose for optimal localization of regenerative stem cell localization at the retina is of major importance at this time.
A quantitative comparison of total number of donor cells at 21 days posttransplantation (50,000 and 100,000 cells group showed an average of 82±4 cells in 50,000 cells group and 253±16 in the 100,000 group) showed better incorporation in the intravenous group as compared to intravitreal group. The highest dose of 200,000 cells delivered to the animals resulted in clumping of cells in the vitreal cavity in close contact with GCL, leading to poor migration in the retinal layers. Donor cells transplanted at a dose of 100,000 cells showed better migration, incorporation, and survival when compared with other dose groups.
Both the dose and route of the transplanted cells have clinical significance for the therapeutic applications in degenerative diseases of retina as most of the clinical trials suffer from lack of data on the optimal dose range as well as the optimal route of injecting stem cells. However, only carefully designed preclinical studies in appropriate models can provide vital clues for accurate extrapolation of results to humans. The results of these experiments can be useful for not only the cases of acute injury but also progressive disorders such as ARMD, which is characterized by breach in the Bruch's membrane, and glaucoma, in which the ganglion cell death occurs. Certain therapeutic strategies to rescue the experimental CNV in animals have been tested by delivering antiangiogenic factors via mesenchymal cells [35]. It is therefore a very attractive proposition to test BMCs for delivery of important molecules in retina. The faster incorporation of Lin-ve BMCs in retina and RPE through intravenous route may play an important role in treating retinal diseases that demand timely recruitment of cells to replace damaged photoreceptors or RPE. The role of growth factors such as vascular endothelial growth factor (VEGF), stromal cell derived factor-1 (SDF-1), and other chemokine factors on recruitment of transplanted cells to the sites of tissue damage has been well established [36]. The differentiation potential of Lin-ve BMCs observed in GCL, RPE, and photoreceptor layers in the intravitreal versus intravenous group will yield important information about the functional state of these injected cells, although several groups have earlier shown differentiation of cells analyzed at various time points and in different models. In this respect, it is pertinent to mention the work of Otani et al., who showed absence of stem cell-derived neurons in the ONL, ruling out the possibility that the injected cells are transforming into photoreceptors (PRs) [37]. This controversial study was offset by a report by Maclaren et al., who showed successful integration of rod photoreceptors that were found to be immature postmitotic rod precursors and not proliferating progenitor or stem cells [10]. In the present study, we have not been able to evaluate the functional effect of Lin-ve BMCs transplantation but assert that a side-to-side comparison between cell types, just like the comparison between delivery routes, is important to advance the field and resolve the problem. Although the study provides vital clues about effective mobilization of BMCs through the intravenous route, we have not been able to conduct side-to-side comparison of various doses of BMCs via different routes at same time points. It should be noted that there was no demonstrable incorporation of donor cells at 4 and 11 days in the intravitreal group, and because the best incorporation was observed at the 100,000 intravitreal dose group in the 21 days time point, the intravenous-related investigations and accompanying quantitative comparisons were limited for 21 days and 100,000 dose group. Further studies that compare the efficacy of transplantation of BMCs through various routes and doses of donor cells in other animal models of retinal injury or degeneration can provide insights into emerging area of biotherapeutics. The dose-dependent effect of donor cells on the incorporation pattern in injured retina emphasizes a need for standardization of dose in animal and human cell transplantation studies.
Footnotes
Acknowledgments
The authors are deeply indebted to Denis English and reviewers for stimulating discussions that shaped this revised article. The authors acknowledge the Indian Council of Medical Research, New Delhi, India, for financial support to research fellows.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.