
Abstract
The potential of autologous bone marrow (BM)-derived progenitor/stem cell (BMSC) therapy for cardiac repair maybe limited by patient-related factors, such as age and the disease process itself. In this exploratory analysis, we assessed the impact of age, different disease states, and granulocyte colony-stimulating factor (G-CSF) therapy on progenitor cell concentration and function in patients recruited to our clinical trials of BMSC therapy for ischaemic heart failure (IHD), dilated cardiomyopathy (DCM), and acute myocardial infarction (AMI). The concentrations of CD34+ cells and endothelial progenitor cells (EPCs) were measured in the peripheral blood (PB) and BM of 201 patients. Additionally, cell mobilization following G-CSF and the functional capability of CD34+ cells (using a colony-forming unit assay) were assessed. We found that older age was associated with a lower PB CD34+ cell concentration in the whole study group as well as blunting the effect of G-CSF on BMSC mobilization in IHD patients. Nonischaemic heart failure (DCM) was associated with a significantly higher baseline PB CD34+ and EPC concentration compared to IHD. Following G-CSF treatment, the CD34+ cell concentration was greater in the BM compared to PB, however, the PB CD34+ cells appeared to have a greater and improved (compared to baseline) functional potential. Our results suggest treatment with G-CSF improves the functional potential of mobilized circulating progenitor cells compared to those in the BM. Further work is required to determine which source of cells is best for the purposes of cardiac repair following G-CSF therapy.
Introduction
T
BMSCs consist of mononuclear cells (BM-MNC) and mesenchymal stem cells (MSCs). The BM-MNC fraction contains a heterogeneous population of cell types, including hematopoietic progenitor/stem cells (HSCs) identified by the CD34+ marker, monocytes (CD14+), lymphocyte subsets characterized by CD3+ (T-cells), CD19+ (B-cells), and endothelial progenitor cells (EPCs), which can be defined by CD133+ VEGFR2+ markers [7]. The CD34+ HSCs and EPCs are thought to be the cell types most likely to promote cardiac repair although the exact mechanisms remain unclear. Theoretically, these include neoangiogenesis, cell fusion, paracrine effects, including activation of survival pathways, and transdifferentiation into cardiac phenotypic cells although the latter remains under considerable debate [8,9]. Although the clinical safety of BMSCs has been demonstrated, clinical effectiveness has been less consistently shown [10 –12]. Potential reasons for this include heterogeneity in patient selection and clinical trial design. Studies have varied with regard to use of peripherally harvested stem/progenitor cells (PBSCs) or BMSCs and have also differed as to whether cells have been mobilized with G-CSF or not. Furthermore, the number and functional ability of BM-MNCs has been shown to be reduced in patients with advanced heart failure and ischaemic heart disease [13]. In particular, aging has been recognised to adversely affect the functional capacity of progenitor cells [14] and the mobilizing ability of G-CSF [15]. Hence, as the number of clinical trials using autologous cells continues to increase, a need has been identified for further mechanistic studies that include analysis of cellular composition and function of the BMSC infusate.
We are currently performing 3 randomized, double-blind, placebo-controlled trials for patients with chronic ischaemic heart failure (REGENERATE-IHD [16], clinicaltrials.gov identifier NCT00747708), dilated cardiomyopathy (REGENERATE-DCM [17], clinicaltrials.gov identifier NCT01302171), and acute myocardial infarction (REGENERATE-AMI, clinicaltrials.gov identifier NCT00765453). The IHD and DCM studies investigate the effects of G-CSF alone or in combination with intracoronary or intramyocardial delivery of autologous BMSC therapy on cardiac function and quality of life in patients with symptomatic heart failure and no further treatment options. The AMI study assesses the safety and efficacy of early delivery of intracoronary BMSC in patients treated with primary stenting for AMI. Our studies, therefore provide an ideal platform to assess the relationship between age and cardiac disease state on the concentration of peripheral and bone marrow (BM) progenitor cells as well as the response to G-CSF-mediated mobilization.
Methods
Objective
This is an exploratory analysis of progenitor cell characteristics in patients recruited to 3 randomized controlled clinical trials of BMSC therapy in patients with IHD, DCM, and AMI. Specifically, we assess the impact of age, disease state, and G-CSF on progenitor cell concentration and function.
Subjects
Peripheral blood (PB) and BM samples were obtained from 201 patients recruited to the REGENERATE- IHD, DCM, and AMI trials. All patients in the AMI analysis had a BM sample for analysis. In the IHD/DCM trials, a proportion of patients were randomized to receive only G-CSF/placebo (saline) and so did not have a BM sample for analysis. The Local Research Ethics Committee has approved the protocols of all 3 trials, which are conducted in accordance with the Declaration of Helsinki. Written informed consent has been obtained from each patient before inclusion in the trial, including consent for biochemical and cellular analysis of PB and BM.
Progenitor cell mobilization with G-CSF
Recombinant human G-CSF (Granocyte®; Chugai Pharma) was administered subcutaneously at a dose of 10 μg/Kg/day for 5 consecutive days to patients enrolled in the DCM and IHD studies. Patients in the control group received saline injections. A PB sample was obtained on days 0, 1, 2, 3, 6, and 7 for estimation of peripheral progenitor cell counts. Patients in the AMI trial did not have G-CSF treatment and a single PB sample was taken for estimation of baseline progenitor cell count.
BM aspiration
BM aspiration was performed on day 6 in patients enrolled to the DCM and IHD studies who had been randomized to receive intracoronary injection of cells/placebo. Patients in the DCM/IHD studies who were randomized to receive only G-CSF or placebo did not have BM aspiration performed. In the AMI study, BM aspiration was performed within 12 h of successful primary stenting for AMI. Aspiration was performed from the posterior superior iliac spine. 100 mL of BM was collected in twenty 10-mL syringes; each syringe contained 1 mL of heparin into which 5 mL of BM was aspirated. The BM samples, together with PB, were then delivered immediately to the Barts Health NHS Trust Stem Cell Laboratory, which is an accredited facility for the production of cellular therapeutic material.
Isolation of BM-MNCs
BM aspirates from the heparin-treated syringes were pooled into a single transfusion bag. The entire volume was then passed through a blood component transfusion set with a 200-μm filter. Autologous BM-MNCs were isolated by Ficoll-Paque (GE Healthcare) density gradient centrifugation and the heparin was washed off at this stage.
Flow cytometry analysis
BM-MNCs were characterized using flow cytometry. All flow cytometry analyses were performed using a BD FACSCanto Flow Cytometer with BD FACSDiva v 5.0.3 software (BD Biosciences). For the identification of HSC populations, cells were incubated with the fluorescein isothiocyanate (FITC)-labeled antibody against human CD45 (BD Biosciences) and the phycoerythrin (PE)-labeled antibody against human CD34 (BD Biosciences) for 15 min at room temperature.
EPCs were analyzed by initially incubating samples with mouse serum IgG (Sigma) for 15 min at 4°C with a cocktail of antibodies comprising the allophycocyanin-labeled antibody to CD133 (Miltenyi Biotec) and the PE-labeled antibody to VEGFR-2 (R&D Systems) to characterize EPCs and FITC-labeled monoclonal antibodies to CD2, CD13, and CD22 (Beckman Coulter) to identify, and therefore, eliminate inclusion of lineage-negative nonprogenitor cells. To ensure exclusion of nonviable cells in the final EPC count, cells were also incubated with a PerCP-Cy5-labeled 7AAD stain (BD Biosciences). Cells were then incubated for 15 min at room temperature with 2 mL of the Pharm Lyse™ buffer (BD Biosciences) to lyse red blood cells. Samples were washed once in phosphate-buffered saline and 20 μL of Accucount flow cytometry beads (Saxon Europe) were added before analysis.
Colony-forming unit analysis
BM-MNCs (2×104 per dish), Day 0 PB MNCs (2×105 per dish), and Day 6 PB MNCs (2×104 per dish) were seeded, in triplicate preparations, in methylcellulose plates (Methocult H4534, including stem cell factor, granulocyte-macrophage colony stimulating, and interleukin-3, Stem cell Technologies). Plates were studied under phase-contrast microscopy, and granulocyte-macrophage colony-forming units (CFU-GM; colonies >50 cells) were counted after 14 days of incubation. Results were taken from the mean of the triplicate results and presented as a ratio of CFU per CD34 cell plated. CFU assays were performed in 25 IHD, 10 DCM, and 12 AMI patients due to the availability of assay.
Statistical analysis
Data are expressed as mean±SD unless otherwise stated. Comparison of the distributions of a continuous variable between 2 independent groups was performed using an unpaired 2-sided t-test. Correlation was assessed using the Pearson r method and a P value calculated using linear regression. Analysis of covariance was used to assess for confounders. A P value of less than 0.05 was assumed to indicate statistical significance. CD34+ stem cell counts are expressed as units per μL (U/μL) and EPC count is expressed as cells per μL (EPC/μL). CFU results have been presented as a ratio of CFUs per CD34 cell plated (CFU/CD34 cell). Statistical analysis was performed with GraphPad Prism version 5.0 (GraphPad Software) and SPSS 19 (IBM).
Results
Baseline characteristics
We assessed the progenitor cell counts in 201 patients: 110 IHD, 38 DCM, and 53 AMI PB samples and 78 IHD, 17 DCM, and 53 AMI matching BM samples. Baseline characteristics of all patients are shown in Tables 1, and 2 lists the characteristics of only the patients in whom CFU analysis was undertaken.
Data presented as number (% of patients) or mean±SD.
IHD, ischaemic heart failure; DCM, dilated cardiomyopathy; AMI, acute myocardial infarction; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal prohormone of brain natriuretic peptide; N/A, not applicable; NS, not significant.
Data presented as number (% of patients) or mean±SD.
Patients in the REGENERATE-IHD study were significantly older, had a higher incidence of diabetes, and were more likely to be taking a statin.
Effect of age on progenitor cell number and function
We found an inverse relationship between age and PB CD34+ cell concentration (r=0.2, P=0.02) (Fig. 1a) in the whole study group (n=201). There was a trend toward an inverse relationship between age and EPC concentration, but this was not statistically significant (Fig. 1b). We also explored the effect of age on the mobilising ability of G-CSF in the chronic IHD patient group. The median age of 64 years was used to divide the patients into 2 groups. We found that the older age group had a lower concentration of CD34+ cells in the BM following mobilization with G-CSF (75.49±64.49 CD34 U/μL vs. 113.5±61.03, P=0.0023) (Fig. 2a). There was also a trend (P=0.09) toward lower percentage increase in circulating CD34+ cells (day 6 compared to day 0) with G-CSF in those aged above 64 years (Fig. 2b).

Correlation between age and peripheral blood (PB) progenitor cell concentration in the whole study group.
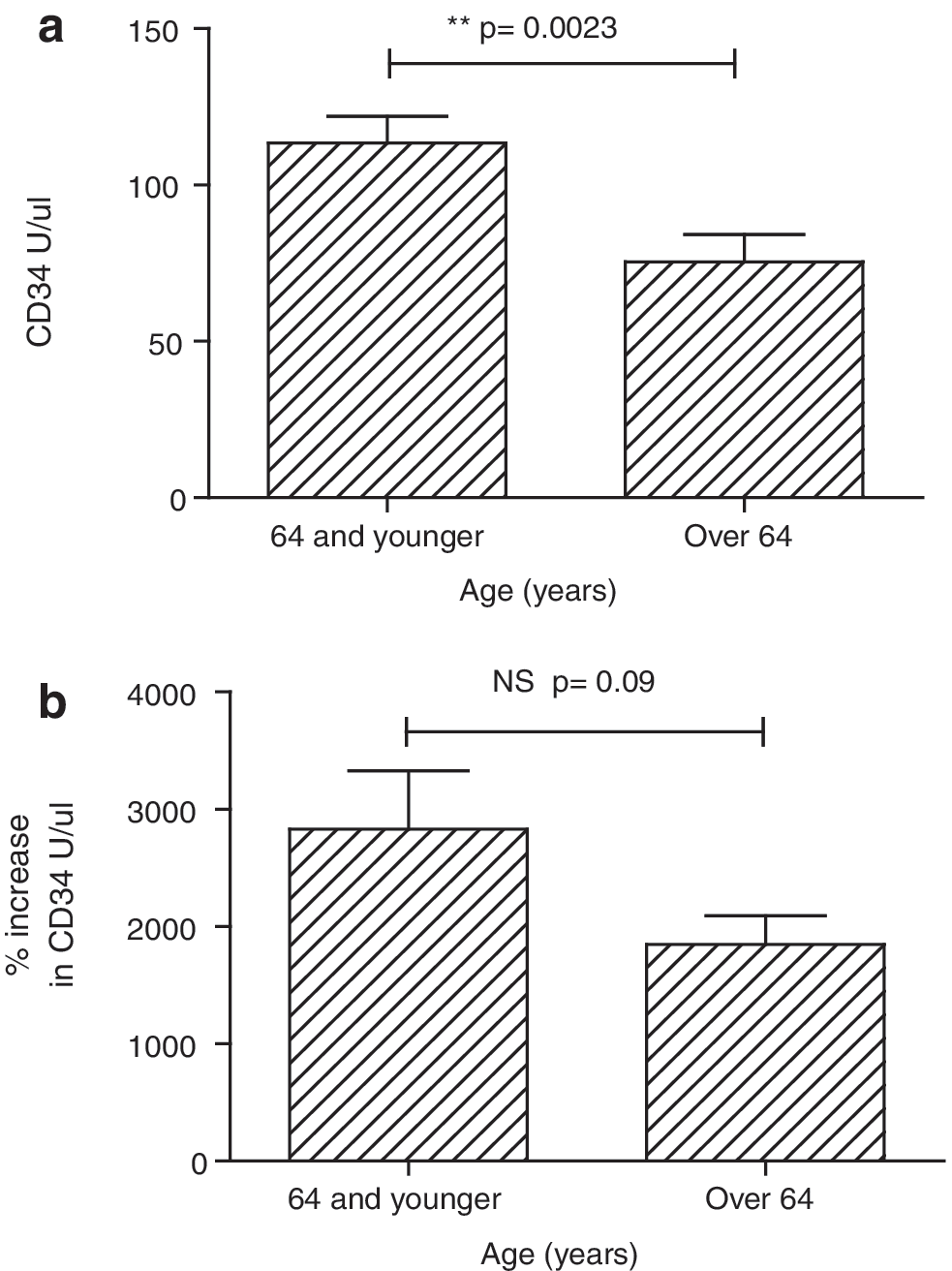
Effect of age on progenitor cell counts following the granulocyte colony-stimulating factor (G-CSF) in patients with ischaemic heart failure (IHD).
We did not find a significant difference in functional CFU potential between the age groups; however, this maybe due to the small number (n=25) of CFU assays performed.
Effect of disease state on progenitor cell number and function
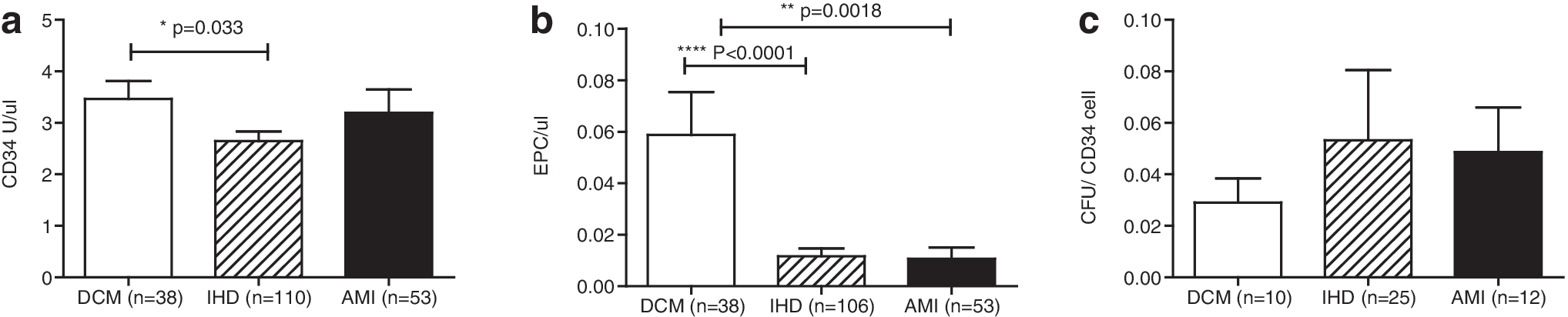
The concentration of circulating CD34+ and EPCs was found to be significantly higher in the baseline PB of DCM patients as compared to IHD patients (3.4±2.1 CD34+ U/μL vs. 2.6±1.9, P=0.033, and 0.06±0.1 EPCs/μL vs. 0.01±0.03, P<0.0001) (Fig. 3a, b). This remained significantly different after adjusting for age, diabetes, and total cholesterol. In AMI patients, the number of circulating EPCs was also significantly lower compared to DCM patients, but similar to IHD patients. Despite there being a higher circulating CD34+ cell count in the DCM patients, the CFU potential was not significantly different (Fig. 3c).
Comparison of baseline concentration of
Effects of G-CSF mobilization
The G-CSF treatment led to a substantial and comparable increase in the peripheral concentration of CD34+ cells in both IHD and DCM patients, day 6 concentration of 52.3 CD34 U/μL compared to 2.7 CD34 U/μL on day 0 (Fig. 4). There was no significant increase in cell concentration in patients who received saline injection only (day 6 concentration of 2.7 CD34 U/μL from baseline of 2.2 CD34 U/μL).
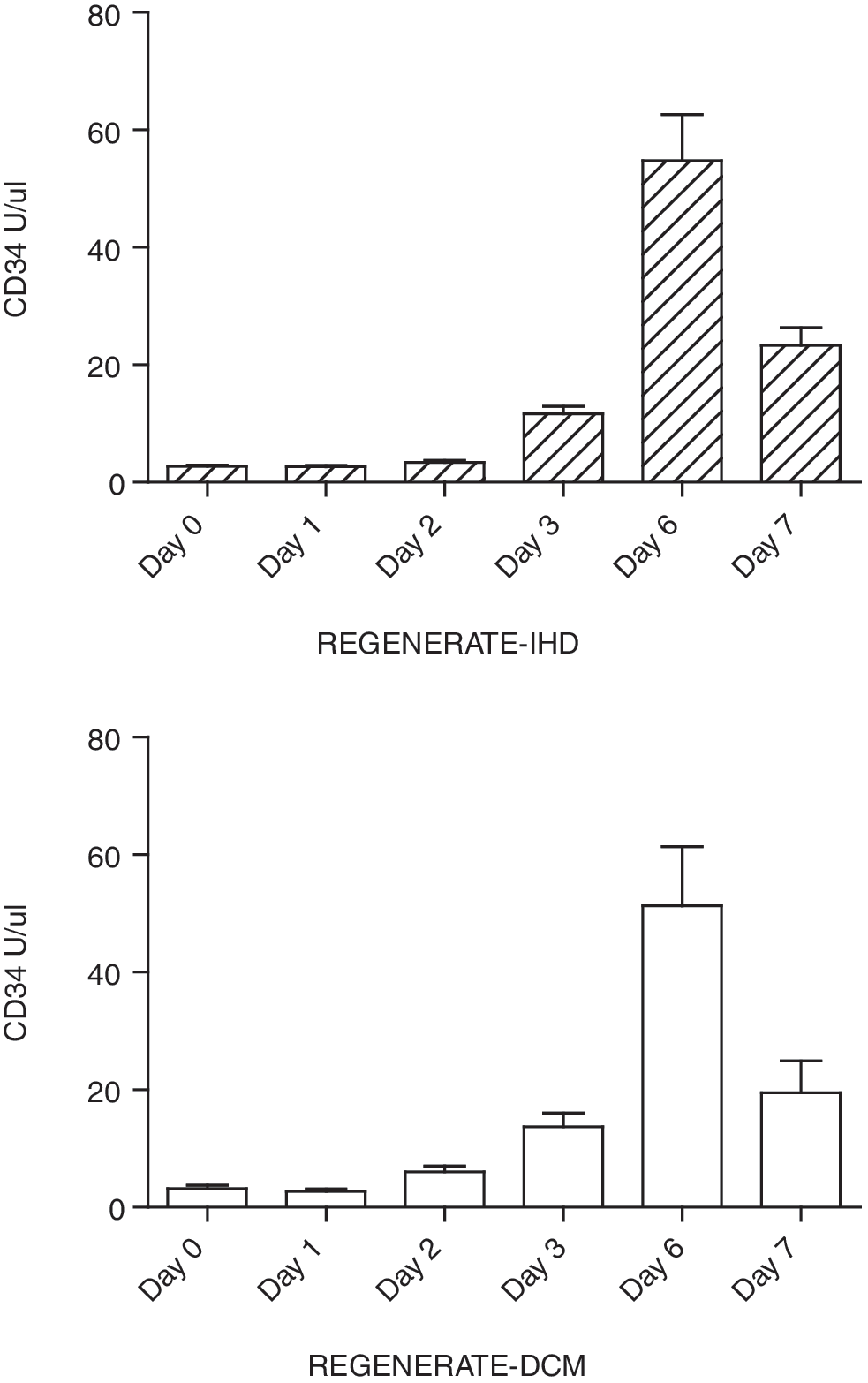
Effects of G-CSF on PB CD34+ cell counts in IHD (top panel) and DCM (bottom panel) showing comparable increase in circulating progenitor cells with a similar peak on day 6.
The progenitor cell count in the BM of IHD and DCM patients was similar following treatment with G-CSF. The increase in BM progenitor cell counts following G-CSF mobilization can be appreciated by comparing the IHD and DCM BMs with that of AMI patients who did not receive G-CSF (Fig. 5).

Comparison of bone marrow progenitor cell counts in the 3 different cohorts showing a significantly higher bone marrow progenitor cell concentration with 5 days G-CSF treatment (DCM and IHD patients) compared to no G-CSF (AMI patients).
The concentration of CD34+ cells in the BM aspirated on day 6 was significantly higher than in the PB on the same day (Fig. 6a, b). However, the CFU functional assessment (Fig. 6c) suggests that PB cells appear to be more functionally active than BM cells (0.15±0.14 CFU/CD34 cell vs. 0.08±0.05, P=0.0081). Furthermore, the CFU/CD34 cell ratio in the PB increases significantly with G-CSF (Fig. 6d), suggesting mobilization of functionally active progenitor cells.

Comparison of PB and bone marrow CD34+ concentration following G-CSF mobilization in
Discussion
The past decade has seen a large increase in the number of clinical trials being performed to assess the safety and efficacy of BMSC therapy for cardiac disease. Only a few of these studies have examined progenitor cell concentration and function in recruited patients [18 –20], an important consideration given the varying degrees of efficacy demonstrated.
The data from this present study confirm previous reports of an inverse relationship between age and PB CD34+ cell concentration in patients with cardiac disease. We have also shown that, in IHD patients, the concentration of BM CD34+ progenitor cells, following G-CSF mobilization, is lower in patients aged above the median age of 64 years (Fig. 2a). There was also a trend toward reduced peripheral mobilization by G-CSF in the older age group (Fig. 2b). The adverse effects of age on progenitor cell number and function has been increasingly recognised [14]. In healthy individuals and patients with coronary artery disease, increasing age is associated with reduced number and function of cultured EPCs and CD34+ cells in the BM [14,21]. Older age is also associated with significantly reduced BM-derived progenitor cell mobilization in patients after AMI [22]. In the recent FOCUS-HF study of intramyocardial injection of BM-MNCs in IHD [19], the number and function of progenitor cells was significantly higher in patients ≤60 years than in patients >60 years. Interestingly, following treatment, objective evidence of improvement (by MVO2) was only seen in the patients <60 years. Hence, the impact of age on BM progenitor cell number and function may limit the efficacy of cell therapy in some patients. This may, in part, explain some of the discrepant clinical trial results, and further work is required to identify the age group of patients that will derive the most benefit of cell therapy.
We have also shown that concentration of circulating CD34+ cells and EPCs are higher in patients with DCM than in those with IHD (Fig. 3a). The number of circulating EPCs is also lower in AMI patients compared to DCM (Fig. 3b). This is consistent with previous reports showing circulating EPCs inversely correlate with number of risk factors for coronary artery disease [23]. Although there was a higher concentration of circulating CD34+ cells in DCM patients, the CFU analysis suggested that there was no difference in functional capability. It is possible that this finding maybe due to an adverse effect of heparin on progenitor cell function as has been recently reported by Professor Zeiher's group (unpublished data), although our data is based on a small number of CFU assays and heparin exposure was similar across all samples. The difference in circulating progenitor cells between IHD and DCM has not previously been demonstrated suggesting that the atherosclerotic process rather than chronicity or severity of disease is the important determinant of the progenitor cell concentration.
G-CSF has been used to mobilize BM progenitor cells in patients with cardiac disease either on its own, as adjuvant therapy with peripheral leukapheresis (PBSCs) or BM harvest, and subsequent direct delivery of progenitor cells to the heart [24 –26]. It is still debated whether G-CSF treatment leads to an increase in progenitor cells in the BM in addition to the mobilization of these cells into the PB. Studies in patients undergoing myeloablative therapy suggest that the transplantation of mobilized allogeneic PBSCs may lead to an earlier recovery in BM function compared to cells obtained from a marrow harvest [27,28]. Our data show that the concentration of CD34+ cells in the BM following 5 days of G-CSF treatment is higher than in the PB on that day (Fig. 6a, b). Conversely, CFU analysis suggests a significantly higher functional potential of the CD34+ cells in the PB compared to BM (Fig. 6c). Several studies have suggested that G-CSF therapy leads to a migration of primitive (potentially more functional) progenitor cells from the BM into PB. These include 2 experimental studies in mice, which showed that after 5–7 days of G-CSF treatment there was a significant reduction in the number of stem/progenitor cells in the BM compartment [29,30].
In contrast to BM transplantation following myeloablative therapy, there is yet to be a published clinical trial comparing the safety and efficacy of mobilized PBSC versus mobilized BMSC for the purposes of cardiac repair. There have, however, been clinical studies comparing the relative efficacy of ex vivo expanded PBSCs and nonmobilized BMSCs. The recent HEBE trial [10] found no improvement in global or regional LV function with either intracoronary PBSC or BMSC compared to standard therapy. In contrast to this, the earlier TOPCARE-AMI study [31] found significant beneficial effects of both PBSCs and BMSCs on LV function. The same group also compared the efficacy of intracoronary BMSCs or PBSCs in patients with chronic IHD in the TOPCARE-CHD study [32]. In this study, only BMSCs appeared to have a beneficial effect on improving LV function with no significant effect of PBSCs. The potentials reasons given for this include the smaller number of progenitor cells derived from PB as well as the fact that circulating progenitor cells are known to be reduced in number and function in patients with heart failure [33]. The PBSCs were not mobilized with G-CSF before harvest, which could have led to a positive effect, particularly, as our study shows that G-CSF can lead to mobilization of functionally active cells (Fig. 6d).
Our findings are clinically important and indicate that further work is required to define whether peripheral or BM harvest of progenitor cells is best for treating patients with heart failure. The possibility that pretreatment with G-CSF may correct for deceased CFU potential, and hence the regenerative capacity of cells from patients with ischaemic heart disease is an important observation that needs further investigation.
Limitations
This is an exploratory analysis, which limits the conclusions that can be drawn, but at the same time generates interesting hypotheses to be examined in future studies. Our study is limited by the lack of a true normal patient control group for comparison although the comparison between disease states provides valuable information. Our analysis is also limited by the lack of CFU-GM assays being performed in all the patients analyzed; this was due to an issue with availability. We would also ideally have assessed for functional ability of the MSC fraction of BM, with a colony-forming unit fibroblast (CFU-F) assay as was done in the recent FOCUS-HF study [19].
Conclusions
Ageing appears to have an adverse effect on circulating CD34+ cell concentration. Furthermore, in patients with IHD, BM concentration of CD34+ cells following mobilization with G-CSF is lower in older patients and PB mobilization is also impaired. The disease process itself also appears to have an effect on PB progenitor cell counts, which are lower in patients with IHD as compared to those with nonischaemic heart failure (DCM). The progenitor cell concentration, following G-CSF mobilization, is significantly higher in BM than PB and the BM harvest may therefore provide a higher progenitor cell yield than the peripheral harvest. However, our functional analysis suggests that peripherally harvested progenitor cells may be more functionally active than those obtained from the BM harvest following G-CSF mobilization. Further studies are therefore required to clarify the effects of G-CSF on BM and circulating progenitor cells, and ultimately, their ability to engraft and improve cardiac function and symptoms in patients with heart failure.
Footnotes
Acknowledgments
This work was funded by unrestricted grants from Heart Cells Foundation, Barts & The London Charity, Chugai Pharma UK and Cordis Corporation.
Institution where work performed: The London Chest Hospital, Barts and the London NHS Trust.
This work forms part of the research themes contributing to the translational research portfolio of Barts and The London Cardiovascular Biomedical Research Unit, which is supported and funded by the National Institute of Health Research.
Author Disclosure Statement
No conflict of interests declared