
Abstract
Delayed engraftment is a significant limitation of umbilical cord blood (UCB) transplantation due to low stem cell numbers. Inhibition of dipeptidyl peptidase (DPP)-4 enhanced engraftment in murine transplants. We evaluated the feasibility of systemic DPP-4 inhibition using sitagliptin to enhance engraftment of single-unit UCB grafts in adults with hematological malignancies. Twenty-four patients (21–58 years) received myeloablative conditioning, followed by sitagliptin 600 mg orally days −1 to +2, and single UCB grafts day 0. Seventeen receiving red cell-depleted (RCD) grafts, matched at 4 (n=10) or 5 (n=7) of 6 human leucocyte antigen (HLA) loci with median nucleated cell dose 3.6 (2.5–5.2)×107/kg, engrafted at median of 21 (range, 13–50) days with cumulative incidence of 94% (95% confidence interval, 84%–100%) at 50 days. Plasma DDP-4 activity was reduced to 23%±7% within 2 h. Area under DPP-4 activity-time curve (AUCA) correlated with engraftment; 9 of 11 with AUCA <6,000 activity·h engrafted within ≤21 days, while all 6 with higher AUCA engrafted later (P=0.002). Seven patients receiving red cell replete grafts had 10-fold lower colony forming units after thawing compared with RCD grafts, with poor engraftment. Systemic DPP-4 inhibition was well tolerated and may enhance engraftment. Optimizing sitagliptin dosing to achieve more sustained DPP-4 inhibition may further improve outcome.
Introduction
We focused on a simple, inexpensive approach to enhance UCB engraftment. Stromal-derived factor (SDF)-1α, and its receptor CXCR4 play key roles in homing/nurturing of hematopoietic stem/progenitor cells [7,8]. Dipeptidyl peptidase (DPP)-4 regulates the chemotaxis and engraftment effects of SDF-1α [9,10], expresses as surface CD26 on hematopoietic stem/progenitors and other cell types [9,10], and is also present in a catalytically active soluble form in plasma [11]. DPP-4 cleaves N-terminal dipeptides from a variety of substrates including SDF-1α at the penultimate proline or alanine [12,13]. Truncated SDF-1 (aa 3–68) cannot activate CXCR4, but antagonizes signals from full-length SDF-1α [9,10]. We demonstrated that inhibition of DPP-4 enhances chemotaxis of human UCB CD34+ cells to a SDF-1α gradient [9]. Further, inhibition or deletion of DPP-4 enhances engraftment of mouse bone marrow cells [10] and human UCB CD34+ cells [13 –15] in mice. Finally, intravenous or oral administration of a DPP-4 inhibitor to lethally irradiated mice also enhances engraftment of untreated mouse marrow cells [16 –18]. Based on these data, we conducted a pilot trial evaluating feasibility and safety, and potential efficacy of systemic inhibition of DPP-4 using orally administered sitagliptin, an FDA approved DPP-4 inhibitor, to enhance engraftment of single-unit UCB transplants in adults with high-risk hematological malignancies.
Design and Methods
Patients
Eligible patients had high-risk acute myeloid leukemia (AML) or acute lymphoblastic leukemia in complete remission (CR) or relapse, refractory aggressive non-Hodgkin's lymphoma (NHL), or refractory chronic myelogenous leukemia. Patients were aged 18–59 years, had a Karnofsky performance status ≥70%, cardiac left ventricular ejection fraction >45%, gas transfer diffusing capacity of lung for carbon monoxide>50%, creatinine clearance >60 mL/min/1.73 m2, and serum bilirubin<2×upper limit of normal. Treatment was restricted to patients lacking human leucocyte antigen (HLA)-identical related or well-matched volunteer unrelated donors, or if the patient's disease was unstable, matched adult donor cells could not be procured within 4 weeks. The trial was approved by the Indiana University Institutional Review Board and was registered at ClinicalTrials.gov (NCT00862719). All patients gave written informed consent.
Selection of UCB grafts
Single UCB units were used as we felt that this was the only way to definitively investigate potential efficacy of effects on HSC engraftment. UCB units were matched at 4 or more of 6 HLA loci (HLA-A, -B, -DRB1) with recipient, and they contained a minimum nucleated cell (NC) dose of 2.5×107/kg recipient body weight before freezing. Donor units with the best HLA-match were preferred, and within an HLA match level units with greatest NC numbers were selected.
Treatment
Patients received 13.2 Gy total body irradiation in 8 fractions on days −7 to −4, cyclophosphamide 60 mg/kg on days −3 and −2, and rabbit antithymocyte globulin (ATG) 2.5 mg/kg on days −4 to −2. To reduce the risk of infection, the protocol replaced ATG with fludarabine 30 mg/m2 on days −4 to −2 after the first 11 patients were enrolled. UCB units were thawed and washed as previously described [19] and infused on day 0. Sirolimus and tacrolimus were administered for graft-versus-host disease (GvHD) prophylaxis, as previously reported [20]. Sitagliptin (Januvia®; Merck & Co., Inc., Whitehouse Station, NJ) 600 mg every 24 h was orally administered from days −1 to +2. The dose of sitagliptin was based on pharmacodynamic studies in healthy volunteers demonstrating >90% plasma DPP-4 inhibition that was sustained for more than 24 h following 600 mg doses [21]. Filgrastim (5 μg/kg/day subcutaneously) was started on day +5 and continued until neutrophil recovery. Patients received antibiotic prophylaxis against bacterial, fungal, and viral infections.
Pharmacokinetic and pharmacodynamic studies
Blood was collected for sitagliptin levels and plasma DPP-4 activity at baseline, and then at multiple time points between 0.5 and 24 h after the first dose, and between 2 and 24 h after subsequent doses for plasma DPP-4 activity. Sitagliptin concentrations were quantified by liquid–liquid extraction and high-performance liquid chromatography tandem mass spectrometry (API 3200; Applied Biosystems, Toronto, Canada) using fluoxetine as the internal standard. The lower limit of quantification was 0.5 ng/mL. Plasma DPP-4 activity was assayed using the DPPIV-Glo Protease Assay (Promega, Madison, WI), according to manufacturer's instructions.
Definitions and statistical analysis
Engraftment was defined as achieving an absolute neutrophil count (ANC) >0.5×109/L for 3 consecutive days with donor derived cells, confirmed by short tandem repeat loci analysis of blood or bone marrow [22]. Platelet recovery was defined as achieving platelets >20×109/L without transfusion for 7 consecutive days. Acute and chronic GvHD were graded using standard criteria [23,24], and toxicity using the NCI Common Terminology Criteria for Adverse Events v3.0.
Cumulative incidences of neutrophil and platelet engraftment were calculated from day 0 until neutrophil engraftment and platelet recovery, respectively, with death prior to recovery a competing risk. Cumulative incidence of non-relapse mortality (NRM) was calculated from day 0 to death from any cause other than relapse, with death due to relapse a competing risk. Event-free survival (EFS) and overall survival (OS) were secondary endpoints, calculated using the Kaplan–Meier method [25]. The independent association of the extent of plasma DPP-4 inhibition, as measured by area under the curve of residual plasma DPP-4 activity, with myeloid recovery earlier than the median time to engraftment was studied using multivariable logistic regression analysis using a backward selection strategy, controlling for baseline clinical characteristics known to affect engraftment [26,27], including age, NC dose, disease status at time of transplantation, and degree of HLA mismatch. For all analyses, a 2-sided α-value of 0.05 was considered significant.
Results
Patients and UCB grafts
Twenty-four consecutive patients undergoing UCB transplantation at Indiana University Medical Center between December 2009 and December 2011 were enrolled in this study(Table 1). Seventeen patients received red cell-depleted (RCD) and 7 received red cell-replete, plasma-depleted (PD) UCB grafts. As shown in Table 2, there was no significant difference between RCD and PD units in pre-freezing or post-thawing NC doses, cell viability and recovery, and CD34+ cell dose infused. However, median colony forming unit (CFU) numbers after thawing were almost 10-fold lower in PD compared with RCD grafts (P=0.0002).
CML patient in late chronic phase failed treatment with 3 tyrosine kinase inhibitors.
AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; NHL, non-Hodgkin's lymphoma; CML, chronic myelogenous leukemia; CR, complete remission, Rel Ref, relapsed and/or refractory; UCB, umbilical cord blood; RCD, red cell depleted UCB graft; PD, plasma depleted UCB grafts; HLA, human leucocyte antigen.
All results presented as median (range).
P-value reflects 2-sided significance level of comparison between RCD and PD grafts (Mann–Whitney test).
NC, nucleated cell; CFU, colony forming unit.
Engraftment and hematopoietic recovery
CFU numbers have been reported to be strongly associated with engraftment [28]. As CFU numbers in PD units were much lower than in RCD units, and could therefore confound evaluation of effects of DPP-4 inhibition, engraftment kinetics were separately analyzed for the RCD and PD groups. Of 17 patients transplanted with RCD units, 1 died on day 29 due to sepsis with beginning neutrophil recovery (ANC 0.3×109/L) at time of death. All remaining 16 patients survived beyond day +30 and engrafted with donor-derived hematopoiesis by day +50. Median time to engraftment was 21 (range, 13–50) days (Fig. 1a), and the cumulative incidence of neutrophil engraftment by day +30 was 88% [95% confidence interval (CI) 74%–100%], and 94% (95% CI, 84%–100%) by day +50. The median percent donor chimerism at time of engraftment was 100% (range, 74%–100%). Median time to platelet recovery to >20×109/L was 77 (range, 48–220) days, with a cumulative incidence of 71% (95% CI 52%–96%) by day +100 (Fig. 1b). Three of the 17 patients receiving RCD UCB units died on days +29, +36, and +56 due to sepsis, cytomegalovirus (CMV) pneumonitis, and relapse of AML, respectively, before platelet recovery. All 14 remaining patients recovered platelet counts, although precise evaluation of platelet recovery was difficult in 4 patients because of thrombotic microangiopathy (n=3) or continuing need for platelet transfusions for gastrointestinal bleeding (n=1). Of the patients who received RCD grafts, the median time of neutrophil engraftment for patients who received ATG (n=7) was 19 (range, 13–29) days, compared with a median of 23 (range, 16–50) days for patients who received fludarabine as part of the preparative regimen (n=10) (P=0.20; Log-rank test). Thus, while the trend was for longer time to myeloid engraftment with fludarabine, there was no statistical difference between patients who received ATG or fludarabine. Engraftment was durable in all patients and no cases of secondary graft failure were observed.
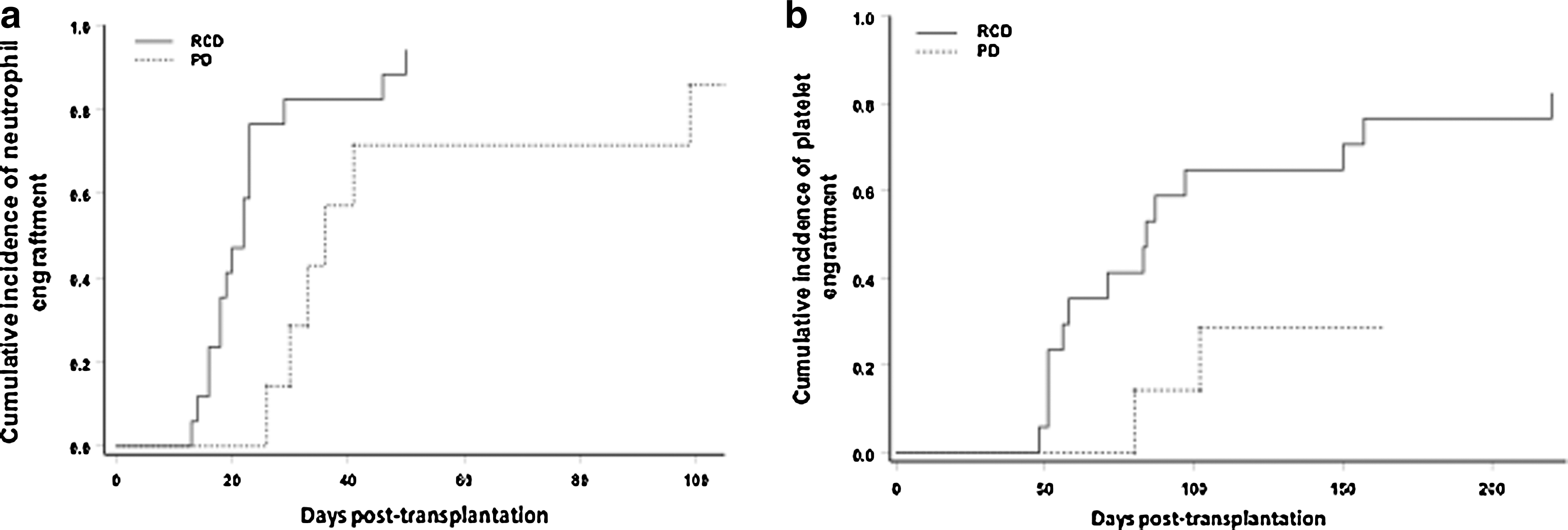
Engraftment kinetics.
For the 7 patients receiving PD grafts, 1 died of sepsis on day +105 without engraftment. Median time to neutrophil engraftment was 36 (range, 26–99) days, with 2 patients engrafting by day +30. The longer time to myeloid engraftment with PD grafts likely reflects the much lower CFU numbers infused in these units. Only 2 of 7 patients receiving PD units achieved platelets >20×109/L on days +80 and +102.
Toxicity, NRM, and GvHD
Grade 3–4 toxicity for all 24 patients included gastrointestinal (vomiting, diarrhea, and oral mucositis) (n=12), acute renal insufficiency (n=2), sinusoidal obstruction syndrome (n=3), thrombotic microangiopathy (n=3), acute cholecystitis (n=1), gastrointestinal bleeding (n=1), and posterior reversible encephalopathy syndrome that resolved on discontinuation of tacrolimus and sirolimus (n=1). No patient developed hypoglycemia.
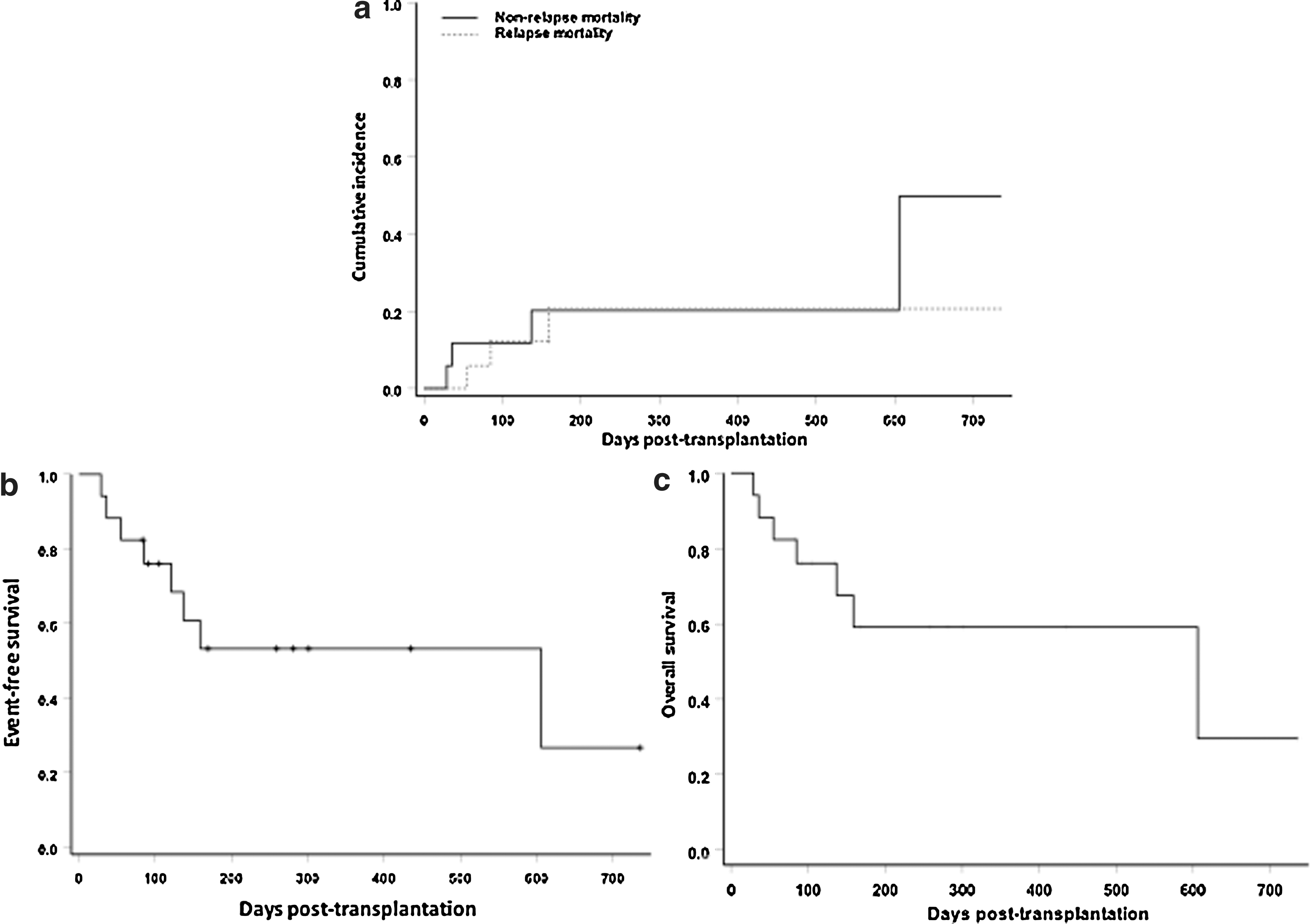
The cumulative incidences of NRM at 6 months and 1 year for patients transplanted with RCD grafts were both 20% (95% CI 7%–57%) (Fig. 2a). Of 17 patients transplanted with RCD units, 4 died of infection, including Staphylococcus aureus pneumonia (day +29), CMV pneumonitis (day +36), Klebsiella pneumoniae septicemia (day +137), and pulmonary aspergillosis in context of corticosteroid therapy for chronic GvHD (day +606). Of 7 patients transplanted with PD grafts, 6 died of infectious complications, including HHV-6 (n=1), adenovirus (n=1), toxoplasmosis (n=1), and bacterial sepsis (n=3).
Mortality and survival for patients receiving RCD umbilical cord blood (UCB) transplants.
Among 17 patients receiving RCD grafts, only 1 developed grade II acute GvHD on day +259 while tapering immune suppression. Of 11 patients who survived beyond day +100, 1 developed de novo extensive stage chronic GvHD and died of infection on day +606. No GvHD was observed among patients transplanted with PD units.
EFS and OS
Response, EFS and OS were all secondary endpoints of the study. Overall, all 11 patients with active leukemia (n=8) or NHL (n=3) at time of transplantation achieved CR. Among the 17 patients receiving RCD units, 4 with refractory AML at transplantation died of relapse between days +55 to +159. After a median follow-up of 259 (range, 84–736) days for surviving patients, median EFS and OS for patients receiving RCD grafts were both 606 days (Fig. 2b, c). One-year EFS was 53% (95% CI, 33%–87%) and 1-year OS was 59% (95% CI, 38%–92%), with 9 of 17 patients alive and disease-free beyond days +84 to +736. Of 7 patients receiving PD grafts, only 1, engrafting on day +26, remains alive with normal blood counts and ongoing CR at day +308.
Sitagliptin pharmacokinetics and pharmacodynamics
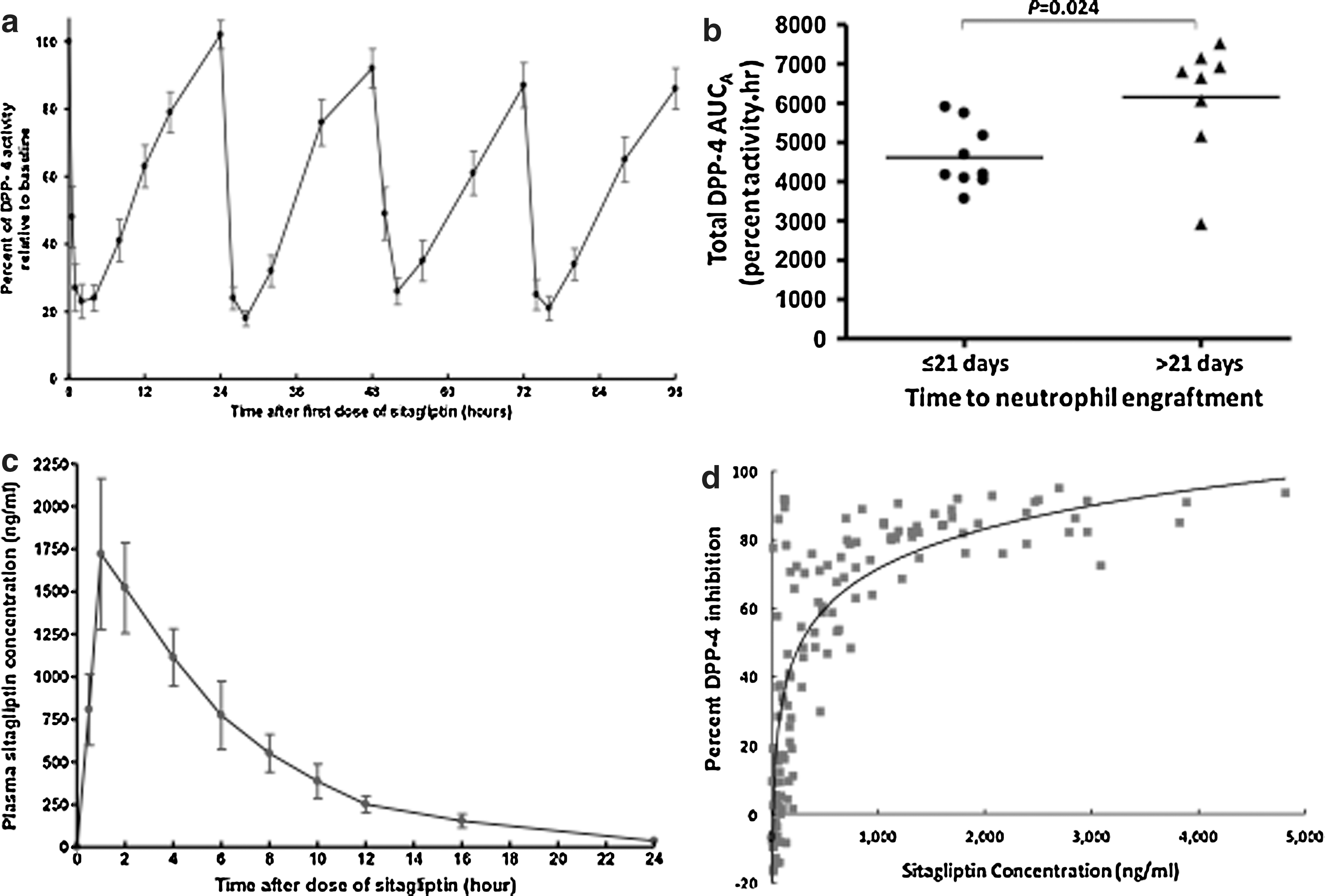
Although there was no significant difference in extent of plasma DPP-4 inhibition between patients receiving RCD and PD grafts (P>0.1, all time points), only the results for RCD transplants are presented because we wished to correlate DPP-4 inhibition with engraftment without the confounding effect of low CFUs associated with PD grafts. As shown in Fig. 3a, maximal inhibition of plasma DPP-4 activity occurred 2–4 h after dosing. Mean (±standard error) DPP-4 activity was 23%±7% of baseline 2 h after sitagliptin administration. However, DPP-4 inhibition was not sustained, returning to 80% or more of baseline by 16 h after each dose.
Sitagliptin pharmacokinetics and pharmacodynamics.
To correlate plasma DPP-4 inhibition with engraftment, the sum of areas under the percent residual activity of DPP-4 versus time curve (AUCA) for each day of sitagliptin dosing was calculated. There was no significant difference between the total AUCA for patients receiving RCD grafts (median 5,169 h·activity, range 2,932–7,530 h·activity) and that for patients receiving PD grafts (median 5,841 h·activity, range 3,198–9,042 h·activity; P=0.37). For patients receiving RCD UCB grafts, the total AUCA of patients engrafting within ≤21 (range,13–20) days was compared with that of patients taking longer to engraft(range, 22–50 days) (Fig. 3b). Median total AUCA for patients engrafting in ≤21 days was 4,189 (range, 3,563–5,903) h·activity, compared with 6,729 (range, 2,932–6,155) h·activity for patients engrafting >21 days (P=0.024; Mann–Whitney test). Nine of eleven patients with total AUCA<6,000 h·activity engrafted before day +21, while all 6 with higher total AUCA engrafted later (P=0.002; Fisher's exact test). On multivariable logistic regression analysis, a lower AUCA was the only significant factor associated with engraftment earlier than 17 days, after adjusting for age, TNC dose, HLA mismatch (1 vs. 2 mismatches), and presence of active leukemia at time of transplantation [odds ratio 0.25 (95%CI 0.10–0.89); P=0.03].
Plasma sitagliptin concentration profile for the 17 patients receiving RCD grafts is summarized in Fig. 3c. Median maximum concentration (C max) of 1,690 (range, 119–4,813) ng/mL was achieved at median T max of 2 (range, 0.5–4.8) h, and the median elimination half-life (t 1/2) was 3.9 (range, 3.0–8.5) h. Median plasma sitagliptin AUC0–∞ was 11,661 (range, 711–31,766) ng/mL·h. Overall, greater plasma DPP-4 inhibition was observed when higher plasma sitagliptin concentrations were achieved (Fig. 3d). There was no significant difference in AUC0–∞ between patients who engrafted within 21 days and those engrafting later (P=0.41; data not shown).
Discussion
We describe feasibility and safety in the first clinical trial investigating DPP-4 inhibition to enhance engraftment following single-unit UCB transplantation in adults with hematological malignancies. The observed median time to engraftment of 21 days using single UCB units compares favorably with a majority of reports where comparable cell doses were infused. Further, our result is especially noteworthy since most of our recipients received 4/6 HLA matched grafts and most had active marrow involvement by leukemia at the time of transplantation, which is a significant factor associated with a longer time to engraftment [27].
Multiple studies have demonstrated adverse effects of low cell dose on engraftment, transplant-related mortality, and survival [29 –32]. A New York Blood Center study of over 600 myeloablative single-unit UCB transplants showed that to achieve 1-year OS of >50%, NC dose must be ≥2.5×107/kg for 5/6 HLA-matched, and ≥5×107/kg for 4/6 matched units [33]. However, only a minority of adults will find UCB units based on these recommendations. Therefore, enhancing engraftment of lower cell doses will likely significantly impact outcomes.
Although the optimal approach to enhance engraftment by inhibiting DPP-4 (ex-vivo or systemic) is uncertain [16 –18], we used oral sitagliptin to avoid the complexity and regulatory hurdles associated with ex vivo manipulation of UCB, and developed a simple, inexpensive method easily usable by transplantation centers. Sitagliptin is a selective inhibitor of DPP-4 approved by the FDA for treatment of type II diabetes mellitus [34]. In this study, sitagliptin used at 600 mg/day was well tolerated and was not associated with any apparent additional toxicity than might be expected in the setting of myeloablative conditioning and UCB transplantation. Importantly, inhibition of DPP-4 yielded favorable engraftment kinetics, with a median time to neutrophil engraftment of 21 days and a cumulative incidence of engraftment of 94% (95% CI 84%–100%) at 50 days in patients receiving RCD grafts. Our results compare favorably with major published series where predominantly adult patients with hematological malignancies received either single or double UCB grafts [27,35 –39], as reviewed in Table 3. As shown, most reported median times to engraftment have been 22 days or longer with the exception of the series reported by Sanz et al. [27], which included a significant number of pediatric patients and only 21% of patients had active disease at the time of transplantation. In the latter report [27], active disease at the time of transplantation was the single most important factor adversely affecting engraftment. Nonetheless, there is significant limitation in evaluating the engraftment kinetics observed in our study relative to those in published reports because of significant differences in important variables that could affect engraftment, including cell dose, degree of HLA match, disease phase, and age of patients treated. However, in the largest, recently updated reported series analyzing engraftment following 1,061 single-unit UCB transplants in patients with hematological malignancies, including over 300 patients with highly comparable features to patients included in our trial in terms of cell dose range (2.5–4.9×107/kg), degree of HLA-mismatch (1–2 mismatches), and type of graft used (RCD), the median time of neutrophil engraftment was ∼28 days, with a cumulative incidence of engraftment of less than 80% at 100 days [26]. Notably, in this updated series, the median time to engraftment was not substantially improved despite inclusion of almost 500 additional patients who were treated more recently [26,30].
Double UCB units were employed in the series with cell doses reflect the combined cell dose of the 2 UCB units used.
MDS, myelodysplasia; HD, Hodgkin's disease; N/A, not available from publication; CI, confidence interval.
While DPP-4 inhibition might have had a positive impact on neutrophil engraftment, the effects on platelet recovery are less certain and will need further study. In at least 4 patients, time to recovery of platelets to >20×109/L was difficult to assess because of increased platelet consumption due to thrombotic microangiopathy (likely related to the use of sirolimus and tacrolimus for GvHD prophylaxis), and need for repeated transfusions for gastrointestinal bleeding. Better platelet engraftment kinetics may have become apparent in the absence of these complications.
A notable observation in our study is the very low incidence of GvHD. Only 1 of 17 patients receiving RCD grafts developed acute GvHD, and 1 of 11 evaluable patients developed chronic GvHD; frequencies much lower than previously reported even when ATG has been used [3,36,38]. Further studies with more patients are required to confirm this observation.
Seven patients receiving PD grafts in our study had worse engraftment and long-term outcome, likely related to very low CFU numbers following thawing and washing of these units; levels likely too low to properly test effects of DPP-4 inhibition on engraftment. The very low CFU numbers obtained from PD grafts may be related to our washing method used being suboptimal for these types of units [40].
While in vivo DPP-4 inhibition was feasible, improvement of this approach may be possible. We did not achieve the expected sustained inhibition of plasma DPP-4 activity as published in healthy volunteers (>90% plasma DPP-4 inhibition for 24 h) [21]. Importantly, plasma DPP-4 inhibition was significantly associated with engraftment indicating that plasma DPP-4 activity may be a good surrogate for bone marrow DPP-4 activity. The reasons for suboptimal DPP-4 inhibition remain unclear because sitagliptin pharmacokinetics were similar to those previously reported [21]. DPP-4 may be upregulated, or more enzyme released from a cellular pool [18] following cell death associated with myeloablative chemoradiotherapy in ways not previously appreciated. Sitagliptin given 2 or 3 times per day may result in more sustained DPP-4 inhibition, which may further improve engraftment kinetics. In addition, we recently showed that DPP-4 also regulates potency of granulocyte-macrophage colony stimulating factor, granulocyte-colony stimulating factor, interleukin-3, and erythropoietin, all of which have the truncation site for the enzyme, and inhibition or deletion of DPP-4 enhances cytokine activities and in vivo hematopoietic recovery after cytotoxic stress [18], suggesting longer administration of sitagliptin may further enhance engraftment.
Other strategies to overcome limitations of low cell dose and enhance engraftment have been suggested [41]. Transplantation of double UCB units has led to increased numbers of adults receiving transplants without evidence that engraftment is significantly enhanced compared with single UCB units [3,42]. Double UCB units significantly increase cost and demand on cord banks to collect more units. Direct intraosseous infusion has been investigated [43], although it remains unclear whether this improves engraftment, and the need for general anesthesia may be difficult for some patients. Although co-infusion of purified, mobilized haploidentical CD34 cells [5,6], and co-infusion of ex vivo Notch ligand-expanded UCB stem cells together with unmanipulated cord cells [4], may somewhat improve engraftment kinetics, these approaches are costly and may be prohibitive for some centers. Approaches that enhance homing, including ex vivo fucosylation [44], or treatment of UCB cells with prostaglandin E2 [45,46], may offer potential synergy with DPP-4 inhibition.
Our results indicate that systemic DPP-4 inhibition may be a reasonable strategy for enhancing engraftment of single-unit UCB transplants, and may offer advantages over other approaches in simplicity and affordability. Improved dosing of sitagliptin to achieve more sustained DPP-4 inhibition, and also for a longer duration to enhance effects on hematopoietic cytokines, may result in enhanced efficacy, and requires further clinical investigation in larger trials.
Footnotes
Acknowledgments
Parts of these studies were supported by grants from the V Foundation for Cancer Research (S.S.F.), and Public Service multi-PI R01HL112669 from the National Institutes of Health (NIH) of the United States (H.E.B. and S.S.F.). S.M.-G. was supported as a predoctoral student on an underrepresented minority grant GM079657 (H.E.B.) from the NIH. Pharmacoanalytical work was performed by the Clinical Pharmacology Analytical Core Laboratory of the Indiana University Melvin and Bren Simon Cancer Center and supported by Institutional grant P30 CA082709.
Author Disclosure Statement
H.E.B. is a founder of Cord: Use Family Cord Blood Bank and serves on the medical scientific advisory board of the Cord: Use Public Cord Blood Bank.