
Abstract
This study was designed to assess the safety and efficacy of human umbilical cord mesenchymal stem cells (UC-MSCs) in the treatment of rheumatoid arthritis (RA). In this ongoing cohort, 172 patients with active RA who had inadequate responses to traditional medication were enrolled. Patients were divided into two groups for different treatment: disease-modifying anti-rheumatic drugs (DMARDs) plus medium without UC-MSCs, or DMARDs plus UC-MSCs group (4×107 cells per time) via intravenous injection. Adverse events and the clinical information were recorded. Tests for serological markers to assess safety and disease activity were conducted. Serum levels of inflammatory chemokines/cytokines were measured, and lymphocyte subsets in peripheral blood were analyzed. No serious adverse effects were observed during or after infusion. The serum levels of tumor necrosis factor-alpha and interleukin-6 decreased after the first UC-MSCs treatment (P<0.05). The percentage of CD4+CD25+Foxp3+ regulatory T cells of peripheral blood was increased (P<0.05). The treatment induced a significant remission of disease according to the American College of Rheumatology improvement criteria, the 28-joint disease activity score, and the Health Assessment Questionnaire. The therapeutic effects maintained for 3–6 months without continuous administration, correlating with the increased percentage of regulatory T cells of peripheral blood. Repeated infusion after this period can enhance the therapeutic efficacy. In comparison, there were no such benefits observed in control group of DMARDS plus medium without UC-MSCs. Thus, our data indicate that treatment with DMARDs plus UC-MSCs may provide safe, significant, and persistent clinical benefits for patients with active RA.
Introduction
R
It has been reported that pro-inflammatory cytokines and chemokines play an essential role in RA [4]. Biological agents aiming at those cytokines have been tested clinically, such as recombinant human tumor necrosis factor (TNF) receptor-Fc fusion protein [5,6] and recombinant human interleukin (IL)-1 receptor antagonist [7]. However, there were moderate–severe side effects observed, including relapse and an increased susceptibility to infections [8]. Moreover, such symptomatic therapies were unable to promote the reconstruction of immune tolerance.
Mesenchymal stem cells (MSCs) are multipotent cells existing in many fetal [9] and adult tissues [10] that can replicate as undifferentiated cells and potentially differentiate to lineages of mesenchymal tissues [11]. MSCs can also modulate several immune functions through interplay with cells from both innate and adaptive immune systems. Furthermore, after administration in vivo, MSCs can migrate to injured tissues, where they can restrain the release of pro-inflammatory cytokines and facilitate the survival of damaged cells, and also induce peripheral tolerance [12]. Clinical studies have confirmed that MSCs have clinical benefits in severe acute graft-versus-host disease [13] and in different autoimmune diseases, such as systemic lupus erythematosus [14]. Previous studies found that MSCs may treat RA, and many mechanisms were explored [15 –17]. However, there were no comprehensive reports regarding the effects of umbilical cord (UC)-MSCs on patients with RA, who were with recurrent symptoms after long-term treatment with regular strategies in clinics.
We are conducting this cohort to evaluate the safety and efficacy of UC-MSCs in the treatment of RA, along with discovery of the possible mechanisms. Here, we demonstrated that (1) UC-MSCs treatment was safe without major side effects during and after infusion. (2) Treatment with disease-modifying anti-rheumatic drugs (DMARDs) plus UC-MSCs was more efficacious than DMARDs plus medium without UC-MSCs. (3) Continuous UC-MSCs treatment maintained clinical benefits. (4) Clinical benefits are likely resulting from anti-inflammation, immune-modulatory, and immune-tolerance induction.
Materials and Methods
Patients
According to the American Rheumatism Association's diagnostic criteria [18], RA patients were enrolled, and a written informed consent was provided in accordance with the Declaration of Helsinki. The study was registered in ClinicalTrials.gov (identifier: NCT01547091), approved by the ethics committee of 323 hospitals of the Chinese People's Liberation Army.
All patients' condition could not be well controlled by multiple traditional chemotherapies, including DMARDs, non-steroidal anti-inflammatory drugs (NSAIDs), and steroid and biological treatment. An inadequate response was defined as discontinuation of traditional medication therapy due to lack of effect and/or serious side effects. Patients should have active disease despite treatment with DMARDs at enrollment, defined as more than three painful joints, accompanied by joint swelling and tenderness and at least one of the following situations: erythrocyte sedimentation rate ≥45 mm/h, C-reactive protein (CRP) ≥of at least 15 mg/dL, or morning stiffness lasting for at least 1 h.
Treatment protocol
All patients continued to receive DMARDs: small doses of DMARDs individually: methotrexate at 7.5–10 mg/week, and/or leflunomide at 10 mg/day, and/or hydroxychloroquine at 200 mg/day. Con-comitant therapy with stable and proper doses of NSAIDs were permitted.
UC-MSCs were obtained from Alliancells Institute of Stem Cells and Translational Regenerative Medicine using the established protocol [19] and met the eligible criteria for clinical use [20]. Patients received either 4.0×107 of UC-MSCs in 40 mL stem cell solvent [21] as treatment, or 40 mL stem cell solvent without UC-MSCs as control, via intravenous infusion.
In detail, 172 RA patients were enrolled and allocated into two groups (Fig. 1). One group is DMARDs group (n=36, treated by DMARDs plus medium without UC-MSCs); another is DMARDs plus UC-MSCs group (n=136, treated by DMARDs plus UC-MSCs). Overall, 136 patients from the treatment group were enrolled from 2010, and 36 patients from the control group were enrolled since late 2012. Therefore, the control population was accessed at a time different from the treated population. However, all patients were enrolled and studied at the same institution, and were not a part of any other formal, randomized controlled trials. In addition, DMARDs plus UC-MSCs group was divided into three groups according to different intervals after the first treatment (Table 1). Group 1 has 76 patients for 3 months' interval; group 2 has 45 patients for 6 month's interval; and group 3 has 15 patients for more than 8 months' interval. In addition, 24 among 76 patients in group 1 were treated by UC-MSCs twice with 3 months' interval.

172 rheumatoid arthritis (RA) patients were enrolled and allocated into two groups. One group is DMARDs plus medium without UC-MSCs group (n=36). Another is DMARDs plus UC-MSCs group (n=136, treated by DMARDs plus UC-MSCs). In addition, DMARDs plus UC-MSCs group was divided into 3 groups according to different intervals after the first treatment: group 1 has 76 patients for 3 months' interval; group 2 has 45 patients for 6 months' interval; group 3 has 15 patients for over 8 months' interval.
UC-MSCs, umbilical cord mesenchymal stem cells; HAQ, the Health Assessment Questionnaire; DAS 28, the 28-joint disease activity score; DMARDs, disease-modifying antirheumatic drugs; NSAIDs, nonsteroidal anti-inflammatory drugs.
Safety evaluation was performed before and after UC-MSCs or medium without UC-MSCs administration by monitoring physical examination, liver and kidney function, chest radiography, and electrocardiograph. Standard hematological and biochemical tests and urine analysis were performed as well. Adverse events were recorded individually.
Assessment of disease status was composed of a complete count of tender and swollen joints [4], the 28-joint disease activity score (DAS28) [22], and the Health Assessment Questionnaire (HAQ) [23]. The other indices of disease activity included C-reactive protein, erythrocyte sedimentation rate, duration of morning stiffness, patient's and physician's global assessments, rheumatoid factor (RF) titers [4], and anti-cyclic citrullinated peptide antibody.
Study end points
The primary efficacy end points were the American College of Rheumatology (ACR) 20 and ACR50 responses [24] in disease activity at different time points. Other efficacy end points were ACR70 response, the DAS28, and the percentage changes from baseline in the HAQ.
T-regulatory cells detection and intracellular cytokine staining for Th1/Th2
Peripheral blood samples of RA patients were collected and analyzed with BD Multitest™ IMK kit. Regulatory T cells were stained with anti-CD4-fluorescein isothiocyanate, anti-CD25-Allophycocyanin, and anti-Foxp3-PE (eBioscience). Th1/Th2 test was carried out using Fast Immune Intracellular Cytokine Staining Procedure. Data were acquired and analyzed by FACS Caliber (Becton Dickinson).
Multiplex cytokine assay
A bead-based multiplex cytokine assay was custom designed for the quantification of the following cytokines: IL-1β, IL-4, IL-6, IL-10, IL-17A, TNF-α, interferon-γ (IFN-γ), regulated on activation, normal T cell expressed and secreted (RANTES), and transforming growth factor-β1 (TGF-β1). Assays were performed according to instructions and read with a Luminex 200 system (Millipore Corporation).
Statistical analysis
All continuous variables were subjected to descriptive statistics. Changes between baseline and end point were compared by the Wilcoxon signed-rank test. Rates of ACR response criteria were analyzed by logistic regression. Data for safety evaluation before and after the treatment were compared by paired t-test. All statistical tests were two sided, and the significance level was set as P<0.05. All analyses were conducted by SPSS 17.0 (SPSS, Inc).
Results
Safety evaluation
No patients showed acute serious side-effects either during or after UC-MSCs infusion, and there were six cases of 136 patients (4%) showing mild adverse effects during the infusion, such as chill and/or fever (<38.5°C), which disappeared within 2 h without any treatment.
Overall, 26 cases of 87 individuals (30%) presenting anemia with average hemoglobin level of 99 g/L returned to normal after UC-MSC treatment. Levels of serum total protein and globulin were decreased (from 71 to 69 g/L and from 32 to 29 g/L, on average, respectively, Table 2), which were consistent with the lessened titers of rheumatoid factor and anti-cyclic citrullinated peptide antibody. No major abnormal findings in hematologic or serum chemical profiles were found in the study. In addition, clinical profiles between DMARDs plus medium without UC-MSCs group as controls (n=36) and DMARDs plus UC-MSCs group (n=58) were shown in Table 3, indicating a similar baseline between two groups before the treatment. DMARDs plus UC-MSCs showed decreased levels of total protein and globulin and increased levels of albumin and hemoglobin compared with the control group. The increased levels of albumin and hemoglobin may be related to the improved liver function and the decreased incidence of gastro-intestinal tract bleeding. In addition, there are no significant differences in the percentage of B cells between before and after UC-MSCs administration in Supplementary Fig. S1 (Supplementary Data are available online at
Value: Mean±SD, t-test, *
P<0.05,
Value: mean±SD, t-test, *
P<0.05,
DMARDs plus medium without UC-MSCs: n=36; DMARDs plus UC-MSCs: n=58.
Efficacy determination
Changes of symptoms
All patients have shown improvements in the diet, sleep, and physical strength as early as 2 weeks after the cell therapy based on patients' reports. In comparison, there was no such improvement in the control group. In addition, the clinical response to UC-MSCs treatment was rapid with the physical evidence after administration of UC-MSCs. The joint pain and swelling were alleviated within 12 h, and was maintained through the period of the study.
Clinical benefits before and after the treatments
Three months after DMARDs plus UC-MSCs treatment, significantly decreased levels of HAQ and DAS28 scores were observed, indicating an improvement of clinical behaviors. Further tests showed a decreased level of CRP and RF and increased levels of the percentage of CD4+CD25+Foxp3+ regulatory T cells (Fig. 2A–E). In comparison, there was no significant change in the scores of HAQ and DAS28 in the control group with DMARDs plus medium without UC-MSCs. In parallel, DMARDS did not alter serum levels of CRP, RF, and percentage of CD4+CD25+Foxp3+ regulatory T cells in peripheral blood (Fig. 2A–E).

Scores of Health Assessment Questionnaire (HAQ), the 28-joint disease activity score (DAS28), CRP, RF, and regulatory T cells before and after 3-month treatment between disease-modifying anti-rheumatic drugs (DMARDs) plus medium without umbilical cord mesenchymal stem cells (UC-MSCs) and DMARDs plus UC-MSCs groups.
Data from Fig. 2 provided the core message that DMARDs plus UC-MSCs showed encouraging clinical benefits in the treatment with refractory RA resulting from a decreased level of systemic inflammation and an increased level of immune tolerance.
The scores of HAQ and DAS28 showed a steady reduction with continuous and repeated treatments (twice with 3 months' interval) (Fig. 3A, B). The number of joints with tenderness and swelling was significantly reduced along with the alleviated symptoms. After two cycles of treatment, 58% (14 in 24) patients achieved ACR20, 13% (3 in 24) achieved ACR50, and 13% (3 in 24) patients achieved ACR70, respectively.

Scores of HAQ and DAS28 were evaluated after twice of UC-MSCs treatment.
In addition, the DMARDs plus UC-MSCs group was divided into three sub-groups according to different intervals after the first treatment (Group 1 has 76 patients for 3 months' interval; group 2 has 45 patients for 6 months' interval; and group 3 has 15 patients for more than 8 months' interval). HAQ Score, DAS28 Score, and ACR were re-analyzed among three groups. We observed a reduced level of HAQ in three groups. However, there was no statistical difference in group 3 (Fig. 4A). A significant decrease of DAS28 was observed in three groups (Fig. 4B). In detail, 50% (38 in 76) of patients achieved remission and 25% (19 in 76) stayed in a low-active period in group 1; 49% of patients (22 in 45) achieved remission and 38% (17 in 45) stayed in a low-active period in group 2; and 53% (8 in 15) of patients achieved remission with 27% (4 in 15) staying in group 3. To further assess the therapeutical consequences, ACR data were further analyzed as shown in Fig. 4C. In detail, 36% (27 in 76) patients achieved ACR20, 28% (21 in 76) achieved ACR50, and 12% (9 in 76) patients achieved ACR70 in group 1. In comparison, only 14% patients (5 in 36) achieved ACR20 in DMARDs plus medium without UC-MSCs group (data not shown). In group 2, 47% (21 in 45) patients achieved ACR20, 20% (9 in 45) achieved ACR50, and 4% (2 in 45) patients achieved ACR70; in group 3, 33% (5 in 15) patients achieved ACR20, 7% (1 in 15) achieved ACR50, and 7% (1 in 15) patients achieved ACR70.
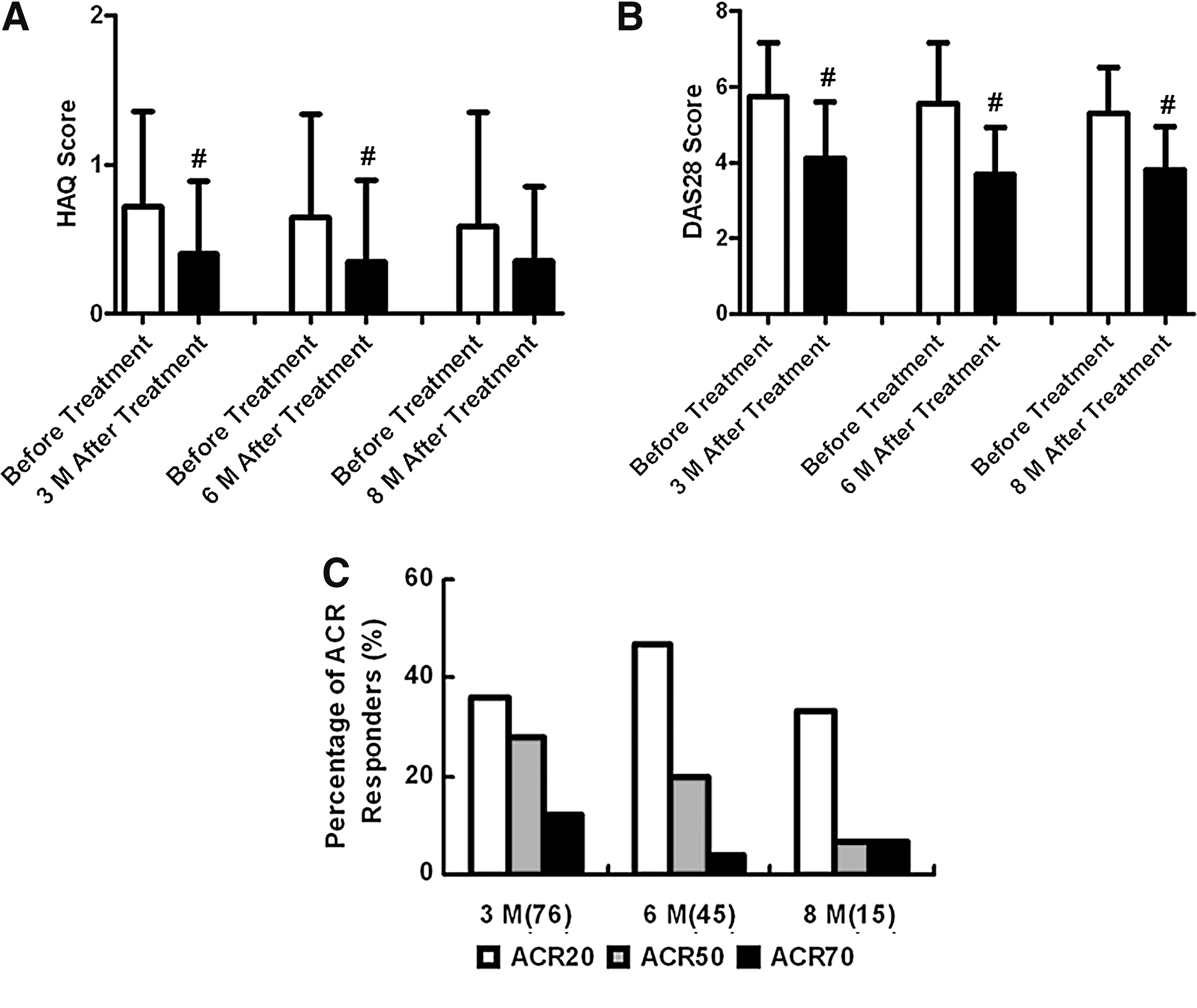
Scores of HAQ, DAS28, and American College of Rheumatology (ACR)20, 50, and 70 response rates at three groups in DMARDs plus UC-MSCs group, respectively.
Potential mechanisms
It has been well documented that anti-inflammation is an important mechanism in the treatment of autoimmune diseases. Level of CRP, a maker of inflammation, was decreased after the treatment in Fig. 5A. In addition, levels of pro-inflammatory cytokines, such as IL-6 and TNF-α, were tested as shown in Fig. 6. Compared with the level from normal donors, patients with RA showed increased levels of IL-6 and TNF-α. One time of UC-MSCs administration induced reduced levels of two pro-inflammatory factors (Fig. 6A, B). Another marker, RF, also showed a decreased trend, particularly at 3 months after the treatment (Fig. 5B). Information from Figs. 5, 6 indicated that UC-MSCs might clear up circulating inflammatory and other rheumatoid-related factors. To further support this notion, cytokine levels of peripheral blood mononuclear were measured in Supplementary Fig. S2. The data indicated that UC-MSCs significantly reduced levels of TNF-α and IL-6.
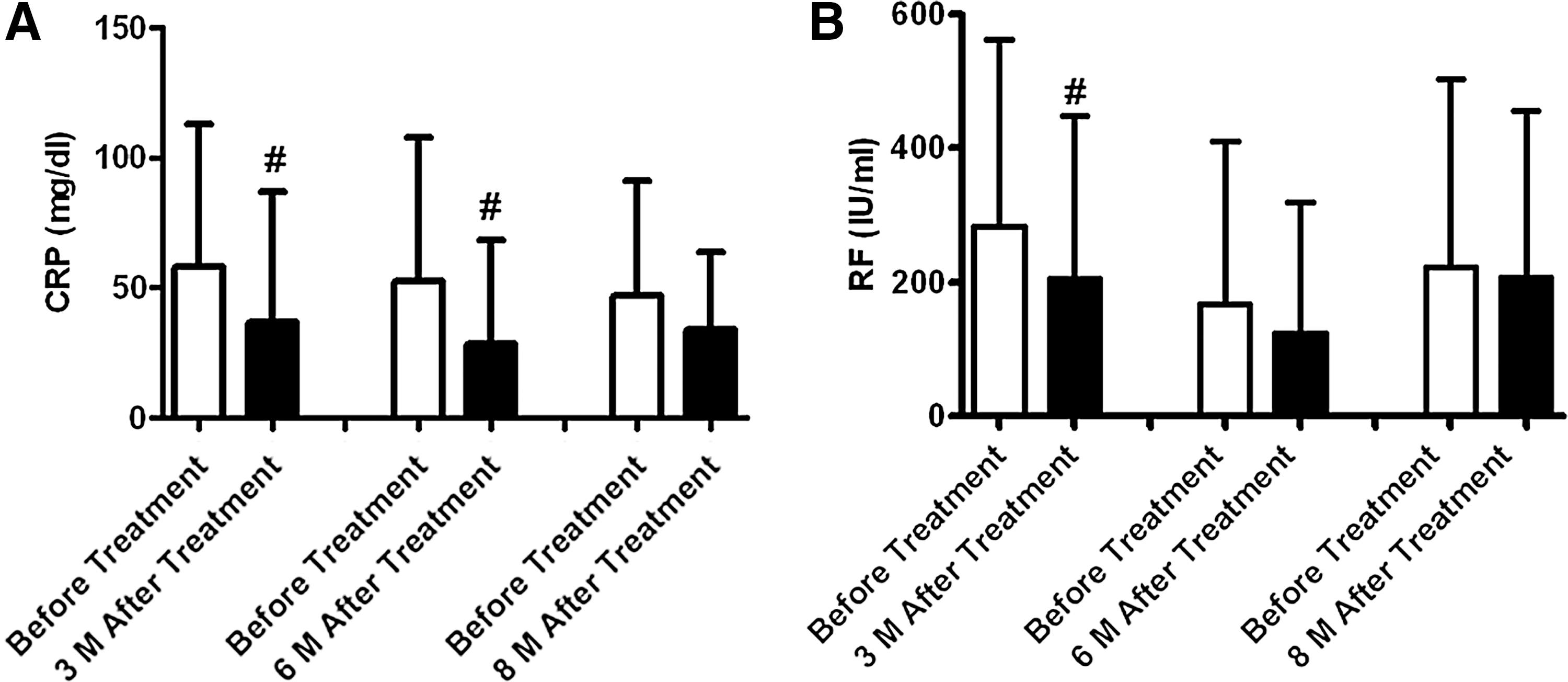
CRP and RF levels were measured at three groups in DMARDs plus UC-MSCs group, respectively.
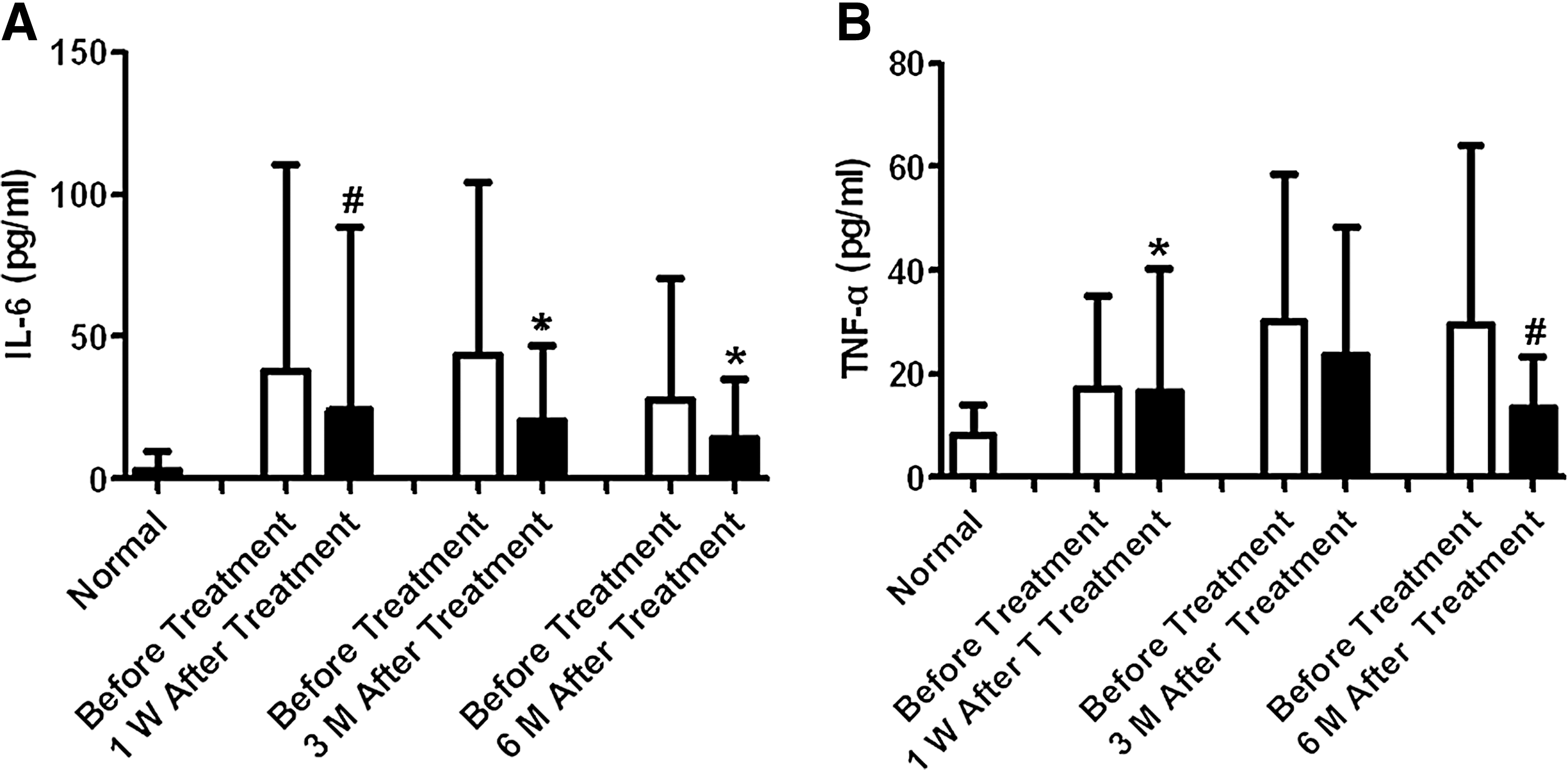
Cytokine milieu of the serum from patients with RA was measured at 1 week, 3 months, and 6 months in DMARDs plus the UC-MSCs group respectively.
Although there were no significant changes in the percentages of CD3+ cells, CD4+ cells, and CD8+ cells before and after treatment (data not shown), the percentage of CD4+CD25+Foxp3+ regulatory T cells in peripheral blood was significantly increased after DMARDs plus UC-MSCs treatment (by 25% in 3 months, by 34% in 6 months, and by 14% in 8 months) in Fig. 7A, and repeated infusion maintained this level (from 3.78% to 5.12%, then to 5.81% in Fig. 7B). In addition, the change of regulatory T cells was found to be associated with the clinical benefits, indicating that the patients showing higher levels of regulatory T cells after UC-MSCs treatment may achieve better clinical benefits (Fig. 7C). Furthermore, the level of IL-4 was increased, which was inconsistent with the decreased ratio of Th1/Th2 cells (Fig. 7D).

Percentage of CD4+CD25+Foxp3+ regulatory T cells to total CD4+ T cells in peripheral blood, the relationship between changes of ACR response and regulatory T-cells percentage, and Th1 and Th2-type responses measuring by IFN
Discussion
The core message from the current study is that DMARDs plus UC-MSCs administration was safe and effective in reducing disease activity for a long period in patients with refractory RA than controls receiving DMARDs plus medium without UC-MSCs. No major toxicities were observed during and after UC-MSCs administration. In UC-MSCs group, evidence of clinical benefits was obtained, and the improvements of clinical manifestations were likely related to the decreased expression levels of various inflammatory cytokines and chemokines, the increased percentage of regulatory T cells in peripheral blood, and the up-regulated IL-4-producing Th2 cells, suggesting that anti-inflammation along with the improved immune-modulation and the induced immune-tolerance are likely to be major potential mechanisms.
RA, the pathogenesis of which is still unclear, can not only lead to joint deterioration, but also cause damage to multiple tissues and organs [1]. Joint damage cannot be repaired by the traditional medications that have been used to treat RA patients for many years despite their obvious and unavoidable side effects [5]. Most of those patients got a relapse and progressed after a certain period of disease stability. Thus, it is critical and necessary to find a new method to improve the therapeutic outcomes.
A large number of active cytokines, such as TNF-α [25], IL-1 [26], and IL-6 [27], have been found in the joints of RA patients, which may influence the disease processes and result in articular damages and the co-morbidities of RA [28]. In recent decades, targeted therapy has been developed; for instance, the etanercept (TNF-α competitive inhibitor) [5] and infliximab (TNF-α monoclonal antibodies) [29] were used to treat RA patients. However, Giles et al. [30] found that TNF-α inhibitor could make patients more susceptible to surgical infections without exerting a positive effect on joint repair, and cessation of therapy may increase the disease activity [6].
MSCs have been reported to have the capacity of modulating immune responses and healing damaged tissues and organs. Previous studies [15 –17,31] have found that MSCs could be a new effective therapeutic approach for autoimmune arthritis [17]. However, MSCs from RA patients could not maintain high clonogenic potential and proliferative capacity as normal MSCs [32], making allogenic MSCs as a possible way to help defective self-MSCs to achieve clinical benefits. With distinct advantages of UC-MSCs, including accessibility, higher proliferation capacity, and lower immunogenicity [19] when compared with bone marrow-derived MSCs, UC-MSCs were chosen in this clinical trial.
UC-MSCs were well tolerated as described in previous reports [33] by showing no anaphylaxis and no severe gastrointestinal side effects. In our study, no major abnormalities were observed in serum chemical profiles, including liver and kidney functions during or after the UC-MSCs treatment, revealing that UC-MSCs infusion was safe and feasible to treat active RA.
Rapid clinical response to UC-MSCs treatment was also noticed in this trial. The joint pain, swelling, and stiffness in patients were relieved within 12 h post-treatment. The possible mechanism may be that MSCs can cause chemotaxis to the damaged organ rapidly and accumulate there [34 –37], subsequently secrete several soluble immunosuppressive factors constitutively, and express a variety of receptors for inflammatory factors under the state of inflammation [12]. In the UC-MSCs group, the disease activity was reduced significantly assessing by DAS28 compared with the condition before treatment. Moreover, clinical utility was defined by ACR20 response, and the higher magnitude responses (ACR50 and ACR70) appeared after the first treatment. In addition, the hematology profiles returned to normal level and autoantibodies titers also declined. We further observed that UC-MSCs treatment increased the patients' compliance to DMARDs by alleviating the side effects of these drugs. The second cycle of treatment resulted in better clinical benefits and improved the quality of life more obviously for RA. These data suggested that RA patients, showing refractory to traditional treatments, may achieve significant improvements after UC-MSCs treatment. It was inferred that the response rate of MSCs was not related to the donor the human leukocyte antigen (HLA)-match. It has been proved that the response rate of MSCs for treatment of steroid-resistant, severe, acute graft-versus-host disease was not related to the donor HLA-match [33]. They have investigated immune responses to allogeneic MSC infused into hematopoietic stem cell transplantation (HSCT) recipients. The recipients given MSCs showed no response to infused MSCs before and approximately 6 months after infusion, the infused MSCs are only weakly immunogenic in humans and validate the clinical use of MSCs from HLA-mismatched donors. It has been shown that patients infused with MSCs that are HLA haploidentical or completely HLA mismatched with the stem cell donor and recipient show no immunological memory to the infused MSCs [38]. Undifferentiated and differentiated MSCs do not elicit allo-reactive lymphocyte proliferative responses and modulate immune responses. So, MSCs can be transplantable between HLA-incompatible individuals [39].
It was known that the cytokines arising from numerous synovial cells were central to RA pathogenesis [1], and MSCs can express various receptors for inflammatory factors [40] which might combine with the corresponding inflammatory factors to reduce inflammation in RA patients. Immunoregulatory role of MSCs may associate with the occurrence of inflammatory mediators [41]. In this study, the serum levels of TNF-α and IL-6 significantly decreased in parallel with the deduction of serum C-reactive protein after treatment, indicating that anti-inflammation was one of the major mechanisms of MSCs. Furthermore, MSCs were recently reported to suppress effector T cells and inflammatory responses and have emerged as attractive therapeutic candidates for immune disorders [16]. UC-MSCs administration in this study significantly increased IL-4 expression secreted by Th2 cells and the percentage of CD4+CD25+Foxp3+ regulatory T cells in peripheral blood. The increased level of regulatory T cells was positively correlated with the improvement of disease status, especially the ACR responses, which enabled the level of regulatory T cells to be one of the important clinical indices for the evaluation of the efficacy of UC-MSCs treatment [17]. In addition, MSCs might provide a multitude of trophic factors with various properties, thereby reducing tissue injury, protecting tissue from further degradation, and thus enhancing tissue repair [42].
This is the first investigation of the safety and efficiency of UC-MSCs in the treatment of RA patients. However, there is one limitation of the current study: All patients were recruited and treated from a single center. Therefore, a larger multiple-center study will be necessary to further confirm current findings. In addition, relevant joint imaging data before and after MSC infusion should be collected and analyzed. In spite of these, this study was also valuable, as all patients were from the failed traditional medication treatment and obtained significant improvements, including symptom alleviation and cytokines decrease, after UC-MSCs treatment.
Overall, our study confirmed the safety and efficacy of UC-MSCs infusion in active RA patients. The therapeutic effects can be maintained for at least 3 months, and repetitive treatment would stabilize the clinical outcomes and improve the patients' quality of life, which was significantly correlated with the increased percentage of regulatory T cells in peripheral blood. Thus, UC-MSCs are suitable applications in the clinic and provide an additional choice to many RA patients.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (30872618), 973 Program (no. 2013CB967101) of the Ministry of Science and Technology of China, State High-tech Research and Development Plans (2011AA020103, 2011AA020109), the Shaanxi Province Social Development Public Relations Project (2012K13-02-35), Key Sciences and Technology Project in Hainan Province (ZDZX2013003-2), and the Military Medicine and Public Health Plan (CLZ120GA23).
The authors thank Professor Sir Martin John Evans (University of Cardiff, UK) for kindly revising this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.