
Abstract
We have recently demonstrated that heterologous transplantation of horse amniotic membrane-derived mesenchymal cells (AMCs) can be useful for cell therapy applications in tendon diseases, and hypothesized that these cells may promote tendon repair via paracrine-acting molecules targeting inflammatory processes. To test this hypothesis, here we examined the immunomodulatory characteristics of AMCs and of their conditioned medium (AMC-CM) in vitro, and studied the potential therapeutic effect of AMC-CM in thirteen different spontaneous horse tendon and ligament injuries in vivo. Our results demonstrate that AMCs are capable of inhibiting peripheral blood mononuclear cell (PBMC) proliferation after allogenic stimulation either when cocultured in cell-to-cell contact, or when the two cell types are physically separated by a transwell membrane, suggesting that soluble factors are implicated in this phenomenon. Our hypothesis is further supported by the demonstration that PBMC proliferation is inhibited by AMC-CM. In our in vivo studies, no significant adverse effects were observed in treated tendons, and clinical and ultrasonographical evaluation did not reveal evidence of inappropriate tissue or tumor formation. Clinical outcomes were favorable and the significantly lower rate (15.38%) of reinjuries observed compared to untreated animals, suggests that treatment with AMC-CM is very efficacious. In conclusion, this study identifies AMC-CM as a novel therapeutic biological cell-free product for treating horse tendon and ligament diseases.
Introduction
T
In addition, recent studies have suggested an immunomodulatory role of implanted stem cells. Animal model studies have demonstrated that MSCs are hypo-immunogenic and inhibit the activation of T and B lymphocytes and natural killer cells [20 –22]. The precise mechanism of this effect is largely unknown. We hypothesized that the beneficial effects observed with transplantation of AMCs to promote horse tendon repair [10,11] could be also mediated via AMC-secreted paracrine-acting molecules and by their immunomodulatory properties. For these reasons, the aims of the present study were to evaluate the immunomodulatory capacity of horse amniotic membrane-derived cells and of the conditioned medium derived from the culture of these cells, and to investigate the effects of injecting the conditioned medium derived from AMCs (AMC-CM) in spontaneous horse tendon and ligament injuries in vivo.
Materials and Methods
Amniotic membrane collection and isolation
Allanto-amniotic membranes were obtained at term of normal pregnancies from three mares. Samples of allanto-amnion were placed at 4°C in calcium- and magnesium-free phosphate-buffered saline (Euroclone, Milan, Italy) supplemented with 4 μg/mL amphotericin (Euroclone), 100 UI/mL penicillin–100 μg/mL streptomycin (Euroclone), and were processed within 12 h of collection. The amniotic membrane was mechanically separated from the allantois. Isolation of AMCs was performed as reported by Lange-Consiglio et al. [10].
Cell culture and expansion
AMCs were cultured in the high-glucose Dulbecco's modified Eagle's medium (DMEM; Euroclone) supplemented with 10% fetal bovine serum (Sigma-Aldrich, Milan, Italy), 10 ng/mL epidermal growth factor (Sigma-Aldrich), 100 UI/mL penicillin–100 μg/mL streptomycin, 0.25 μg/mL amphotericin B, and 2 mM L-glutamine (Sigma-Aldrich) (standard medium) at a density of 1×105 cells/cm2 in T75 culture flasks (Euroclone). The flasks were incubated at 38.5°C with 5% CO2 and 90% humidity. The medium was replaced after 72 h for the first time to remove nonadherent cells, and was subsequently replaced twice weekly until cells reached approximately 80% confluence. Cells were then detached with 0.05% trypsin-EDTA (Euroclone), counted, and redistributed into new culture flasks to maintain and expand the culture for three passages (P). At this passage, the cells were used to prepare the CM or were cryopreserved in liquid nitrogen, using standard cryopreservation protocols, for lymphocyte proliferation studies. Molecular biology analyses at P3 showed that these cells display a typical mesenchymal stromal phenotype, with the expression of markers such as CD29, CD44, CD106, CD105, and MHCI, but not of CD34 and MHCII, as reported by Lange-Consiglio et al. [10].
For experimental use, cryopreserved AMCs were thawed quickly in a 37°C water bath, washed with the Roswell Park Memorial Institute medium (RPMI) complete, centrifuged, plated in the RPMI, and expanded at 37°C, 5% CO2.
Preparation of AMC-CM
AMCs at P3 were plated in 24-well plates (Euroclone) at a density of 1×105 cells/mL/well in the DMEM standard medium.
To generate AMC-CM, cells were cultured for 5 days at 37°C in a humidified atmosphere of 5% CO2. Supernatants from each plate were then collected, pooled, centrifuged at 700 g, filtered (0.2 μm) to remove cellular debris, and stored at −80°C. This procedure was performed for cells obtained from three different placentas.
For the in vitro lymphocyte proliferation test described below, the AMC-CM was utilized after thawing. For the in vivo experiments, all of the collected supernatants were lyophilized and stored at 4°C until use, at which point, they were dissolved in sterile water to one-quarter of the initial volume. The control, nonconditioned medium (non-CM) was generated in the same way as above, except that no cells were cultured in the plates.
Peripheral blood mononuclear cell isolation
Horse peripheral blood mononuclear cells (PBMCs) were obtained from heparinized whole blood samples, after informed consent was obtained from the owners, using density gradient centrifugation (Lymphoprep; Axis-Shield, Oslo, Norway) at 500 g without brakes for 20 min at room temperature.
Lymphocyte proliferation test
Lymphocyte proliferation was induced by stimulating PBMCs (2×105 horse PBMC/well in a 96-well flat bottomed-plate) through the addition of phytohemagglutinin (PHA; Sigma-Aldrich) at a final concentration of 2 μg/mL in a final volume of 200 μL/well of the RPMI complete medium.
To study the effects of AMCs on T lymphocyte proliferation in a cell–cell contact setting, different amounts of cultured AMCs (2×105, 1×105, 0.5×105, 0.25×105) were plated in the RPMI complete medium and left to adhere overnight. The next day, AMCs were γ-irradiated (3,000 cGy), and 2×105 activated PBMCs were added to each well, obtaining PBMC:AMC ratios of 1:1, 1:0.5, 1:0.25, and 1:0.125. AMCs were irradiated to ensure that any proliferation observed could be attributed solely to the proliferation of responder lymphocytes. PBMCs without AMCs were used as controls. All cultures were carried out in triplicate, using flat-bottomed 96-well tissue culture plates (Corning-Celbio, Milano, Italy), in a final volume of 200 μL of the RPMI complete medium.
For lymphocyte proliferation tests with segregated AMCs, transwell chambers with 0.4-μm pore size membranes (Corning-Celbio) were used to physically separate the lymphocytes from the AMCs. Different amounts of cultured AMCs (2×105, 1×105, 0.5×105, 0.25×105) were plated in the RPMI complete medium in the upper chambers of the transwell inserts. The next day, 2×105 activated PBMCs were added to each lower chamber, obtaining PBMC:AMC ratios of 1:1, 1:0.5, 1:0.25, and 1:0.125.
Lymphocyte proliferation tests were also performed in the presence of supernatants collected from AMCs, which had been cultured for 5 days (AMC-CM). To evaluate the effect of AMC-CM, different amounts (50 or 100 μL/well) of AMC-CM or control medium (non-CM), were added to activate the PBMCs.
In all cases, lymphocyte proliferation was assessed after 3 days of culture by adding 0.67 μCi per well (96-well tissue culture plates) of [3H]-thymidine (INC Biomedicals, Milano, Italy) for 16–18 h. Cells were then harvested with a Filtermate Harvester (PerkinElmer, Waltham, MA), and thymidine incorporation was measured using a microplate scintillation and luminescence counter (Top Count NXT; PerkinElmer).
Experimental groups and AMC-CM injection in vivo
Thirteen privately owned sport horses suffering from different types of tendon or ligament injuries were referred for orthopedic evaluation to the private practitioner coauthoring this study. A complete clinical examination was performed and all imaging modalities necessary to diagnose and document the emerging lesions were considered. Ultrasonographic examination (US) (Medison Sonovet Pico, GE Logiq e) was performed by the same practitioner. As a routine, all affected tendons or ligaments were US evaluated in both transverse and longitudinal scans and fully documented. The lesions were graded according to six categories of quantitative assessment as described by Rantanen [23]. All horses included in the study, except for case 1, had new, unilateral, acute injuries and an ultrasound-detectable hypoechoic lesion. Only lesions graded from 4 to 6 were included in this study. The characteristics of the horses' injuries are reported in Table 1. Case 1 had already sustained a core lesion in the superficial digital flexor tendon (SDFT) 8 months before the time of this study. Intralesional platelet-rich plasma (PRP) was reported for this animal, and the reinjury occurred in the early phase of retraining.
SI, sella italiano; KWPN, Koninklijk Warmbloed Paardenstamboek Nederland; PRE, pure spanish horse; BWP, Belgian Warmblood; Ara, Arabian; Hannov, Hannover; SJ, show jumping; LF, left front; LH, left hind; RF, right front; RH, right hind; G, gelding; F, female; M, male; SDFT, superficial digital flexor tendon; SL, suspensory ligament; OSL, oblique sesamoidian ligament; DIP, distal interphalangeal joint; metac, metacarpal; DS, digital sheath.
Permission from the University Bioethics Committee n.9.12/11, as well as written consent from the owners, were both obtained to allow evaluation of the ability of AMC-CM to exert beneficial effects in vivo. Considering that the AMC-CM was concentrated fourfold after lyophilization, and also taking into account the need for a uniform treatment protocol, an amount of two milliliters of AMC-CM was decided on as a standard experimental volume. This fixed amount, injected under ultrasonographic guidance into damaged tendons or ligaments, was chosen based on the average dimension of similar lesions in which, two milliliters are usually sufficient to load the lesion, as observed by the authors' previous experiences.
The interval between lesion/implantation ranged from 8 to 30 days. Three horses were used as controls, whereby non-CM was injected intralesionally with the same technique. Hair was clipped with a No. 40 blade. Routine aseptic surgical preparation was performed with a chlorhexidine scrub and alcohol. A local anesthetic ring block (2% Mepivacaine, Galenica Senese, Italy) proximal to the injection site and mild sedation with Detomidine (Pfizer Italia, Latina, Italy) were the only restraints used. The SDFT lesions were injected using a longitudinal technique (preferred in these cases by the operator) with a 20-gauge, 70-mm needle, in a proximal–distal direction. All of the other lesions were injected transversely using a 21-gauge, 40-mm needle, inserted laterally. A sterile bandage was applied and maintained for 48 h, during which, the horses were box rested. They were then allowed to undergo hand walking exercise for 15 min/day over 15 days and 30 min/day for a further 15 days. No nonsteroidal anti-inflammatory drugs (NSAIDs) or antibiotics were given, based on the aseptic technique.
In case 11, the distal insertion of the collateral ligament of the distal interphalangeal joint (DIP) was injected with the assistance of a radiographic guided technique, as described by Werpy [24] (Fig. 1). The whole coronary band and pastern was clipped and sterile surgical preparation of the area was performed. A proximal digital nerve analgesia (3 mL of 2% Mepivacaine per site) applied to the abaxial sesamoid was considered mandatory, as well as sedation with Detomidine (0.01 mg/kg), to avoid any reaction of the horse during needle placement. A 19G 70-mm spinal needle was inserted and directed toward the collateral fossa of the distal phalanx, with fine tuning and confirmation achieved with multiple different views taken with a portable digital radiography system (Cuattro DR Equine), until the needle tip appeared to be in an ideal position before injection. A Robert Jones bandage was applied and maintained for up to 3 weeks, during which the horse was box rested, and then allowed to be hand walked.
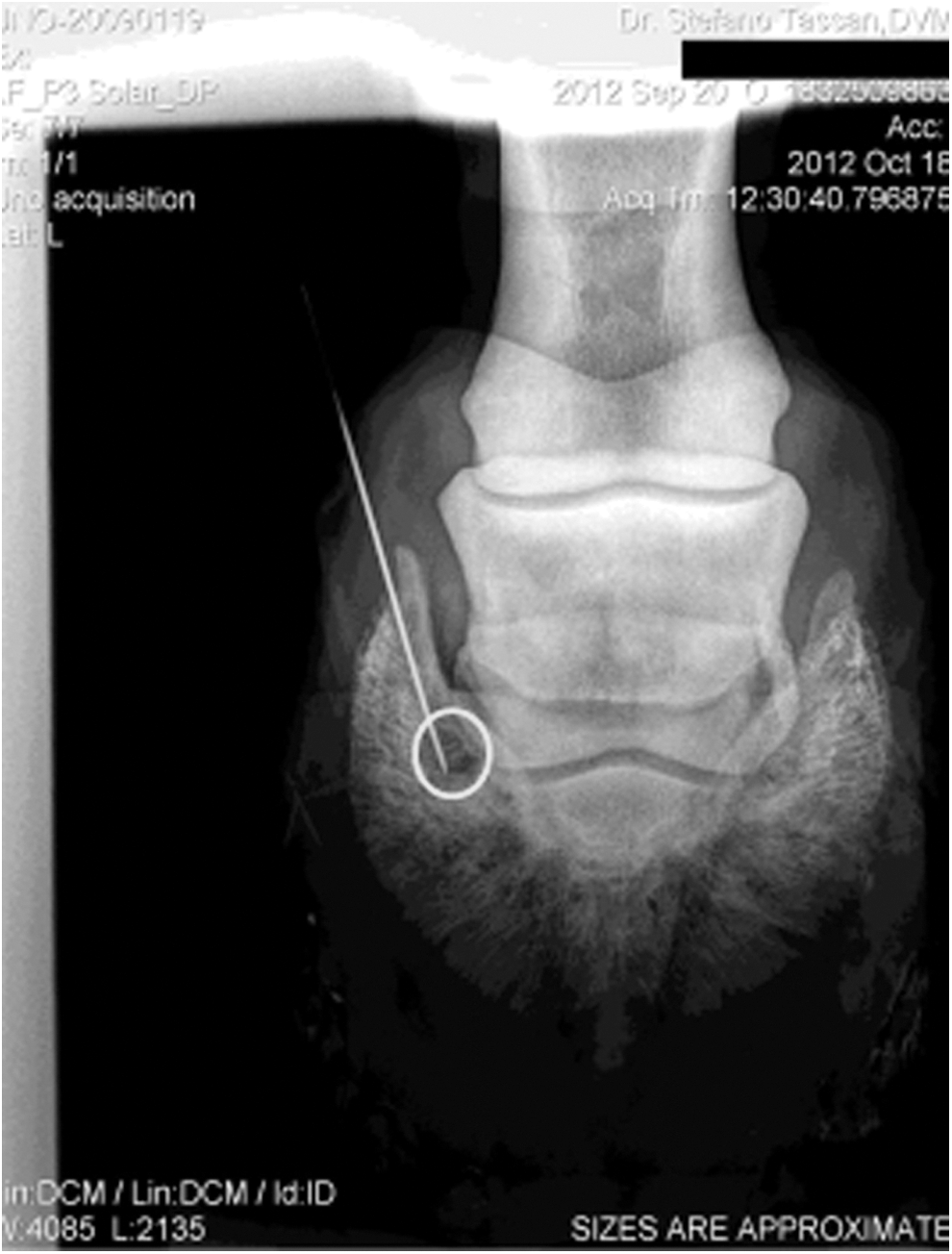
Distal enthesopathy of the DIP collateral ligament in patient 11. Radiographic guidance of the tip of the needle targeting the osteolytic area (visualized by the circle) induced by enthesopathy of the DIP collateral ligament at its insertion on the distal phalanx. AMC-CM injection is correctly achieved. AMC-CM, conditioned medium derived from amniotic membrane-derived mesenchymal cell; DIP, distal interphalangeal joint.
All horses were examined clinically and ultrasonographically at approximate monthly intervals after treatment, during convalescence and rehabilitation up to 12 to 15 months. The individual exercise program was fine tuned depending on US healing. Follow-up information was obtained from retraining until 2 years thereafter, or sooner, if a reinjury occurred.
Statistical analysis
Data are expressed as mean±SD. The Student's t-test was use to assess differences between groups. Differences were considered statistically significant for P values<0.05.
Results
Effect of AMCs and AMC-CM on PBMC proliferation in vitro
Through in vitro studies, we demonstrated that AMCs could inhibit PBMC proliferation after activation with PHA, both when the two cell types were cultured in direct contact and also when they were physically separated by a transwell system (Fig. 2). The inhibitory effect was dose dependent, and the higher effects were observed at a ratio of responder cells: AMCs of 1:1, both in the cell to cell contact and transwell experiments. These data suggest that cell contact was not required for the inhibitory action of AMCs, and that secreted molecules were responsible for the anti-proliferative effects observed.
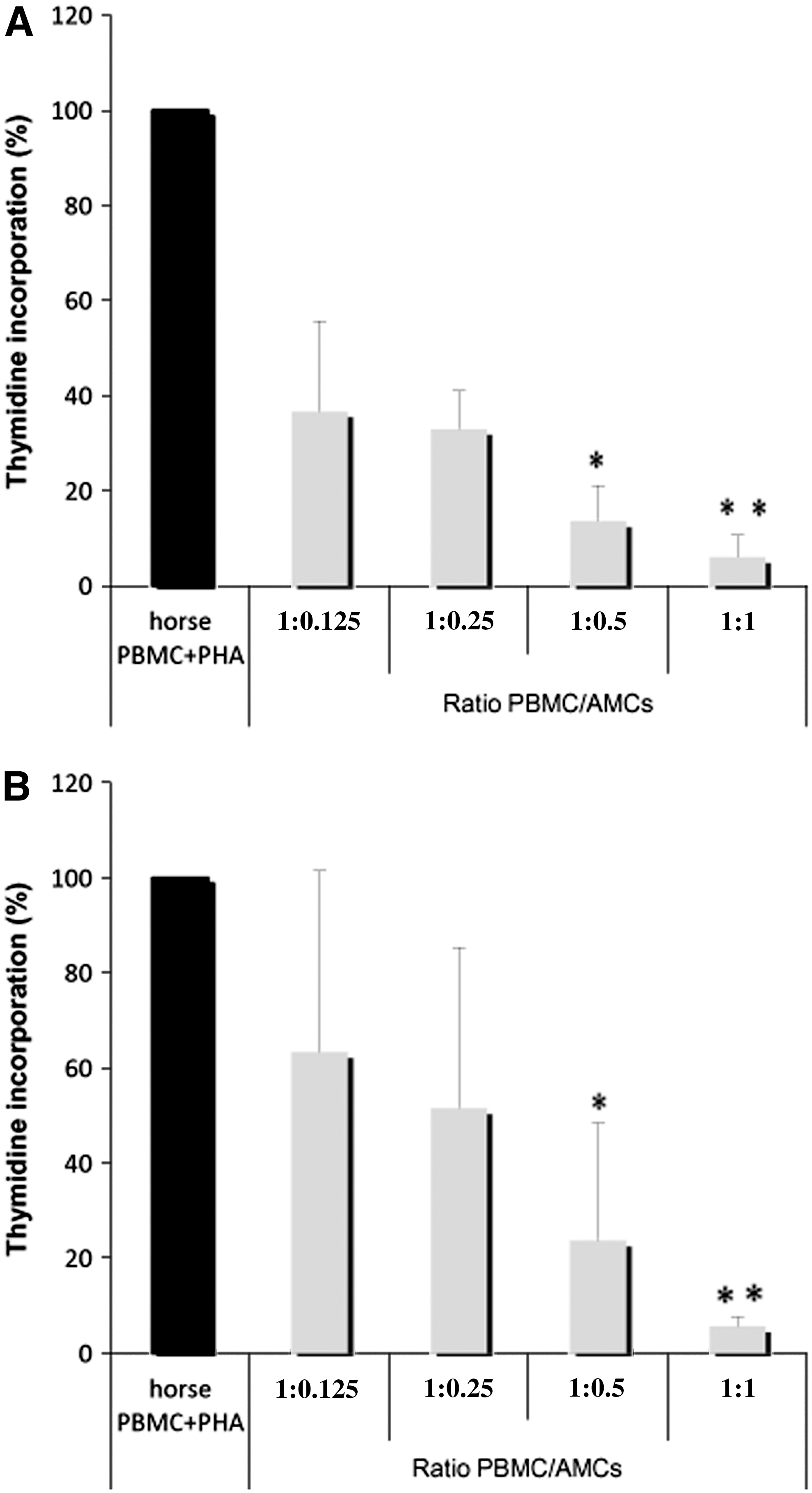
Effects of differing amounts of amniotic mesenchymal cells (gray bars), either in contact
This was confirmed by the observation that AMC-CM produced at passage 3 possessed the ability to inhibit PHA-stimulated T lymphocyte proliferation in a dose-dependent manner. On the contrary, the control media, no-CM, did not shown any antiproliferative effect (Fig. 3).

Effects of different amounts (50–100 μL) of control medium or the CM derived from AMC culture on the proliferation of PHA-stimulated lymphocytes (PBMC+PHA). Data represent the mean and SD of at least three independent experiments. ***P<0.001 versus PBMC+PHA.
In vivo tendon and ligament repair
Details regarding the horses enrolled in this study are displayed in Table 1. Anatomically specific lesion analysis included 5 SDFT, 7 suspensory ligaments (SL) (five branches: SLB, and two body), and 1 collateral ligament of the DIP.
Follow-up records were available for all of the treated horses. All intralesional procedures were well-tolerated and no adverse reactions to the AMC-CM injections occurred, with no soreness or flares noticed thereafter. Patients were able to walk easily straight after the procedure and no NSAID requirement could be objectively assessed, thereby confirming horses' welfare. Furthermore, no perioperative antibiotics were given, considering the sterility of the preparations administered and the aseptic technique used. An obvious improvement in lesional ecogenicity, which is often unusual if compared to other regenerative techniques, could always be observed at day 30 (Fig. 4A–C). Despite the limited number of cases, no abnormal tissue evolution could be detected at any time postinjection. The absence of fibrotic, metaplastic, or mineralized islands in the treated area is considered a safety characteristic. Healing-related neovascularization, which could not be observed before treatment (case 6), was variably, but consistently documented and detected in the affected area in the early stages during series of US with power doppler imaging. Neovascularization extension and intensity decreased and finally disappeared as the healing process progressed, confirming that this was associated with the treatment. It is noteworthy that this neovascularization was observed to last longer than ultrasonographic healing, and this finding was thus considered to be a key point to allow training to resume (Fig. 5).
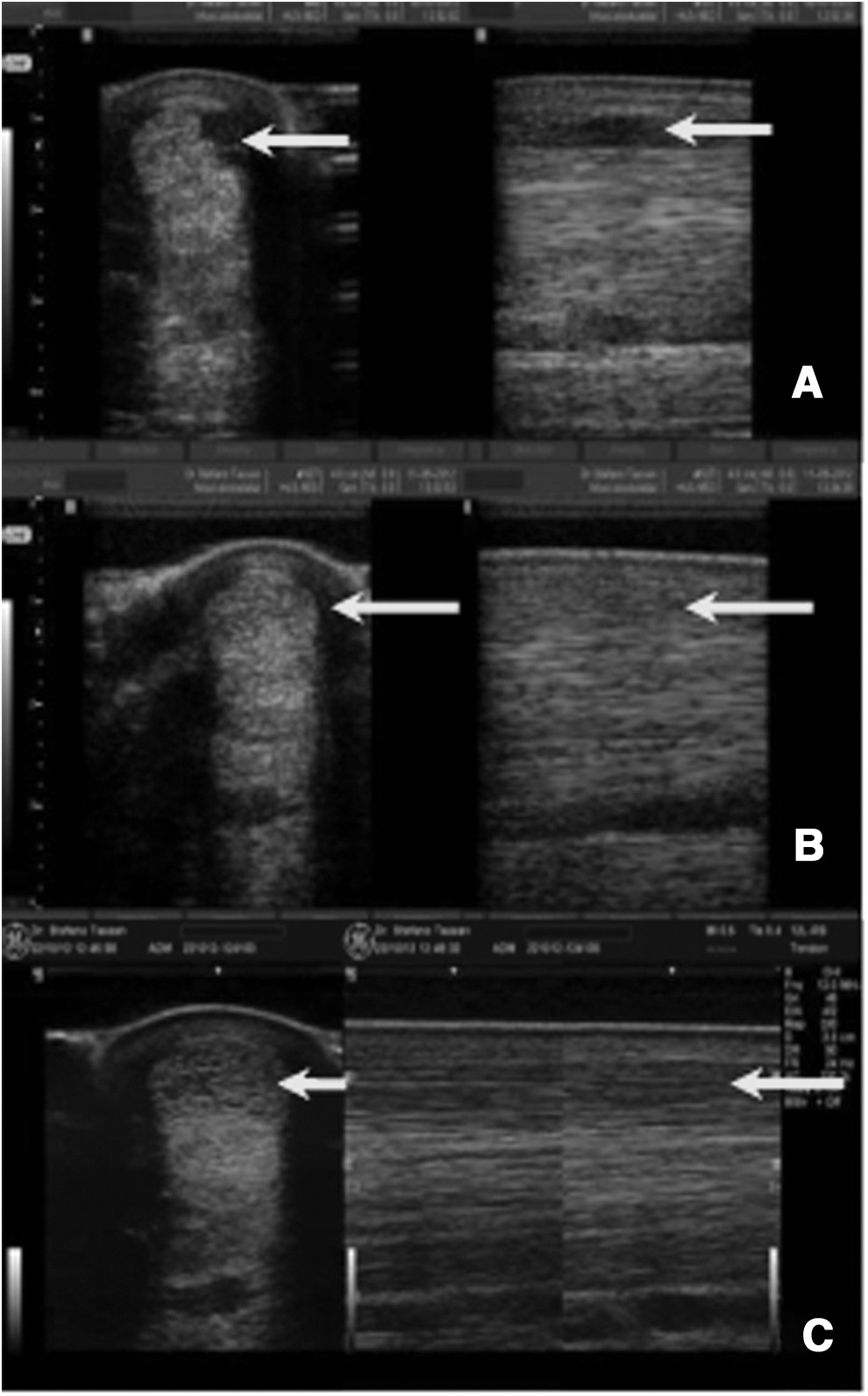
Ultrasound images of SDFT disease treated with the conditioned medium (AMC-CM) monitored at different time intervals

Transverse and longitudinal US scans of a severe acute SLB desmopathy in patient 6. Obvious hypoecogenic area
Six out of the thirteen horses resumed their previous activity level within a time range of 4 to 5 months post-treatment. Three Arabian mares are progressively retraining for long distance endurance racing (120 km), while two extremely severe lesions (one SLB and one DIP collateral ligament) are successfully recovering from dramatic lameness (respectively, 4/5 and 5/5) and have commenced a riding program. Two reinjuries have occurred, one SDFT and one SLB. No obvious repair or regeneration was ultrasonographically observed in the control horses treated with non-CM (Fig. 6A–C).
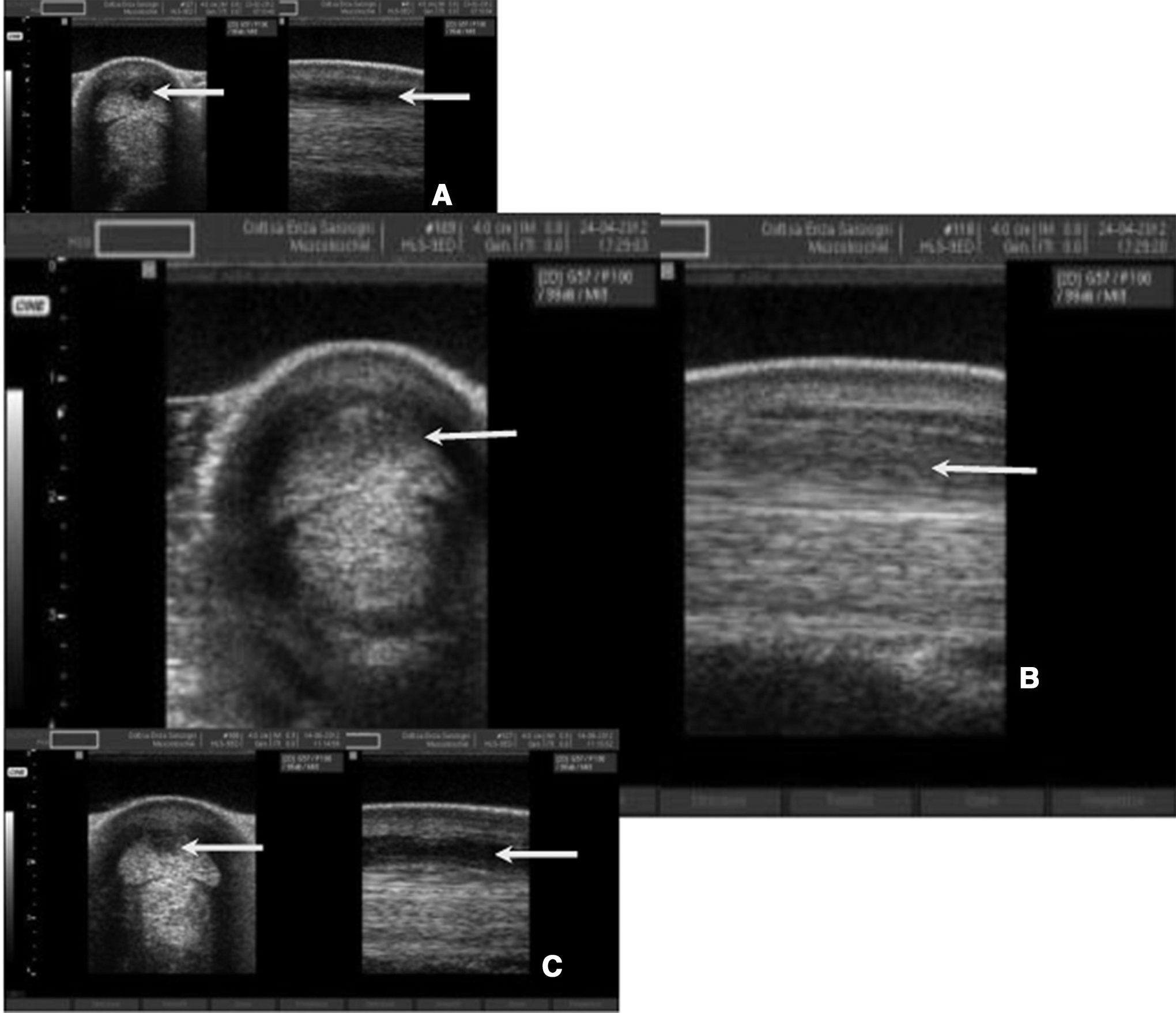
Ultrasound images of SDFT disease treated with the unconditioned medium (control) at different time intervals
Two years after AMC-CM injection, the average incidence of reinjury in horses was 15.38%.
Discussion
As in other tissues, tendon healing follows a sequence of events consisting of an acute inflammatory phase, a proliferative (fibroblastic) phase, and a remodeling phase, during which fibrous scar tissue replaces the originally well-arranged collagen network. The elasticity of a scarred tendon is vastly inferior to that of healthy tendon, which increases the risk of reinjury [25]. To date, MSCs have been considered as viable candidates to support the healing of soft tissue injuries because of their ability to differentiate into tenocytes, which may occur following in vivo transfer [12,26,27]. Current knowledge of the biological characteristics of MSCs also focus much attention on the role of paracrine factors released from these cells, the mechanisms of their regenerative/reparative potential, and on their ability to control the inflammatory process.
The potential immunomodulatory properties of MSCs in horses have been explored by Carrade et al. [28] using MSCs derived from horse BM, adipose tissue, umbilical cord blood, and umbilical cord tissue. These authors showed that MSCs of all of the investigated tissues, when cultured in cell-to-cell contact with PBMCs, decreased lymphocyte proliferation, increased prostaglandin 2 and interleukin-6 secretion, and decreased production of tumor necrosis factor-α and interferon-γ. Here, and to our knowledge for the first time in veterinary medicine, we have demonstrated that horse AMCs are capable of inhibiting PBMC proliferation not only when cultured in cell–cell contact with responder cells, but also when separated from them by a transwell membrane. The inhibitory effects were more pronounced when increasing numbers of AMCs were added to the cultures, suggesting a dose-dependent effect. The finding that inhibition of T-cell proliferation was induced by AMCs in the transwell system suggests that soluble factors are implicated in this phenomenon. This hypothesis was further supported by our findings that PBMC proliferation was inhibited by the AMC-CM. Our results are similar to findings that have been reported using human term placenta, which clearly demonstrate that cells isolated from the mesenchymal tissue of human amniotic membrane, as well as the CM derived from the culture of these cells, could both inhibit lymphocyte proliferation [18,29 –31].
Even though it is generally accepted that MSCs from amniotic membrane or other sources act in a paracrine fashion, mechanisms underlying the immunosuppressive actions of these cells remain to be fully elucidated [for review, see Refs. 20,32,33]. The identity of these soluble factors remain unknown, even though TGF-β1, hepatocyte growth factor, prostaglandin E2, interleukin-10, heme oxygenase-1, interleukin-6, and human leukocyte antigen-G5 are all known to be constitutively produced by MSCs [34 –36]. Recently, Rossi et al. [31] suggested prostaglandins as one of the key effector molecules of the antiproliferative activity of human amniotic membrane-derived cells.
An important role for soluble factors in stem/progenitor cell-mediated reparative effects has been supported by animal experiments using the CM as an effective treatment for different tissue injuries. Indeed, in a porcine model of myocardial ischemia and reperfusion, intravenous and intracoronary injection of the CM obtained from human MSC cultures reduced the infarct size and improved cardiac performance [37]. Furthermore, systemic infusion of human MSC-CM has been shown to reduce apoptosis and stimulate proliferation of hepatocytes in a rat model of acute liver injury [38]. Meanwhile, intramuscular injection of the CM derived from human endothelial progenitor cells has been shown to result in tissue revascularization and functional recovery in a rat model of chronic hind limb ischemia [39].
In support of a key role for soluble factors in the suppressive action of human amniotic membrane-derived cells, Cargnoni et al. [40,41] used a mouse model of lung fibrosis to show that a reduction in severity and progression of the disease could be obtained both after transplantation of amniotic membrane-derived cells and also after the injection of their conditioned medium, thereby underlining the anti-inflammatory effects of these media.
All of the important results described above were obtained using the CM in induced disease, while in our study, for the first time, the CM derived from cultured horse amniotic membrane-derived cells was used to treat spontaneous horse tendon and ligament injuries. We treated 13 horses with different tendon or ligament injuries that were followed up for 2 years. Clinical and ultrasonographical evaluation of the involved tendons or ligaments did not reveal evidence of inappropriate tissue or tumor formation, independently of the type and severity of diseases. In the absence of any perioperative collateral treatment, it is possible to attest that no local or focal reaction has occurred. These results are suggestive of a correlated anti-inflammatory effect of AMC-CM. Indeed, besides a demonstrated lack of worsening of the lesion straight after treatment, a marked reduction in swelling and cross-sectional area in the very early postoperative period was also noticed. Moreover, interestingly, using power Doppler US, neovessels were imaged within the treated area as soon as 1 month after AMC-CM injection.
Neovascularization, as a functional stage of tendon healing, was constantly detected after our treatment both in tendons and ligaments, in accordance to similar observations by other authors [42] using other tendon regenerative treatments such as PRP. An example of this neovascularization is reported in Fig. 5, which relates to a SLB, while a similar pattern was detectable in all the other tendons and ligaments. While improvement in echogenicity and fiber architecture was observed, the vessel size and quantity decreased and eventually disappeared in a later stage, with individual variation, at approximately the fourth month. This is clearly correlated with a positive tissue-healing process, and must be considered as an important timing predictor in the rehabilitation program. To our knowledge, this finding can be considered compatible with the local action of angio-acting cytokines or vascular extended growth factors and should be considered an effective requirement for tendon healing. Clinical outcomes after AMC-CM injection can be considered favorable after 2 years of follow-up. Considering that increasing evidence has recently highlighted the ability of MSCs isolated from various sources to produce bioactive molecules, which are potentially able to exert several types of paracrine effects (eg, anti-scarring, anti-inflammatory, anti-apoptotic) on target cells [43], our observations lead us to hypothesize that soluble factors released by AMCs may interact with and stimulate tendon-resident cells to initiate an anti-inflammatory and angiogenic response, which leads to a regenerative/reparative response. In particular, factors derived from AMC-CM may counteract the action of inflammatory cells accumulated at the site of injury, and may also exert trophic effects, as documented by Tang et al. [44] in the ischemic myocardium and in bleomycin-induced lung fibrosis [41].
Despite the fact that our study population is limited and that statistical analysis would be unreliable, the remarkable low rate of reinjuries observed (15.38%) leads us to speculate that treatment with AMC-CM is very efficacious, especially if one considers that no obvious repair or regeneration was ultrasonographically observed in the control horses treated with non-CM. Moreover, the two reinjury cases observed could be better considered as a standard default of tendon therapies. Indeed, we observed 1 SDFT reinjury out of five horses with the same tendon disease, corresponding to a rate of 20% that is consistent with other author's finding [45] when BM-MSCs were implanted. The other reinjury of the SLB, 1 year after treatment, belongs to a heavy vaulting horse, which was always exercising on the lunge at left rein (as required by the sport). It is well-documented [46] that SLB contributes to joint stabilization by acting synergically to collateral ligaments when horses are exercised in circles, meaning that the lateral SLB of the outside limb (in this case, the right hind) sustains a greater degree of biomechanical stress, and therefore, a second injury at this level has to be considered as the result of cyclical overloading.
On the other hand, it must be underlined that our treatment was successful in a severe condition of a multiple core lesions in the metacarpal and intrathecal SDFT of a patient (case 2), which had already been reinjured after failure of a previous regenerative treatment.
These results are consistent and overlapping (in terms of time interval needed to reach complete healing) with the beneficial effects of transplanted horse amniotic membrane-derived cells that we have observed previously in the same animal model [10,11], and therefore suggest that cell treatment could be substituted by the use of CM derived from the culture of these cells.
In conclusion, our data show that the CM derived from the culture of horse amniotic cells exerts both in vitro immunomodulatory potential and also favors the healing process in damaged tendons, suggesting that in both cases, the effect was exerted by factors released from these cells rather than through cell-to-cell contact.
Our results may open the way to consideration of cell-free treatment approaches for tendon and ligament diseases, offering a series of added advantages with respect to other current treatments. In particular, AMC-CM can be produced easily and in large quantities; it can be stored efficiently because it maintains its efficacy after the lyophilization process; as a cell-free treatment, it can drastically reduce the risk of adverse immunological reactions, infectious risks, and other potential long-term negative effects caused by the presence of exogenous cells; finally, it is also conceivable that AMC-CM could be administered safely via intravenous injection, avoiding clot formation and lung capillary entrapment [40]. Even though this study identifies AMC-CM as a novel therapeutic biological cell-free product in spontaneous tendon and ligament diseases, elucidation of the nature and characteristics of the paracrine soluble molecules underlying the efficacy of AMC-CM therapy, and an understanding of the mechanisms responsible for the beneficial effects of the paracrine actions performed by stem cells in general, remain ongoing challenges for all researchers in the field.
Footnotes
Acknowledgment
Dr. Marco Evangelista is deeply acknowledged for his critical reading of the manuscript and English revision.
Author Disclosure Statement
The authors declare that no competing financial interests exist in relation to this manuscript.