
Abstract
Halting the first clinical trial on the use of embryonic stem cell derivatives for spinal cord injury resulted in disappointment and created concerns about the future use of pluripotent stem cell-based therapy in the treatment of human diseases. This article presents reflections and concerns related to the halted embryonic stem cell-based clinical trial and discusses some important and controversial issues for achieving safe and successful cell therapy. This manuscript highlights two important points for successful translation of pluripotent stem cell-based therapy in clinics: (i) reproducible xeno-free growth and differentiation of pluripotent stem cells in good manufacturing practice conditions as the prerequisites to ensure a defined and controlled cell source and (ii) extensive studies in small and large animal models and comprehensive basic studies to determine any adverse or toxic effects of transplanted cells, especially teratoma formation, in addition to improving surgical procedure and cell delivery system.
Introduction
A
Independently of this pioneering trial outcome, the prevailing opinion regarding hESC-based therapy of SCI is that there are still many hurdles to overcome before translating preclinical studies in animal models to humans [1]. The hESC-based therapy is increasingly recognized as a promising strategy for degenerative disorders, bearing a risk that the race to be the first may convert into a disadvantage for the trial organizers. This raises profound questions related with translational research that involves cell therapy using pluripotent stem cells.
Could the Intention to Be First-to-Market Using hESCs or Any Other Pluripotent Stem Cells Convert in a Disadvantage?
Research in hESCs is undoubtedly promising, but rigorous safety procedures and large-scale basic research must be performed before any application of these cells and their derivatives in the clinic. Two most important points are key to successful translation of pluripotent stem cell-based therapy in clinics: (i) reproducible xeno-free growth and differentiation of pluripotent stem cells in good manufacturing practice conditions are prerequisites to ensure a defined and controlled cell source and (ii) extensive studies in small and large animal models and comprehensive basic studies are needed to determine any adverse or toxic effects of transplanted cells, especially teratoma formation, in addition to improving surgical procedures and cell delivery systems.
Differentiation of Pluripotent Stem Cells Toward Clinically Acceptable Specific Cells and Understanding Their Mechanism of Action
Since the generation of the first hESC line [2], research in this area has progressed at a rapid pace, developing efficient protocols globally for differentiation of these cells to clinically relevant cell types. hESCs bear the advantage over any other stem cells in that they are pluripotent, providing an unlimited starting cell source for differentiation to any type of tissue of the human body. The main requisite for application of these cells in SCI, aside from abundance, is efficient differentiation toward neural cells without traces of pluripotency. Generation of a pure population of OPCs is fundamental for SCI due to the possibility of teratoma formation in the host by undifferentiated cells. In the protocol on which Geron's trial was based [3], this was overcome by a lengthy differentiation procedure in which the cells were exposed to extrinsic factors directing OPC generation and creating nonpermissive conditions for pluripotency. The authors claimed the OPCs yield of over 90%. The first controversy surrounding Geron's clinical trial was the lack of reproducibility in independent laboratories. Although OPCs generated with this protocol were confirmed to be efficient in rat models of thoracic and cervical SCI by the same authors, many investigators raised concerns that this protocol was not sufficiently tested for reproducibility and robustness and therefore the potential for translation was diminished. A concern was also raised regarding the unexplored mechanism of action of generated OPCs besides the remyelination strategy that Geron was pursuing [4]. Extensive mechanistic studies are required not only regarding the transplanted cells themselves, but regarding the trophic support that they may provide to the environment, including endogenous remyelination [5] and increased expression of a number of neurotrophic factors contributing to neuroprotection and even axonal sprouting as reported for other cells [4]. Due to the different nature of potential target mechanisms of transplanted cells, it is important to establish timeframes during which they achieve their beneficial effect in preclinical animal studies. In 2009, the FDA postponed Geron's trial because preclinical data showed that SCI animals treated with GRNOPC1 developed small spinal cysts at the injection site. When these problems were resolved, the trial was reinitiated. Therefore, more time is needed to elucidate the regenerative processes behind the locomotor benefits of transplanted cells and decipher the specific and nonspecific mechanism(s) of cell transplantation and improve safety issues in humans.
Another concern related to Geron's protocol is the presence of animal components in the differentiation procedure. The majority of neural differentiation protocols, including the one used in the trial includes the presence of animal components, bearing a risk of xenogenetic pathogen cross transfer, thus limiting their medical applications. Animal components such as B27 supplement or Matrigel used by Geron should be substituted with human material and tested. Xeno-free conditions for derivation and differentiation of pluripotent stem cells are the main requisite related with the safety issue for future cell therapies [6 –8]. Xeno-derived components as well as teratoma formation should be monitored long after administration in animals (6 months to a year) to improve safety issues for future clinical application.
Animal Models in Preclinical Studies of SCI
Rodent animal models are insufficient to model SCI in humans, not only due to the size difference, which impedes correct dosage prediction in humans, but also due to anatomical and physiological discrepancies, including immune responses. In addition, human SCIs are largely heterogenic, differing in the spinal level, severity, and time since injury [9]. Another significant issue is the surgical procedure in contused and transected animals, which involves laminectomy decompressing the spinal cord before the injury, while in humans decompression occurs hours to days after injury. Therefore, the level of locomotor functional recovery seen in quadruped models is difficult to extrapolate directly to the neurological improvement in humans. The establishment of a consensus animal model that reliably predicts experimental therapeutic outcome in SCI is an impediment for future translational studies. Extensive studies, including small and large animal models covering all types of injury (acute, subacute, and chronic) are prerequisites for translation of stem cell therapy to humans.
The Costs of the Trial
The financial cost is another important issue to be taken into account if the studies are to be continued in patients. Unpredictable variables that may occur in the preparation of products that are to be tested in humans should be taken into account. Even if rodent models are widely available and accessible, the cost of primate studies is still very high and represents only a fraction of the budget required to start the human clinical trial. The collaboration between basic scientists and clinicians in predicting the financial impact of any stem cell-based clinical study is fundamental. With the keen expectations of a large patient community, as was the case with Geron's trial, it is prudent to demonstrate the economic viability before entering Phase I, because abandoning any trial for financial reasons adversely impacts the future of stem cell research and benefits of this research investment. It is to acknowledge that Geron spent over 170 million dollars on this trial and the patient community should be aware that, in addition to scientific efforts, there is a need to invest more to move ahead from the laboratory bench to the patient bedside.
Conclusions
Novel, high-risk therapies have to prove highly efficient over the existing ones to convince the society of its benefits. Despite some current flaws in hESC-based therapy, the potential in this field is recognized and the process of clinical application is inevitable. Huge efforts are necessary in the differentiation procedure, development of xeno-free conditions, reduction of teratoma formation, selection of adequate animal models to proceed to safe human clinical trials (Fig. 1). Geron's experience in terms of growth, manipulation, and injection of appropriate cellular dose of hESC derivatives will benefit others who plan to bring to the clinics similar types of cells. The stem cell field was revolutionized by the discovery of induced pluripotent stem cells that overcame the ethical issue related to hESCs, but still bear safety issues. The other ongoing trial with hESC-derived retinal pigment epithelium (RPE) in patients with Stargardt's macular dystrophy and dry age-related macular degeneration reports exiting results [10]. This trial involves a more promising setup, the eye as a highly accessible, immunologically privileged organ, and RPE cells with simple connectivity and relatively easily obtained in vitro. This stem cell-based trial will certainly serve to gain clinical experience that is directly relevant to the central nervous system or spinal cord therapies. This news underlines the impact of pluripotent stem cells on the medical field with a realistic promise for treatment of many human diseases.
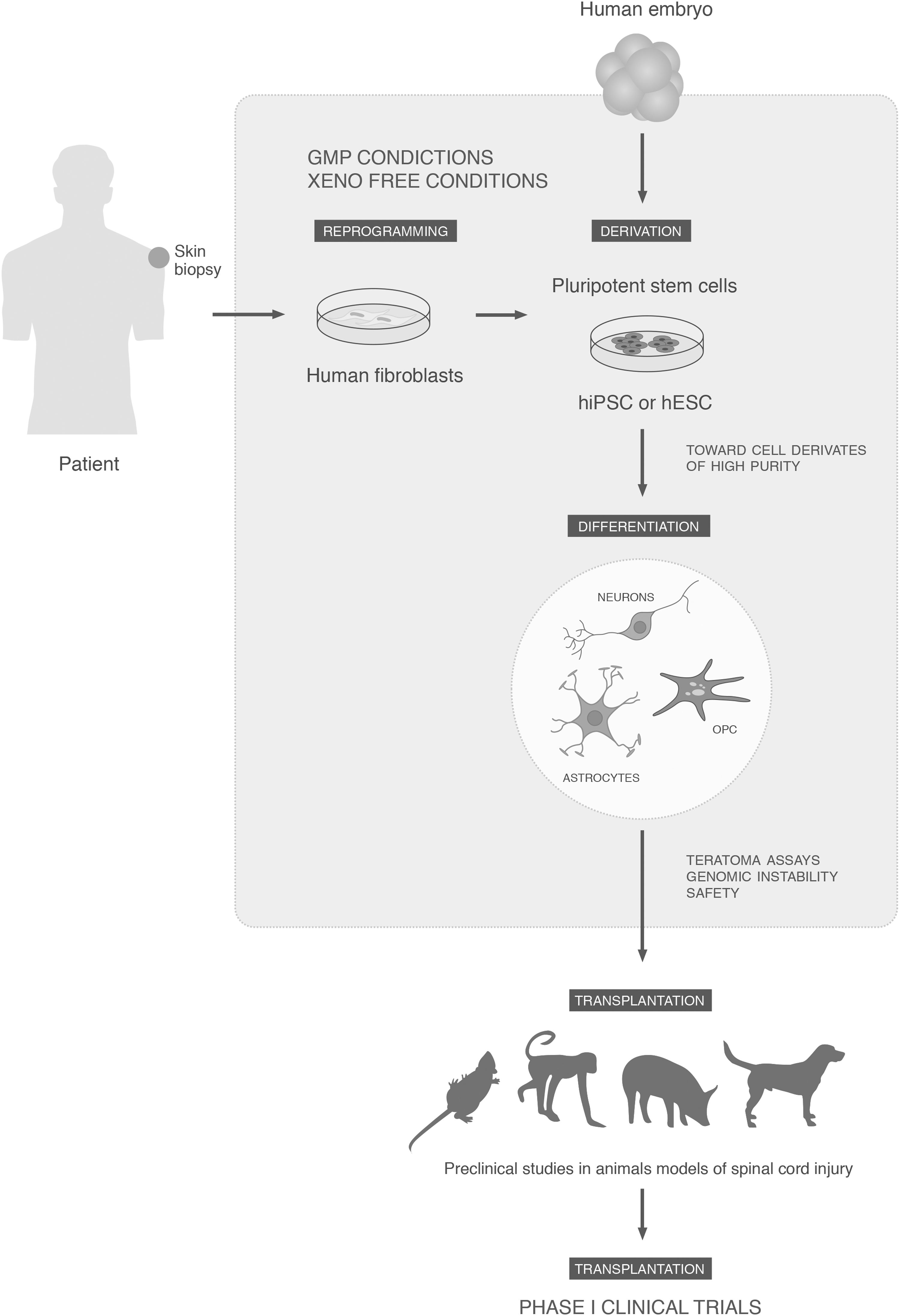
Prerequisites for efficient and safe pluripotent stem cell-based therapy. hiPSCs, generated by reprogramming patient's fibroblasts and hESCs, derived from human embryos can be differentiated toward neural progenitors: OPC, MP, and astrocytes. The processes of derivation and differentiation need to be performed in xeno-free and GMP conditions. Safety assessments of teratoma formation, genome instability, and extensive preclinical studies in large animals are the principle prerequisites required to proceed to clinical trials. hESCs, human embryonic stem cells; hiPSCs, human induced pluripotent stem cells; OPCs, oligodendrocyte progenitor cells; GMP, good manufacturing practice.
Footnotes
Acknowledgments
This work was supported by funds for research from “Miguel Servet” contract of Instituto de Salud Carlos III of Spanish Ministry of Science and Innovation (S.E.), fund for Health of Spain PI10-01683 (V.M.-M.), and Junta de Andalucia PI-0113-2010 (S.E.). The authors would also like to thank Richard Griffeth for English editing.
Author Disclosure Statement
The authors indicate no potential conflicts of interest.