
Abstract
In June 2013, Canadian Blood Services (CBS) established the National Public Cord Blood Bank (NPCBB) accessible to Canadian and international patients and researchers. The NPCBB promotes efforts that contribute to research and improved clinical care by making units not suitable for banking or transplantation available for research. In the context of the NPCBB of the CBS, this article will focus on the practical tools (e.g., consent protocols) developed to optimize umbilical cord blood (UCB) banking and research while enabling ethical provenance of UCB stem cells. The Canadian approach represents an ideal model for comparison as it is a country in which the national public bank (and other regional/provincial public banks) coexists with private companies.
Introduction
Umbilical cord blood (UCB), long treated as waste material, is today considered a valuable source of multiple stem cells (SCs) for both research and clinical applications [1]. UCB is currently regarded as standard practice for the treatment of hematologic diseases [2,3]. The increase in the demand for UCB for clinical applications, paired with the outstanding challenges for satisfying such demand (e.g., volume and expansion and HLA diversity), has generated, in turn, a surge in the use of UCB for research [4]. Biomedical research on UCB will increase our knowledge about current blood SC transplantation practices as well as the processes for collecting, manufacturing, and storing cord blood. Recent studies show the possibility that UCB cells may be useful in the treatment of a variety of diseases, including degenerative neuromuscular disorders [5], wound healing [6], diabetes [7,8], ischemic heart diseases [9,10], and other vascular disorders [11]. In addition to blood precursor cells, UCB also contains SCs that can differentiate into other cell types, thereby fuelling speculation about the use of CB SCs for regenerative medicine [2]. For instance, the derivation of human-induced pluripotent SCs from UCB cells [12] suggests the potential for a valuable and affordable source for the development of novel therapies [13]. Consequently, further research is needed to investigate the expanded potential of UCB and its therapeutic use in both cell and tissue therapies [7,14].
Since the first human UCB transplant, biobanks have been established for the collection and cryopreservation of UCBs [15]. It has been argued that a centralized, national model for UCB is best suited to meet society's needs [16]. In Canada, approximately 70% of patients who need an unrelated blood SC transplant are unable to find a suitable match in their own family [101]. Public cord blood banks can provide additional opportunities for finding a match [16]. Moreover, while approximately 25%–40% of UCB units collected are bankable, the remaining 60%–75% units are not bankable for transplant purposes because of low collection volume of low cell counts [102]. As a result, there are a large number of UCB units that could be available to the research community, thereby stimulating the translation of research into novel cell therapies. Consequently, with the establishment of the first national public cord blood bank in Canada (with hospital collection sites across the country), the National Public Cord Blood Bank (NPCBB) of the Canadian Blood Services (CBS) [103], it is expected that timely access to HLA-diverse, quality–controlled, and ethically sourced UCB will increase. It is foreseen that the increase in the number UCB units would benefit the 400 Canadian patients in need of UCB transplant every year [17]. This will reduce dependency on international sources at the same time as transforming Canada into a global supplier.
This article will report on the establishment of the NPCBB of the CBS with particular focus on the mechanisms developed to optimize cord blood banking and research in Canada. The Canadian UCB banking landscape represents an interesting case study because of its two unique features: first, the coexistence of public national and provincial (Fig. 1) (Hema-Quebec [104]) UCB banks together with flourishing private (for-profit) UCB banks [105 –107]; second, its role as a promoter of biomedical research by making nonbankable units available to the national and international scientific community.

Héma-Québec's mission is to efficiently provide adequate quantities of safe, optimal blood components, substitutes, human tissues and cord blood to meet the needs of all Quebecers; to provide and develop expertise along with specialized and innovative services and products in the fields of transfusion medicine and human tissue transplantation.
The NPCBB of CBS
In June 2013, CBS began operating the NPCBB. The NPCBB has as a core mission the collecting, processing, testing, and storing of cord blood units donated for use by any Canadian or international patient in need of an allogeneic SC transplant. The NPCBB is part of the OneMatch Stem Cell and Marrow Network [108], which is a national program that (a) recruits healthy, unrelated, volunteer blood SC donors; (b) conducts searches for patients who need an unrelated blood SC transplant; and (c) coordinates the delivery of blood SCs when a match is found.
The NPCBB is supported by the CBS, which in turn is funded by the federal and provincial ministries of health. Health Canada has authority to enforce national safety standards for minimizing health risk to recipients of human cells, tissues, and organs under sections 8 and 19 of the Food and Drugs Act [109] and Human Cells, Tissues and Organs for Transplantation Regulations [110]. Health Canada has regulatory oversight through the CBS—for all provinces except Quebec—as well as for the safety of blood products in Canada [111]. Furthermore, the Tri-Council Policy Statement and guidelines from the Canadian Institutes of Health Research add regulatory oversight on the issue of stems cells derived from UCB. The Society of Obstetricians and Gynaecologists [18] and the Stem cell Network [112] have also laid out clear professional guidelines and policy statements, respectively.
Healthy pregnant women of at least 18 years of age reaching 34 weeks or later in their pregnancy can qualify to donate their infants' UCB if neither the mother nor the infant has any diseases or medical conditions that could be transmitted on to a patient who receives a UCB SC transplant (e.g., infectious diseases such as HIV and hepatitis). A mother must deliver at one of the NPCBB's designated collection hospitals in order to donate her baby's UCB. Emphasizing the altruistic aspect of the program, the NPCBB makes it clear that the mother's participation is completely voluntary with no direct benefit to the mother or the infant. There is no cost to the mother for her participation in the program at the same time as there are no reimbursements to the mother for any aspect of the UCB donation. All the cord blood donations to NPCBB are made through the generosity of each individual donor.
Optimizing cord blood banking and biomedical research
As mentioned above, at the core of the NPCBB mission is to facilitate equitable access to ethnically diverse and ethically sourced UCB units for both clinical and biomedical research purposes. Empirical studies assessing the views and attitudes of pregnant women with regard to the collection, testing, and banking of UCB demonstrate that this population is supportive of a system for donating UCB for both potential transplantation and research [19]. However, there are gaps in knowledge and understanding levels, particularly among racial and ethnic communities [20 –24].
Similarly, a survey of Canadian researchers revealed support toward an overarching national framework providing equitable and ethical access to UCB. However, obstacles to equitable access are what most Canadian stakeholders identified a major concern given heterogeneous scientific practices (e.g., procurement) [14,22], and socioethical and policy frameworks. Moreover, it has been noted that despite efforts to harmonize the field [22,113], tools for optimizing access to ethically sourced UCB, via interoperable guidelines for procurement (e.g., consent), access, and transfer of samples/data as well as governance (oversight mechanisms, ethics review), while crucial for public infrastructures such as the NPCBB's, still need to be developed. This was underscored by the fact that certain ethical and policy issues arising in the research context were distinct from those arising during the process of collecting, donating, and using UCB for banking and clinical applications.
While ethical and policy issues associated with UCB collection, banking, and clinical/research uses have been identified and some guidance developed, central issues remain to be resolved [25,26,114]. Debate on what constitutes adequate informed consent for UCB donation also continues (as, for instance, with respect to who should seek consent, from whom, and when consent should be obtained) [26,115]. In the context of UCB research, it is necessary to adopt consent protocols that prospectively address unforeseen secondary uses and international exchange of samples and related data, along with a core list of disclosure elements (e.g., benefits and risks, possible commercialization) [27]. Additional vexing questions are: What are the implications of genetic testing of UCB for the informed consent process? Should donors be informed of test results? How to develop ethnically appropriate and culturally sensitive procedures for UCB collection, donation, storage, and use?
Without a centralized framework accompanied with transparent policies and guidelines, researchers currently obtain UCB from hospital labor and delivery departments, from obstetrician-gynecologists, or from direct solicitation of parents [22] on an ad hoc basis.
This practice does not always provide for quality-controlled or ethically sourced UCB for research (e.g., collecting UCB samples without the parents' consent does not reflect the principle of donor's autonomy [116,117]). As noted in a survey of Canadian researchers [14], the scientific community is supportive of a nationally centralized and public system that will allow access to UCB units and that will diminish public concerns over the use of UCB samples in biomedical research (recommendation 3 in [22], recommendation for oversight in [28], and statement 7 in [118]).
Responding to these collective needs, the NPCBB has developed practical tools building a robust ethical and legal framework for UCB banking, transplantation, and research. With respect to research, the NPCBB has developed national informed consent protocols (Fig. 2,3) for prospective UCB research as well as information pamphlets for potential UCB donors. In addition, much-needed information tools for ethics review boards (and similar groups) to facilitate the interpretation and interoperability of national guidelines have been developed. A robust ethical framework has been designed by way of a two-step process promoting informed and autonomous decision making while respecting privacy and confidentiality.
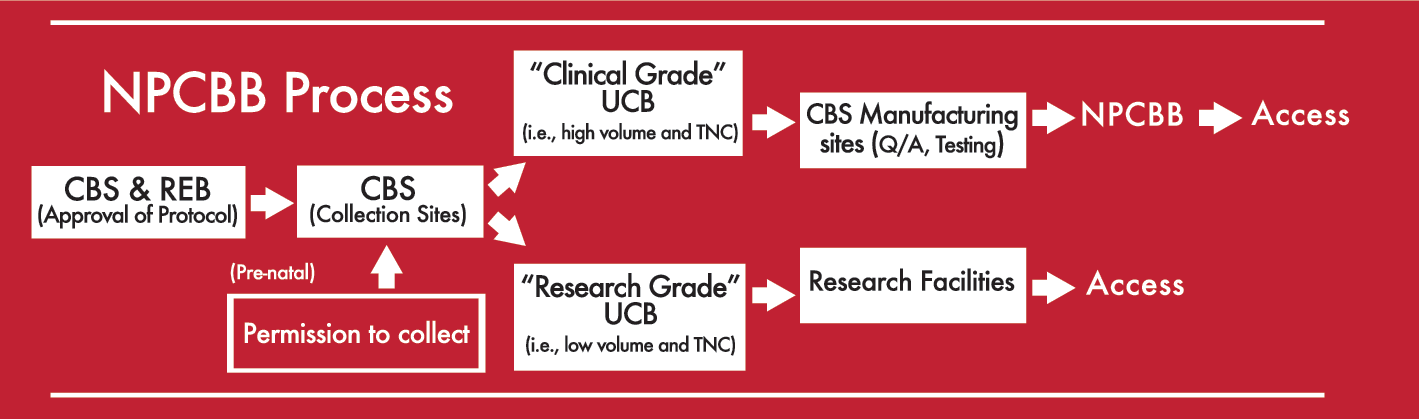
The National Public Cord Blood Bank process.
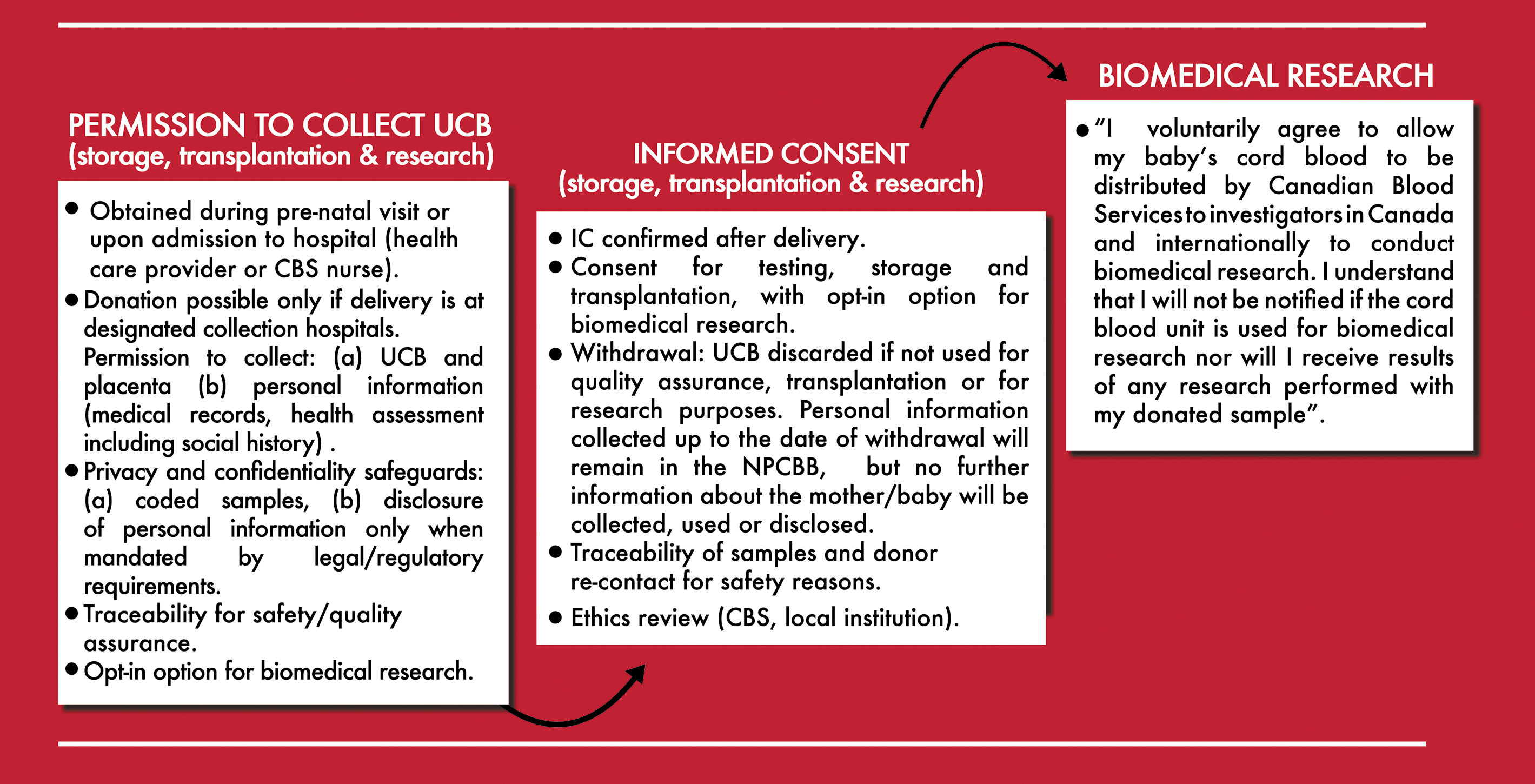
The informed consent process.
A mother initially provides a “permission to collect” at the time of prenatal visits. The permission to collect allows her physician, midwife, and/or the NPCBB staff to collect the infant's cord blood at birth. Verbal and written information regarding the program's goals and practices are provided at this first stage of the process (e.g., two separate donor information pamphlets for transplantation and biomedical research, in addition to information posted on the NPCBB website) so as to ensure enough time to make an informed decision to join the program. After collection, the cord blood units and the mother's blood samples are placed in a secure location until all screening tests are complete. These units are sent to the NPCBB manufacturing facility to start the process of testing and preparing the cord blood for storage. At this second stage of the process a CBS/NPCBB staff member discuss the NPCBB with the mother and reconfirm willingness to participate with an informed consent and undertake the mother's medical history and general health assessment.
At the time of providing the “permission to collect,” the mother is offered the opportunity to provide consent (“opt-in”) for biomedical research if later it is determined that the donated UCB is unsuitable for storage or transplantation. In all cases, the mother's consent can be withdrawn at anytime with no penalty. Donor privacy and confidentiality are protected with robust mechanisms [119]. Personal identifiers are removed from samples donated for biomedical research and replaced by a unique code. Only minimal information about the donor is disclosed to researchers, such as the date of delivery, infant's sex, and the criteria used to determine the unsuitability of the UCB for transplantation purposes. In this manner, donor identity will not be revealed to researchers.
Governance is ensured by mandating that all research protocols be subject to the approval by the CBS and undergoing ethics review by the CBS Ethics Board. In addition, researchers must obtain ethics approval from their own institutions. Furthermore, following international ethical principles, CBS encourages researchers to disseminate scientific knowledge by presenting the results of biomedical research in meetings and publishing in scientific journals (statement 30 in [118]).
Conclusion
UCB banking was initially developed for the storage of unrelated UCBs [29]. However, private (commercial) banks eventually offered UCB storage for future autologous transplantation. This appealed to future parents who wanted to take a “biological insurance” for their children [20,120]. However, to this date, estimates show only a small probability of lifetime use in a family without known health issues [30]. Indeed, a Eurocord study conducted between 1988 and 2007 found that only three autologous SC transplantations were performed out of total of 3,372 [31]. Private UCB banking is an expensive endeavor with an annual storage price of at least $125 in Canada [105 –107] and $180 in the United States [32], in addition to other fees (“family registration,” processing, etc.).
Promoting public UCB banking is not unique to Canada; several countries lead the way by forbidding private cord blood banks (e.g., Italy and France) or establishing regulatory frameworks applicable to both public and private UCB banks [121]. In the United States, the Health Resources and Services Administration supports 13 public banks [33]. The U.S. Food and Drug Administration (FDA) now considers UCB to be a biological product [122] and mandates UCB banks that store samples for potential therapeutic purposes to operate under strict conditions [34,123,124], including obtaining and renewing a license. While the new FDA regulatory framework responds to the need to establish quality control and oversight systems over UCB banks, there are concerns that this new regulatory environment does not fuel innovation in the field of SC research and regenerative medicine [35]. As of August 2012, only three UCB banks had completed this new licensing process [124], demonstrating that enforcing the regulations remains a major endeavor. Moreover, there is the possibility that only larger U.S. UCB banks (mostly private) would be able to afford the cost associated with the complex regulatory system put in place by the FDA since 2009 [33]. The U.S. context thus presents a valuable case study for other countries wishing to reform their regulatory frameworks.
To ensure the sustainability of a public not-for-profit system such as the one promoted by the NPCBB, novel frameworks for financing and joining UCB resources should be considered, such as public–private partnerships [36,125]. The coexistence of private–public and provincial–national UCB banking in Canada could be used as an evolving model for optimizing UCB collection, patient care, and fostering novel research in the field of SC science.
In a country in which both public (provincial and national) and private systems coexist, a way to move forward is to foster cooperation between these entities. One way to optimize UCB usage is for private UCB banks to encourage their clients to consent to donating UCB samples that are found unsuitable for storage or therapeutic uses to public biomedical research (recommendation 1 in [22]) [36]. This approach, already adopted by several states in the United States [126,127], would make best use of UCB resources that currently exist in the private and public UCB banks across Canada.
Footnotes
Acknowledgments
This project was supported, in part, by the CBS and the Stem Cell Network of Canada.
Author disclosure statement
The authors' funding sources have played no role in the design, interpretation, or writing of the present article. No competing financial interests exist.