
Abstract
Cellular therapy for liver disease has been available in the clinic for more than 20 years, yet remarkably few patients receive this experimental therapy. Reasons for the small number of transplants performed are partially related to access to useful liver tissue and the difficulty with the isolation of viable cells. Stem cell sources of hepatocytes could theoretically relieve these obstacles to therapy if large numbers of functional hepatocytes could be generated and transplanted without risk of tumorigenicity. To date, there are no reports of stem cell sources with all of these characteristics, despite claims otherwise. Here we report the results of preclinical studies with appropriate animals models of metabolic liver disease and acute liver failure, and their correction by the transplantation of human amnion epithelial stem cells. The encouraging results of the preclinical studies have motivated the movement of isolation and banking of these cells to good manufacturing practice conditions so that the cells can be used in the clinic for transplantation of patients with liver disease.
Introduction
Regenerative medicine has the potential to produce a paradigm shift in medicine. It is likely that stem cell therapy will be intimately involved and greatly responsible for this shift. With few exceptions (antimicrobials, hormone replacement therapy), traditional medicine has been concerned with treatment of symptoms of disease but rarely the correction or reversal of the disease process itself. The alleviation of the symptoms of disease has immediate and positive effects on patient health and welfare, and will have a continuing role in medical therapy. Whenever possible, medical therapy should also contain a component of disease correction. Correction of a disease process can be accomplished through several mechanisms. The therapy applied can itself replace or reverse the disease-causing process. An example of that would be the direct transplantation of dopaminergic neurons into the brain of a Parkinson patient. If effective, the transplanted cells would directly replace the degenerated neurons of the patient and an immediate effect or function of the transplanted cells could be expected. A second method of disease correction is by facilitating of the body's natural regenerative processes. In this approach the cellular therapy applied may not directly replace the missing function or correct the defect, but would allow the regeneration and the repair of the defect by the body's own cells. Regeneration and repair could proceed via many processes; for example, paracrine factors could facilitate or enhance the proliferation of resident cells at the damaged site to repair the damage and restore function. A second mechanism to enhance repair of damage is via inhibition of processes that actually prevent natural regeneration from occurring. Examples of this would be the formation of scar tissue on skin or internal organs such as lungs, kidney, or liver in response to damage. There is strong evidence that all of the processes described above play a role in stem cell therapy of disease [1 –3]. It is thought that throughout evolution there was strong survival pressure and selection of mechanisms to close or limit a wound. These pressures resulted in “healing” processes that quickly close wounds with little regard for long-term function of the damaged organ. Chronic damage and the replacement of functional organ tissue with scar tissue results in loss of organ function. Drastic treatments such as whole-organ transplantation are frequently the only therapy for severely compromised organ function. Since stem cell therapy has the capacity to influence all of the processes described above, there is scientific support for the continued investigation of stem cell therapy in regenerative medicine and their translation to the clinic. However, problems remain with these technologies. Which cells should we use? And importantly, how should we apply them?
For simplicity one could consider stem cells in two broad groups based on their presumed properties: embryonic/embryonic-like and nonembryonic stem cells. In the embryonic/embryonic-like group, one would place embryonic stem cells and any cell type reprogrammed or induced to pluripotency (iPS) with genetic or other factors [4,5]. A second broad category of nonembryonic stem cells would contain all other stem cell types that have been identified and reported from fetal, neonatal, or adult tissues such as mesenchymal stem cells (MSC) [6] or amnion-derived stem cells [7]. The choice of a particular stem cell type for an experimental therapy would depend on the time frame expected for translation to the clinic. While pluripotent stem cells have the greatest potential to produce different tissues, their efficient differentiation to a particular mature cell type, and the potential for tumor formation from any undifferentiated cells remaining in the population are serious impediments to a quick translation to the clinic [8]. While limited clinical trials are underway with specific pluripotent stem cell-derived cell types, their use in the regeneration of major organs such as liver, pancreas, lungs, or kidneys is still laboratory science [9 –11]. Adult stem cells from various sources are already in clinical trials in several countries [12]. The general lack of tumorigenicity of this cell type has motivated the rapid translation to the clinic.
Cellular therapy of liver disease
Over 30 years of laboratory research with animals has shown that certain liver diseases can be treated by the transplantation of isolated liver parenchymal cells (hepatocytes) without the need for whole-organ transplantation [13 –19]. Our group was the first in the United States to translate hepatocyte transplantation to the clinic to treat liver diseases, including acute liver failure (ALF) and metabolic liver disease [20 –23]. In addition, hepatocyte transplantation has been used as a “bridge” technique to keep patients alive long enough to receive a whole-organ transplant. Now more than 13 centers around the world have developed hepatocyte transplantation technology [24]. While effective, at least in the short-term, hepatocyte transplantation has been hampered to a large extent by the same problems that limit liver transplantation: the availability of the liver [25,26]. Thus, alternative sources for the cellular therapy of liver disease have been the focus of much recent research. While ES and iPS-derived hepatocyte-like cells have been produced, their level of differentiation is quite primitive and the tumorigenic potential of these cells has not been overcome to the level required for a clinical study where billions to tens of billions of cells would need to be transplanted. Alternative cell types will be needed for a timely translation of the stem cell therapy to the clinic.
Hepatocyte-like differentiation of human amnion epithelial cells
Miki et al. reported that human amnion epithelial cells (hAEC) isolated from term placenta have surface markers and gene expression profiles that are similar to those reported for human ES cells [7]. Additional studies reported that under specific culture conditions hAEC could adopt hepatic characteristics [27]. Previous studies suggested that human amnion membrane or isolated epithelial cells could be safely transplanted into animals or patients and that they could be useful in the treatment of liver diseases, including Nieman–Pick or liver cirrhosis [28 –33].
As with ES or iPS-derived hepatocyte-like cells, hAEC-derived cells showed primitive hepatic differentiation in culture. However, if freshly isolated cells were transplanted into the liver of SCID/beige mice, without prior differentiation in culture, human cytochrome P450 genes, plasma proteins, and many nuclear hormone receptors and hepatic transport proteins were expressed at levels observed in normal human liver tissue [34]. Presumably, the microenvironment provided by the transplantation of hAEC into the liver enabled maturation of liver gene expression far beyond that previously observed in cultured cells. Normal copies of genes known to be mutated in human metabolic liver diseases such as Crigler–Najjar or the urea cycle defect, ornithine transcarbamylase deficiency, were expressed at high levels when hAEC were transplanted into the mouse liver. Encouraged by the lack of tumorigenicity of the stem cell and the expression of genes that could correct metabolic liver diseases, additional studies were designed to test the hypothesis that hAEC transplantation might be useful to correct these liver defects.
Preclinical studies of hAEC therapy of metabolic liver disease
The efficacy of hAEC transplants was assessed in animal models of two human metabolic liver diseases: an intermediate form of maple syrup urine disease (iMSUD) and phenylketonuria (PKU). Mutations in the enzyme responsible for metabolism of branched chain amino acids, branched chain α-keto acid dehydrogenase (BCKDH), result in MSUD. Mutations in phenyalanine hydroxylase and the resulting alterations in phenylalanine (Phe) levels are responsible for the symptoms observed with PKU. The liver contains the highest level of these enzyme activities, and both are considered liver-based metabolic diseases. Liver-directed cellular therapy, if effective, could be beneficial in the treatment of both PKU and MSUD. Prior studies indicated that the transplantation of mouse hepatocytes resulted in the improvement of life span and the correction of many of the amino acid and neurotransmitter levels observed in a mouse model of iMSUD [35,36], so additional studies were initiated to determine if hAEC transplantation was effective therapy for this liver disease.
The transplantation procedures were similar for the two diseases and are condensed and presented in Figure 1. Amnion membrane is stripped from the remaining placental tissue and incubated in 0.05% trypsin–EDTA (2 × for 30 min) while rotating vigorously at 37°C. Epithelial cells released by trypsin are then used for transplants, cryopreserved for later use, or plated for additional experiments. Cells plated on cell culture plates have a simple epithelial morphology as shown in Figure 1.
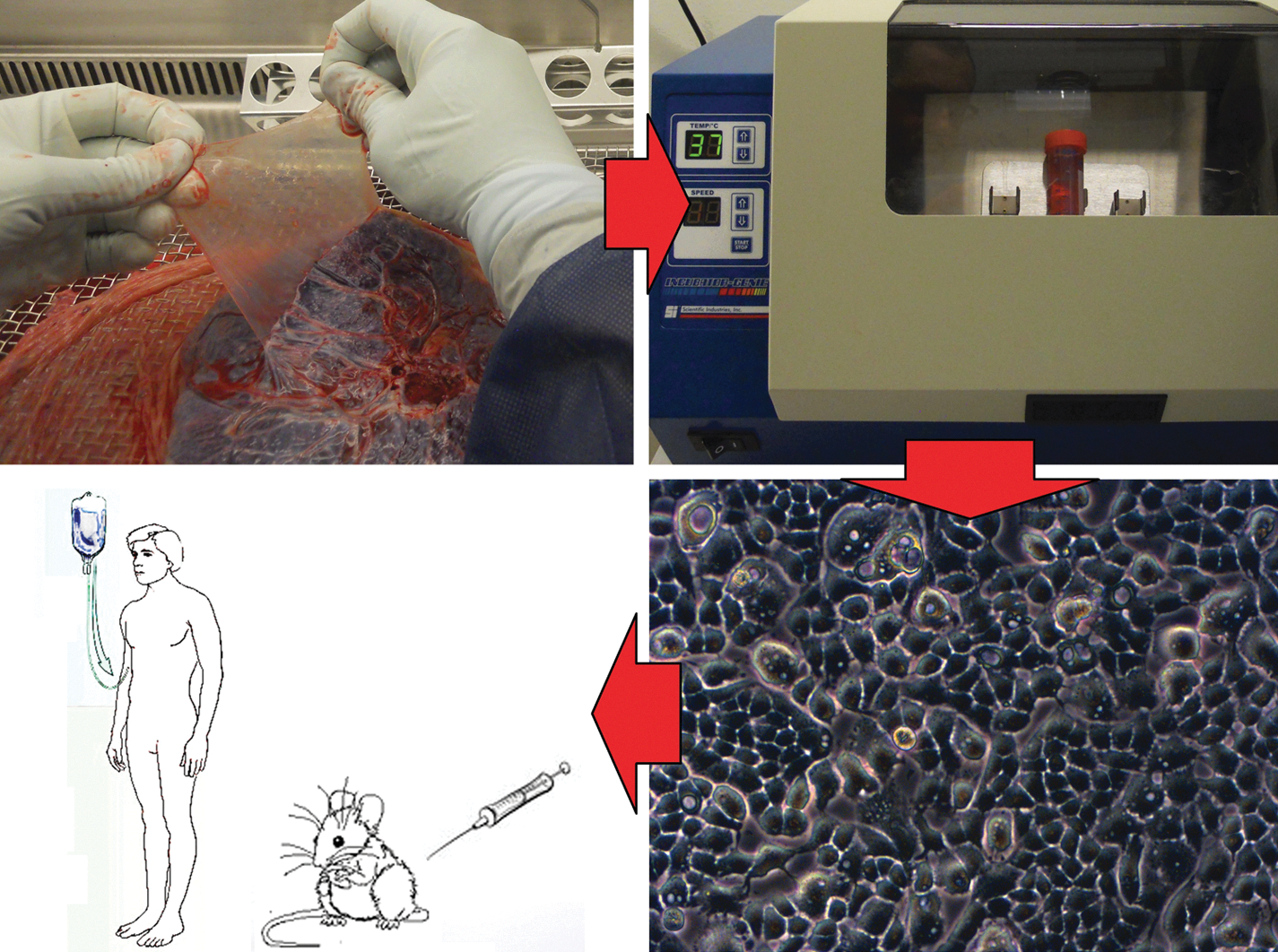
Diagram of the isolation of epithelial cells from human amnion. The amnion layer is stripped from the other placental tissues and incubated with trypsin to release the epithelial cells. Rotating the tissue rapidly during the incubation enhances the yield of cells. Isolated cells can be transplanted into mice or plated for additional experimentation.
Homozygous affected animals were given two direct liver injections of 1 × 106 cells over the first 10 days of life and an additional 4 × 106 cells between 21 and 35 days of life [37,38]. Control animals received injections of Hanks balanced salt solution (HBSS), the medium used to infuse hAECs. No additional cells were transplanted, and the animals were maintained on a normal protein diet throughout their life. All iMSUD animals that received HBSS only and did not receive hAEC transplants died before 28 days of age with severe cachexia, muscle weakness, and seizures. Nine of 11 animals (82%) transplanted with hAEC survived to 100 days, displayed normal weight gain and activity, and showed no gross symptoms of the disease. Transplanted animals were euthanized at 100 days for biochemical and molecular analysis. In MSUD, mutations in BCKDH activity result in elevations in branched chain amino acids (leucine, isoleucine, and valine) in the serum and brain. Transplantation of hAEC normalized the levels of leucine, isoleucine, and valine as well as alanine in both the serum and brain, and reduced the levels of alloisoleucine by >80%. The liver of transplanted animals contained approximately 5% human DNA, and BCKDH activity in the liver increased by 5%–7%, indicating the continued presence of human cells and enzyme activity that correlated well with human DNA content of the mouse liver [37,38].
Human AE cells engrafted and survived long-term in immunocompetent mouse livers without administration of immunosuppressive drugs. Although additional investigations are needed to determine the mechanism of action in this particular model, the immunomodulatory properties of amnion and hAEC are well known [39 –43]. It has been shown that hAEC inhibited mixed lymphocyte reactions in a dose-dependent manner with 66%–93% inhibition [44]. The immunomodulatory mechanism might involve secretion of suppressive mediators such as TNF-α, FasL, TRAIL, TGF-β, and MIF or by cell-to-cell contact with responding T cells. Some reports suggested that the presence of HLA-G immunological cell surface molecules is responsible for the cell-to-cell immunosuppressive properties of hAECs. In addition, the expression of complement inhibitory proteins, CD59 antigen, decay-accelerating factor, membrane attack complex, and Fas antigen/CD95/APO1 is likely responsible for the xenogenic immunoregulatory effects [45 –47].
Studies are ongoing with an animal model of PKU transplanted with hAEC, and the preliminary results suggest that hAEC will correct PKU as effectively as iMSUD. Affected animals received transplants of mouse hepatocytes or hAE, or vehicle control. Brain Phe levels were improved by 50%–75% in animals receiving mouse hepatocytes, and completely normalized in animals receiving hAEC transplants. In PKU animals, high Phe levels alter the levels of many other amino acids and neurotransmitters. Transplantation of hAEC also normalized brain levels of amino acids, including taurine, glycine and aspartate, serine, histidine, and phosphoethanolamine (Skvorak et al., in preparation). The normalization of brain Phe levels in PKU animals given hAE transplants is important preclinical evidence to support the translation of this cellular therapy to the patients.
hAEC therapy of ALF
ALF can occur after acute viral hepatitis, acute-on-chronic liver disease, toxin exposure, or major liver surgery, and is characterized by massive tissue damage that leads to impaired and/or insufficient hepatic function. In severe cases, liver transplantation (whole organ) is the only useful therapy. As indicated above, hepatocyte transplantation has been used in acute-on-chronic liver failure to “bridge” or support liver function in patients waiting for an organ transplant. In addition to chronic liver diseases, hepatocyte transplantation has been used as cellular therapy for ALF [48,49]. In a few reports, ALF patients who received hepatocyte transplants while waiting for a liver transplant recovered completely without subsequent whole-organ transplantation. Similar to MSCs, hAECs have been reported to have immunomodulatory and anti-inflammatory properties that may be of particular benefit in the cytokine ALF and other liver diseases [50 –53]. The efficacy of hAEC transplants was evaluated in a robust and reproducible model of ALF in mice. Mice were given a dose of d-galactosamine (d-gal) that was fatal to 100% of otherwise untreated animals within 3 days. A subgroup of animals was transplanted with 2 million hAECs via splenic injection 6 h after intoxication with d-gal. Animals that received d-gal alone all died within 72 h, while 100% of the animals that received hAEC transplants after d-gal treatment survived. There were corresponding and significant improvements in AST and ALT levels in the hAEC-treated animals. Animals receiving hAEC transplants displayed normal activity and no signs of distress by day 3 posttransplant and appeared to enjoy a complete recovery.
Summary
Both the iMSUD and the PKU mice are thought to be faithful models of the corresponding human disease, with respect to the mutations in the disease-causing genes and the alterations in amino acids and neurotransmitters in affected animals. The corrections of the biochemical imbalances characteristic of the disease by cellular therapy is encouraging. The observations that hAEC works as well or better than mature mouse hepatocytes in the correction of disease are particularly encouraging as these preclinical studies suggest that hAEC could be used in the clinic to treat these liver-based metabolic diseases. In addition to the correction of metabolic liver disease, hAEC were shown to effectively reverse the biochemical, histological, and lethal effects of d-gal-induced ALF. Because of their immunomodulatory properties, both MSC and hAEC might be equally effective in the reversal of some forms of ALF, particularly those where the immune systems is activated and sensitized to destroy hepatocytes. However, MSC have not been shown to express liver genes at mature liver levels and have not been shown to be effective in the correction of metabolic liver disease. It is desirable and efficient to have one cell type, hAEC, that could be isolated and banked under good manufacturing practice procedures and available for cellular therapy of metabolic liver disease and ALF. On the basis of the work reported here, information has been submitted to the regulatory authorities to begin isolation and banking of hAEC under conditions that will allow their use in the clinic for transplantation for the treatment of human liver disease.
The protocol to be proposed is one of minimal manipulation. In such protocols, the cells are isolated from the tissue and used directly for a transplant procedure, or cryopreserved for a later transplant. Such a protocol avoids many of the problems concerning ex vivo expansion of the cells, possible genetic changes accrued during the culture period, and avoids the identification of culture media, growth factors, and other reagents that are compatible and approved for use in cells for a clinical transplant. Since the preclinical studies were conducted with cells that were not expanded or differentiated before the transplant, the data gained in the preclinical studies are relevant to and support a minimum manipulation protocol.
One issue that remains is that of immunosuppression. Nearly by definition, the placental stem cells will be used in allogeneic transplants. For cases of metabolic liver disease as described here, the cells from the placenta will carry the same mutation as the liver of the infant so that autologous transplant of these cells would not result in a correction of the phenotype. With allogeneic transplants, immunosuppression of the patient at the time of transplant is the normal procedure. Patients who are candidates for the hAE stem cells would be those already listed for allogeneic hepatocyte transplants; thus, no alteration of the hepatocyte protocol would be needed. The immunosuppression protocol would be identical whether the recipient received allogeneic hepatocytes or hAEC, and no new risks attributable to immunosuppression would be added to the transplant procedure. As already discussed above, the hAEC appear to be immune privileged. It is not clear whether immunosuppression would be required posttransplant. No immunosuppression was administered to the mice in the preclinical studies, and even the xenogeneic-hAEC were retained throughout the observation period. Whether the ability to correct a metabolic liver disease with hAE transplants and the lack of a requirement for immunosuppression posttransplant can be translated to the clinic will be examined soon.
Pluripotent Stem Cells • macular degeneration • spinal cord injury
Adult Stem Cells • Mesenchymal stem cells ➢ Graft verses host disease ➢ Crohn's disease ➢ Type 1 diabetes ➢ Pulmonary fibrosis ➢ Liver cirrhosis ➢ Ischemic stroke ➢ Multiple sclerosis ➢ Wound healing • Neural stem cells – amyotropic lateral sclerosis (ALS) • Limbal stem cells – limbal stem cell deficiency
(Source:
Footnotes
Acknowledgments
This study was supported by grants from the National Phenylketonuria Alliance (R.G. and K.S.), California Institute of Regenerative Medicine (TR3-05488 to T.M.), Pfizer Inc., and by the Torsten and Ragnar Söderberg Professorship in Regenerative Medicine (S.C.S.).
Author disclosure statement
S.C.S. and T.M. own stock in Stemnion LLC. No cells or products from Stemnion LLC were used in these studies.