
Abstract
In this retrospective study, 209 patients with malignant disease were analyzed for levels of T-cell receptor excision circles (TRECs) for the first 24 months after allogeneic stem cell transplantation. CD3+ cells were separated by direct antibody-coupled magnetic beads, followed by DNA extraction according to a standard protocol. The δRec-ψJα signal joint TREC was measured with real-time quantitative PCR. Patients were grouped based on malignant disease: chronic myeloid leukemia, chronic lymphatic leukemia, acute myeloid leukemia (AML), acute lymphocytic leukemia (ALL), and myelodysplastic syndrome (MDS). Patients were further subdivided based on TREC levels below (low-TREC) or above (high-TREC) median at each time point. TREC levels were then correlated to relapse incidence and relapse-free survival (RFS). For patients with AML, low TREC levels 2 months post-transplantation were correlated to high relapse incidence at 5 years (P<0.05). In patients with chronic leukemia, high TREC levels were correlated with improved RFS (P<0.05). For patients with MDS, high TREC levels at 9 months post-transplantation were associated with higher RFS at 5 years (P<0.02) and lower relapse incidence (P<0.02). This study shows the potential use of TREC measurement in blood to predict relapse in patients with AML and MDS after allogeneic hematopoietic stem cell transplantation.
Introduction
A
The reconstitution of T cells post-ASCT depends on the peripheral expansion of T cells originating from the graft as well as differentiation of T cells from donor hematopoietic stem cells (HSC) [6,7]. The thymic output of de novo, differentiated T cells can be estimated by quantification of T-cell receptor excision circles (TRECs) in peripheral blood [8 –10]. TRECs are formed as a circular DNA by-product after the rearrangement of the T-cell receptor genes. Since TRECs are not duplicated during mitosis, their concentration in peripheral circulation decreases after every T-cell division. Due to this, the levels of TREC give an indirect measurement of thymic output.
Several reports have described parameters that affect thymic activity after ASCT [9,11 –13]. However, less is known about how TREC levels post-ASCT affect clinical outcome. Low TREC levels have been associated with an increased incidence of CMV reactivation [14]. This finding is supported by another report that also demonstrated a correlation between low TREC levels and higher transplant-related mortality (TRM) [9]. Decreased TREC levels after ASCT have further been associated with lower overall survival (OS) [9,15]. To date, only small studies have shown an association between TREC levels post-ASCT and relapse of malignant disease [16,17].
In this study, we analyzed the impact of TREC levels after ASCT on disease relapse and survival in patients with hematological malignancies. Due to the difference in treatment protocols and disease etiology, the patient cohort was split into subgroups based on disease type. We show that a low TREC count after ASCT was associated with an increased relapse rate in patients with acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS). Lower TREC levels were also associated with decreased OS in individuals with chronic leukemia and MDS.
Materials and Methods
Patients
This study included 209 patients with hematological relapse who had undergone ASCT at the Centre for Allogeneic Stem Cell Transplantation, Karolinska University Hospital, between September 2002 and April 2009. Part of the patient material was also included in a study by Sairafi et al. [9]. All patients had a minimum follow-up time of 3 months. Leukemic relapse was defined as 20% or more blast cells in bone marrow (BM) aspirates on morphologic examination or as extramedullary occurrence of leukemic cells. In chronic myeloid leukemia (CML) patients with increasing levels of BCR-ABL, a BCR-ABL ratio exceeding 0.02% on three consecutive occasions or a ratio of 0.05% on two occasions was also defined as relapsed disease. Patients with MDS were classified according to both the French-American-British (FAB) Cooperative Group and the WHO classifications. All recipients and donors were typed for HLA class I and II by allele-level PCR sequence-specific primers [18]. Additional information about the patients, treatment procedures, and supportive care are given in Table 1. This study was approved by the regional ethics review board (approval No. 2011/549-31/1).
Low risk, first remission or first chronic phase; high risk, beyond these stages; BM, bone marrow; CML, chronic myeloid leukemia; CLL, chronic lymphocytic leukemia; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; MDS, myelodysplastic syndrome; MM, mismatch; Cy, cyclophosphamide; fTBI, fractionated total body irradiation; Bu, busulfan; Melf, melfalan, Flu, fludarabine; ATG, anti-T-cell globuline; Treo, treosulfan; CsA, cyclosporine A; MTX, methotrexate; FK, tacrolimus; RAPA, sirolimus; PBSC, peripheral blood stem cell; NC, nucleated cell; GVHD, graft versus host disease.
Conditioning
Myeloablative conditioning regimens (MACs) consisted of cyclophosphamide (60 mg/kg daily) for 2 days combined with 12 Gy (4×3 Gy) of fractionated total body irradiation (TBI), busulfan (1 mg/kg daily) for 4 days, or a combination of busulfan and melfalan [19]. The reduced intensity conditioning regimens consisted of fludarabine in combination with TBI and/or other cytostatic agents [20]. All patients receiving grafts from matched, unrelated donors (MUD) were in vivo T cell depleted using antithymocyte globulin (2 mg/kg for 3–4 days before transplantation [21]).
Graft versus host disease prophylaxis
The majority of patients (92%) were treated with cyclosporine A (CsA) combined with four doses of methotrexate (MTX). CsA was discontinued after 3 months in cases with a sibling donor or after 6 months for MUD transplants. Fifteen patients received a combination of tacrolimus and sirolimus (Table 1).
TREC analysis
Patient blood samples were collected 2, 3, 9, 12, and 24 months after SCT. CD3+ cells were separated using direct antibody-coupled magnetic beads (Dynabead System; Invitrogen AS) followed by DNA extraction according to a standard protocol. DNA samples were stored at −20°C until use.
The δRec-ψJα signal joint TREC was measured using a TaqMan real-time quantitative PCR protocol with primers and probes directed to the signal joint region [22]. The amount of TRECs in CD3+ cells was expressed as the ratio between TRECs and the housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and calculated using the delta-CT method, formula 2(Ct GAPDH−Ct TREC). TRECs and GAPDH were analyzed in multiplex. The methodology of TREC analysis is described in more detail elsewhere [9].
Statistical analysis
The probabilities of OS were estimated using the Kaplan–Meyer method and compared with the log-rank test. Relapse and TRM were estimated using an estimator of cumulative incidence curves taking competing events into consideration. The Mann–Whitney U test was used to compare continuous variables, and Fisher's exact test was used to compare the distribution of categorical variables. Predictive analysis for OS was performed with the Cox proportional hazards regression. Predictive analyses for relapse, TRM, and graft versus host disease (GVHD) were based on the proportional hazards model for subdistribution of competing risks. Univariate and multivariate analyses were then performed using Gray's test and the proportional subdistribution hazard regression model developed by Fine and Gray. Factors that were included in the statistical analysis were age, donor type, graft type, risk, cell dose, blood group and HLA matching, conditioning, ATG, GVHD, infections, T-cell chimerism, and the use of mesenchymal stromal cells and TREC levels. Factors that showed a P value of<0.1 in the univariate analysis were included in the multivariate analysis.
Results
Low TREC levels after ASCT are associated with increased risk for relapse in AML patients
Patients with AML were analyzed separately for the correlation between TREC levels after ASCT and relapse incidence and relapse-free survival (RFS). Of the tested time points (2, 3, 6, 12, and 24 months), a significant correlation existed only at 2 months between lower TREC levels and a higher incidence of relapse (P<0.05) (Fig. 1a). Only a trend (P=0.15) could be observed at 2 months between RFS and low TREC levels (Fig. 1b). There was no correlation observed between TREC levels and OS or incidence of acute graft versus host disease (aGVHD) at any time points (data not shown). Multivariate analysis of risk factors associated with relapse in AML patients showed that both the use of peripheral blood stem cells (P<0.05) and TREC levels above median at 2 months (P<0.05) were associated with decreased relapse (Table 2). A major ABO bloodgroup mismatch (P<0.01) between donor and recipient was associated with an increased relapse rate. Multivariate analysis for RFS only showed a disadvantage for patients with high-risk disease (P<0.02) and bacteremia post-ASCT (P<0.01).

Acute myeloid leukemia (AML) patients. Incidence of relapse
Multivariate was not possible to perform due to 0 individuals in one patient group.
RFS, relapse-free survival; high risk, beyond first remission or first chronic phase; HSV, herpes simplex virus I and II; VZV, varicella zoster virus; TREC, T-cell receptor excision circles; OS, overall survival.
Low levels of TREC correlate to increased GVHD incidence in acute lymphocytic leukemia patients
In patients with acute lymphocytic leukemia (ALL), there was a significant correlation between aGVHD I–IV and TREC levels at 6 and 9 months post-transplantation. Individuals with a TREC value lower than the median had significantly higher incidence of aGHVD (6 months P<0.001 and 9 months P<0.02) (Fig. 2). No significant correlation was found between TREC levels and OS, RFS or incidence of relapse (data not shown).

Acute lymphocytic leukemia (ALL) patients. The impact of acute graft versus host disease (aGVHD) on TREC levels at 3, 6, and 9 months post-ASCT.
TREC levels post-ASCT predict the survival rate in patients with chronic leukemia
In individuals with chronic leukemia [CML and chronic lymphatic leukemia (CLL)], there was a significant correlation between TREC levels at 3 months and RFS (P<0.05) and OS (P<0.005) (Fig. 3a, b). No significant correlation was found between TREC levels and aGVHD or relapse incidence at any time point (data not shown).
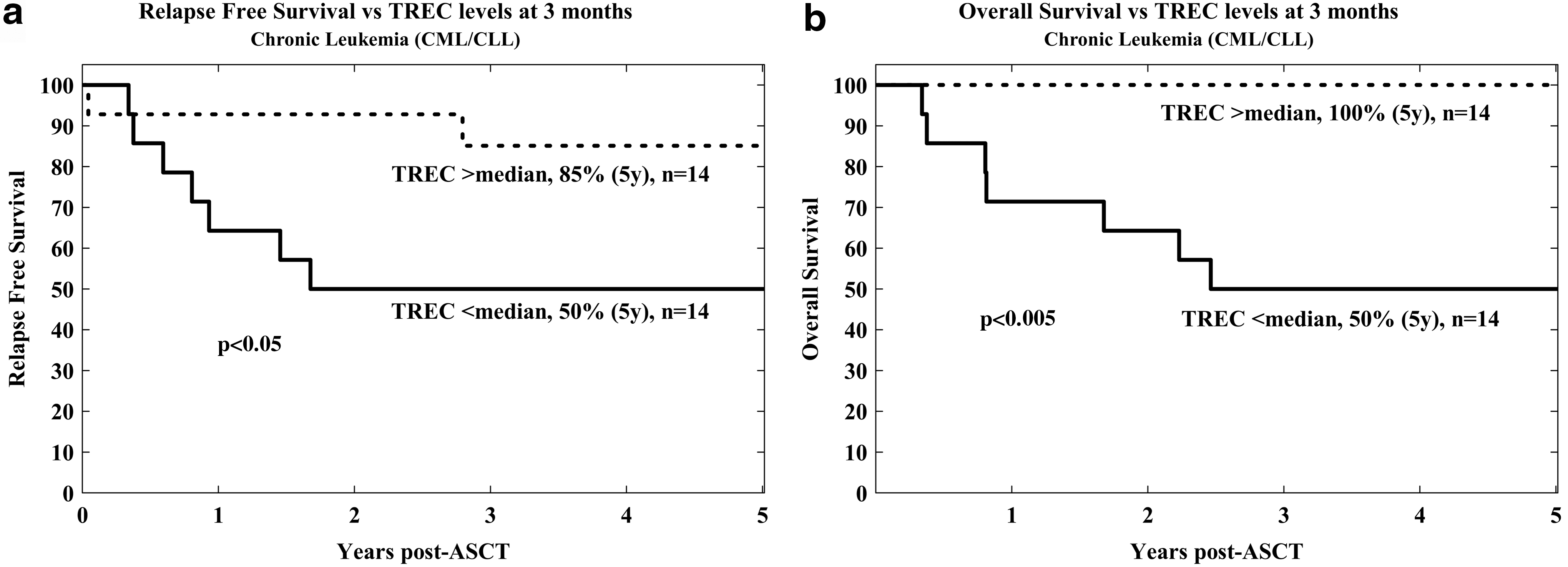
Chronic leukemia patients. RFS
Multivariate analysis for RFS revealed that herpes simplex virus (HSV) reactivation post-HSC transplantation (HSCT) was associated with a decreased RFS (P<0.05) (Table 2). TREC levels above median at 3 months post-HSCT were significantly correlated to an increased RFS (P=0.06). Multivariate analysis for OS for these patients revealed that reactivation of HSV (P<0.05) and varicella zoster virus (VZV) (P<0.05) was associated with a decreased OS. High TREC levels at 3 months post-HSCT could not be included in the multivariate analysis as all patients in that group were alive.
TREC levels post-ASCT in MDS patients predict relapse and long-term OS
In patients with MDS, lower TREC levels at 9 months were significantly associated with an increased risk of relapse (P<0.02) (Fig. 4a). At both 6 and 9 months post-ASCT, lower levels of TREC were associated with a decrease in RFS (P<0.02) (Fig. 4b, c). For OS, there was a significant advantage with higher TREC levels at 6 and 9 months post-ASCT (P<0.05 and P<0.02, respectively) (Fig. 4c, e). Most death in the low-TREC groups were due to relapse after 6 months.
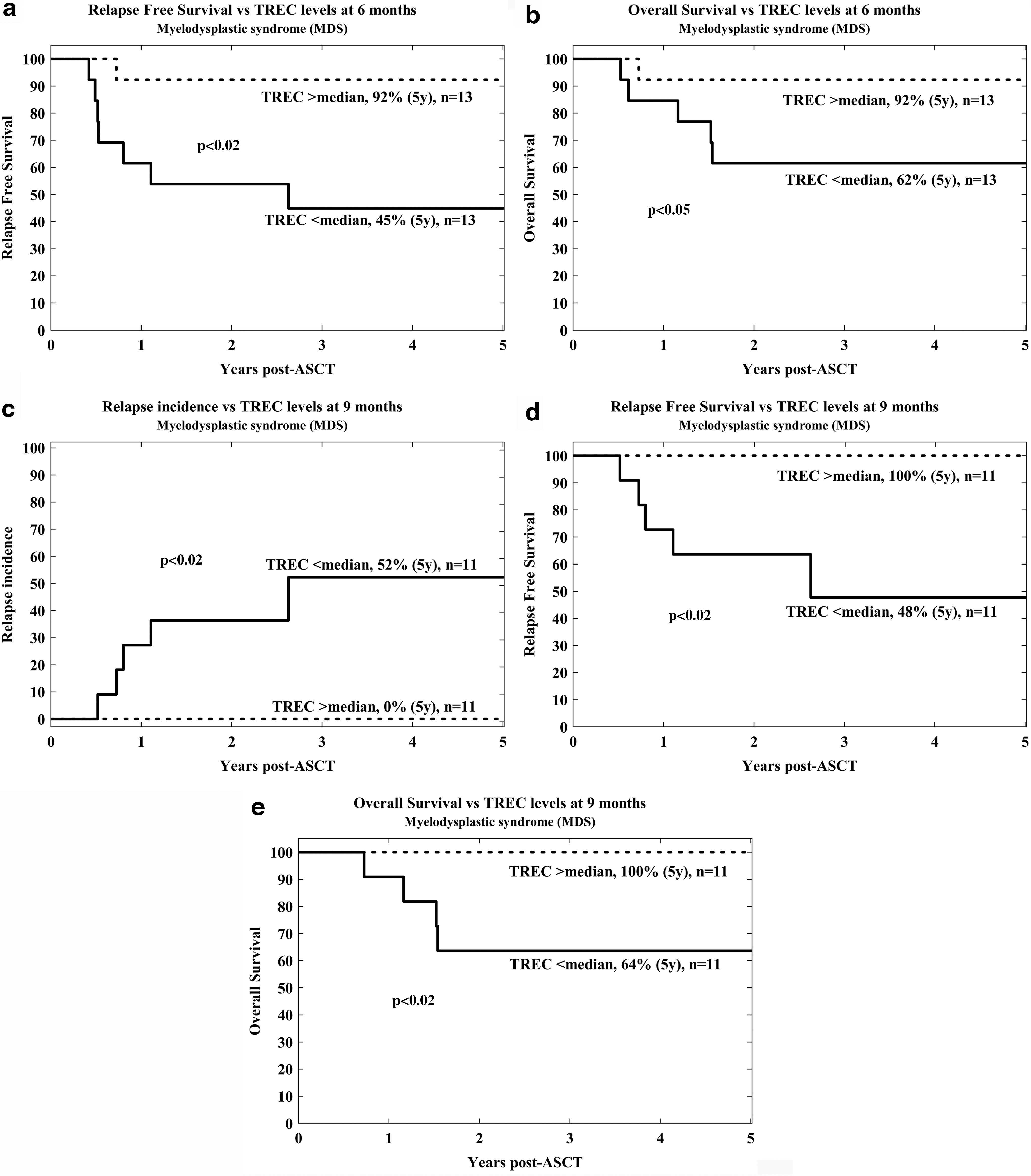
Myelodysplastic syndrome patients. RFS
Multivariate analysis for RFS revealed that nucleated cell dose (P<0.05) and TREC levels above median, 6 months post-HSCT (P<0.02), were associated with favorable prognosis in this patient group (Table 2). TREC levels 9 months post-HSCT could not be included as no patients died in the group containing patients with above median TREC levels. Additionally, in a multivariate analysis for OS in MDS/MPS patients, only a major ABO donor–recipient mismatch was associated with unfavorable prognosis (P<0.05) (Table 2).
Effect of ATG on TREC levels
We have previously shown that ATG significantly decreased TREC levels during the first 6 months post-ASCT [9]. Whereas ATG in itself is also associated with the risk of relapse [23], it is important to adjust the analysis for the patient with or without ATG separately to elucidate the direct effect on the correlation between TREC levels and relapse seen in this patient material. When analyzing only the patients receiving ATG separately for the different disease categories, TREC levels were still significantly associated with relapse and RFS as above (data not shown). For patients without ATG, the same analysis was performed with the same results, except for patients with chronic leukemia and ALL where the numbers were too few. Due to limited patient numbers in the patient subgroups, multivariate analysis was not possible to perform.
Discussion
The critical role of rapid T-cell reconstitution post-ASCT and its links to GVHD and GVL are well known [3,24 –27]. As peripheral blood TREC levels provide an easy, but indirect, measurement of T-cell thymic output, we speculated that their levels might be predictive of relapse after ASCT.
Studies have shown that TREC is a more accurate marker for recent thymic emigrants compared with phenotypic markers such as CD45RA, CCR7, and CD62L [28,29]. In addition, the frequency of cell populations carrying the surface marker CD45RA changes over time due to the ongoing conversion of these cells to CD45RO+ memory [8].
Whereas several studies have associated TREC levels with CMV reactivation, GVHD, TRM, and OS [5,9,12,14,30 –33], no clear correlation has been shown between relapse and TREC levels after ASCT. An association between leukemic relapse and low TREC levels has been suggested, however, no statistical significance was reported possibly due to limited patient numbers [34]. Two recent studies do describe a significant correlation between recovery of thymic function and relapse after T-cell depleted HLA-haploidentical ASCT [16] and unrelated cord blood ASCT [17]. The studied populations consisted mainly of children with ALL and were relatively small.
In this study, the kinetics of TREC levels after ASCT was highly variable and dependent on the primary disease (data not shown). This could be a consequence of the high variability between different diseases as relates to the conditioning regimen and median patient age, both known to significantly impact TREC levels [9,10]. In addition, the preference of different stem cell sources and doses might also influence the development [9,12,30,35,36]. Disease-dependent heterogeneity in thymic reconstitution could be a reason why earlier reports have not shown a convincing association between TREC levels and relapse of the underlying disease [12,13,32]. In an earlier study from our group with partly overlapping patient material, we failed to show any correlation between relapse and TREC levels, but in that study, no subdivision was done between disease indications in contrast to the present study [9]. Clearly, when dividing the patients with malignant disease into subgroups based on ASCT indication, several associations between TREC levels post-ASCT and relapse emerged.
In earlier studies, it has been shown that quicker reconstitution of peripheral lymphocyte levels post-ASCT is associated with an increase in OS in patients with acute leukemia [37,38]. However, these studies do not distinguish between cells originating from the grafts and lymphocytes differentiated in the host from HSCs.
TREC analysis was used as an estimate of de novo differentiation of naive T cells in the different patient groups. Higher TREC levels 2 months post-ASCT correlated to a lower relapse rate and a higher RFS in patients with AML (Fig. 1 and Table 2). This suggests that the presence of newly produced T cells early after ASCT plays an important role in the GVL effect. The fact that low TREC levels in AML patients measured at 2 months are predictive for relapse is of clinical importance. Various treatment options exist at this stage to influence the survival chances in these patients, for example, through tapering of the immunosuppressive therapy or treatment with donor lymphocyte infusions (DLI). We could observe a strong association between a major ABO mismatch and an increased risk of relapse (Table 2). This is in contradiction to several larger studies [39,40]. In an earlier study from our center, we also failed to see this association [41]. Our observed results may be related to a small sample size and should be confirmed in a larger study on only AML patients.
In patients with ALL, low TREC levels were associated with the incidence of aGVHD at 6 and 9 months (Fig. 2). Previous studies have demonstrated that aGVHD and chronic graft versus host disease (cGVHD) negatively affect TREC levels suggesting that low TREC levels are most likely a consequence, and not cause, of early aGVHD [11,12,14,31,42]. Interestingly, patients diagnosed with ALL were significantly younger than those in other groups (median age <20 compared to >40, Table 1). We have previously reported an association between TREC levels and GVHD in younger (<30) individuals [9], in line with the current observations. Of interest is that only in ALL patients (due to the high proportion of children), TREC levels ever reach to levels comparable to normal healthy individuals. For all other patient categories in this cohort, TREC levels stay below normal levels up to 24 months post-HSCT (data not shown).
In patients with chronic leukemia, there was a positive correlation between RFS and OS, and higher TREC levels 3 months post-ASCT (Fig. 3). These data are in line with a previous study on CML patients linking a higher relapse rate with no detectable TREC post-ASCT [43]. This suggests that effective thymic output is important to prevent relapse and improve survival in this patient group (Fig. 3). Furthermore, CML has been shown to be responsive to the GVL effect after DLI treatment [44,45]. This is also in line with our finding where a functional T-cell compartment and its putative GLV effect is of importance to inhibit the leukemic disease.
MDS consists of a heterogeneous group of clonal stem cell disorders of the hematopoietic lineage. Patients are often characterized by ineffective hematopoiesis with consequent cytopenias and a predisposition for transformation to acute leukemia [46]. Today, ASCT is the only potentially curative treatment for patients with MDS, but it is associated with a high relapse risk [47]. Low TREC levels significantly correlated to decreased RFS and OS at 6 and 9 months (Fig. 4). Furthermore, the relapse incidence at 9 months correlated to low TREC levels. This is of interest as it is well known that these patients seldom respond to the added GVL effect of DLI [48]. That a GVL effect from T cells is still exerted by the allograft, can be seen through the fact that patients with low TREC levels have a lower RFS (Fig. 4). In addition, most deaths in the low TREC group are due to relapse (Table 2). These data suggest that reconstitution of a functional immunity after HSCT is vital for a sustainable control over malignant MDS clones. Whether this is a direct effect exerted by the thymus-derived T cells or a consequence of functional hematopoiesis inhibiting the growth of malignant clones through space limitation is unclear.
In this study, we have shown that TREC monitoring can be a powerful tool to predict relapse after ASCT, especially in patients with AML and MDS. Low TREC levels may be a future indication for early immunological interventions, for example, DLI or tapering of immunosuppression to decrease the risk of relapse.
Footnotes
Acknowledgments
This study was supported by the Swedish Childhood Cancer Foundation, The Swedish Research Council (VR), the Swedish Society for Medical Research (SSMF), the Stockholm County Council, and Karolinska Institutet.
Author Disclosure Statement
The authors have no conflicts of interest to declare.