
Abstract
Ischemic diseases are the major cause of death and morbidity in Western countries. In the last decade, cell therapy has been suggested to be a promising treatment both in acute/chronic myocardial and peripheral ischemia. Different cell lineages have been tested, including endothelial progenitor cells. A subpopulation of bone marrow-derived immature ECPs, expressing the highly conserved stem cell glycoprotein antigen prominin-1 or CD133 marker, was shown to possess pro-angiogenic and antiapoptotic effects on ischemic tissues. The mechanisms implicated in CD133+ cells ability to contribute to neovascularization processes have been attributed to their ability to directly differentiate into newly forming vessels and to indirectly activate pro-angiogenic signaling by paracrine mechanisms. A large body of in vivo experimental evidences has demonstrated the potential of CD133+ cells to reverse ischemia. Moreover, several clinical trials have reported promising beneficial effects after infusion of autologous CD133+ into ischemic heart and limbs exploiting various delivery strategies. These trials have contributed to characterize the CD133+ manufacturing process as an advanced cell product (AMP). The aim of this review is to summarize available experimental and clinical data on CD133+ cells in the context of myocardial and peripheral ischemia, and to focus on the development of the CD133+ cell as an anti-ischemic AMP.
Introduction
D
The aim of this review is to summarize available experimental and clinical data on CD133+ cell in the context of myocardial and peripheral ischemia, and to focus on the development of the CD133+ cell as an advanced medicinal anti-ischemic product.
Biological Properties of CD133+ Cells
Discovered in 1997 from mouse footpads immunized with human fetal liver CD34+ cells [4], CD133 is a highly conserved stem cell glycoprotein antigen, described as marker for identification of early immature endothelial progenitor cells (EPCs) [5].
Regardless of their origin—BM versus peripheral blood (PB) versus umbilical cord blood (UCB)—the CD133+ cells phenotype invariably indicate the presence of early immature EPCs as identified by the different coexpression of CD133+/KDR+/CD34+ surface markers, according to their differentiation status [3,6 –8].
After positive immune-magnetic selection, CD133+ cells do not express [5,7,9], or express at very low level [3,8] markers of endothelial differentiation, such as vWF, CD31, Ulex-1, CD146, or CD144, whereas frequently express the hematopoietic antigen CD45 [3,10 –13] and mesenchymal markers such as CD105 and CD90 [7,14 –16]. After endothelial differentiation, these cells lose the EPC markers, maintain low levels of hematopoietic markers, and acquire the expression of adult endothelial cell markers (CD31+, CD144+, KDR+, Tie-2+, vWF+, DiIAcLDL+, Flt-1, and CD146+).
Since 2001, in vitro evidence has been provided on migratory and angiogenic properties of CD133+ cells, along with the ability of this cell subpopulation to trans-differentiate into mature cardiovascular-related lineages such as endothelial cells (Table 1).
BM, bone marrow; ED, endothelial differentiation; G-CSF, granulocyte colony-stimulating factor; HUVECs, human umbilical vein endothelial cells; IL, interleukin; mPB, mobilized peripheral blood; NA, not available; PB, peripheral blood; PDGF, platelet-derived growth factor; UCB, umbilical cord blood; VEGF, vascular endothelial growth factor.
CD133+ cells are able to migrate upon vascular endothelial growth factor (VEGF) and stromal-derived factor [8,17] gradients in vitro and in vivo [18]. As for their angiogenic ability, CD133+ cells act in vitro both directly through differentiation into endothelial cells and indirectly through the paracrine release of an angiogenic cytokine pool. Differentiated CD133+ cells were shown capable to induce in vitro capillary tubes formation [7,10,16,17,19]. Using a three-dimensional collagen gel culture system, the hematopoietic stem and progenitor cell marker CD133 has been detected during angiogenesis both in early and in later stages of culture. Moreover, CD133+ cells have been found in newly formed capillary tubes from aortic explants in vitro [20]. Interestingly, CD133-expressing cells have been found in the neo-endothelial monolayer of left ventricular (LV) assist device surface 1 month after implantation, revealing the ability of this cell type to actively contribute to vascular remodeling in vivo [8]. Very recently, Adini et al. [21] showed the critical role of CD133 protein for endothelial cells growth, through regulation of proliferation and angiogenesis, and by interacting with the VEGF family.
A consistent body of knowledge exists on the indirect angiogenic and protective effects conferred through a variegated cocktail of substances released in a pacracrine manner by CD133+ cells upon ischemic conditions. In particular, it has been shown that CD133+ cells secrete in vitro notable bioactive angiogenic [angiopoietin-2, b-FGF, VEGF, EGF, HGF, and granulocyte colony-stimulating factor (G-CSF)], morphogenic (BMP), pro-inflammatory [RANTES, interleukin-6 (IL-6), IL-8, and GRO], anti-inflammatory (IL-10), and anti-apoptotic (IGF-1) molecules, along with matrix-remodeling factors including different metalloproteinase and their inhibitors (MMP-1, MMP-3, MMP-9, TIMP-1, TIMP-2, and TIMP-4) [12,13,17,22 –24], which synergistically concur to reduce tissue damage after ischemia. Table 1 shows immunophenotype characterization, endothelial differentiation markers, and cytokine assays in available literature.
Much more debate exists on cardiomyocyte differentiation ability of EPCs [25]. Available evidence shows that trans-lineage commitment of EPCs to cardiomyocyte is not a common differentiation cascade, even if frequency seems higher compared to cell fusion [26 –31]. Specifically, only few groups have focused on CD133+ cardiomyocyte lineage commitment. Ma et al. did not find element of cardiomyocyte-like differentiation in vitro neither with BM-derived nor with UCB-derived CD133+ cells [10]. On the other hand, a cardiac phenotype, characterized by positive immunostaining with antibodies against troponin I, cardiac MHC, and myosin ventricular heavy chain, was shown in vitro after CD133+ cell culture in cardiomyogenetic conditions [7,32,33]. In an attempted to identify in vivo trans-differentiation of human CD133+ cells 4 weeks after injections in ischemic rats, Leor et al. demonstrated that engrafted cells were negative for cardiomyocyte (troponin and sarcomeric actin) and endothelial (CD31 and vWF) markers [34,35]. More recently, Avitabile et al. showed the ability of UCB CD34/CD133+ cells to acquire in vitro cardiac functional features through cell fusion with neonatal cardiac myocytes [36].
Notably, far to be elucidated as well is the complex interaction between EPCs activity and the inflammatory response present in the early phase of acute ischemia [37]. It has been proposed that inflammatory stimuli have a beneficial effect on EPCs, promoting endothelial differentiation [38], enhancing angiogenic response [39], and inducing a rapid release of EPCs into the circulation [40]. On the other hand, inflammation-derived factors like CRP, TNF-alpha and IL-1β inhibit survival differentiation and decrease survival of EPCs [40,41]. No information in this regard is to date available for CD133+ cells. Equally, there are at present no data conclusively demonstrating the capability of CD133+ subpopulation to recruit resident cardiac stem cells (CSCs) under ischemic conditions through a paracrine mechanism already described for EPCs [42], although CD133+ cells can produce the whole cytokine cocktail required to promote migration, growth, and differentiation of CSCs (Table 1) [43 –46].
Figure 1 summarizes the different mechanisms implicated in CD133+ cells-mediated cytoprotection and tissue restoration upon ischemia.
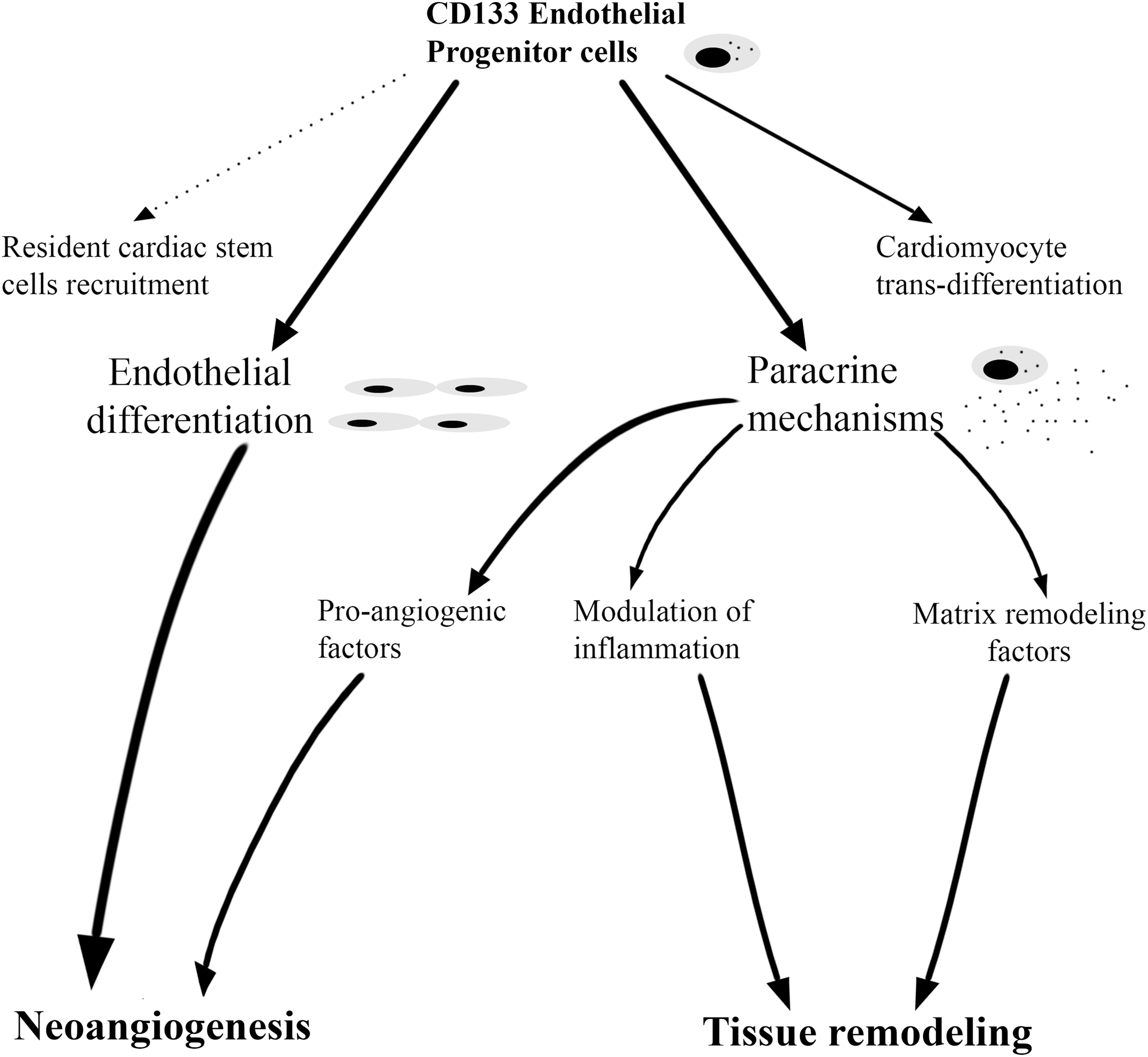
Principal mechanisms implicated in the reported anti-ischemic effects conferred by CD133+ cells.
CD133+ Cell Delivery in Animal Models of Ischemia
Several preclinical studies in small and large animal models of myocardial and peripheral ischemia have tested safety and efficacy of CD133+ progenitor cells administration.
Safety considerations
At present, in more than 300 animal experiments including mice, rats, and pigs, a single administration of autologous or allogeneic CD133+ cells was not reported to provoke any local or systemic adverse reaction (Tables 2 and 3). No evidence of ectopic tissue formation, including benign cell growth, has been described in the literature, nor cardiac/muscular inflammation, edema, and calcifications. As reported by Das et al. [47] in a rodent model of ischemic myocardial injury, intramyocardial injection of human-derived expanded CD133+ cells was not related to significant increase in oncogenic molecules such as PTEN, AKT, p38, and others. To our knowledge, no information is available on the effects of repeated administrations.
AMI, acute myocardial infarction; CMI, chronic myocardial infarction; EPC, endothelial progenitor cells; EXP, nanofiber expanded cells; FU, follow-up; IC, intracoronary; IM, intramyocardial; IV, intravenous; LVEDV, left ventricular end diastolic volume; LVEF, left ventricular ejection fraction; MSCs, mesenchymal stem cells; SM, skeletal myoblasts; SVEC, saphenous vein endothelial cells; VIP, VEGF plus PDGF overexpressed stem cells.
HLI, hind limb ischemia; i.m., intramuscular; IV, intravenous.
Myocardial ischemia
Both rodent and large animal models have been employed to analyze the potential of CD133+ progenitor cells in acute and chronic myocardial ischemia settings (Table 2). In a rat model of acute myocardial infarction (AMI), Kocher et al. [34] demonstrated for the first time the ability of human-derived-CD34+-coexpressing CD133+ cells to reduce the fibrotic area, collagen deposition, and myocytes apoptosis after coronary ligation, and to increase capillary density and improve cardiac function as measured by left ventricular ejection fraction (LVEF). Of note, cardiac function improvement persisted up to 15 weeks after stem cells transplantation and no increases in capillary numbers at sites distal to the infarct zone was observed. In the same study, authors reported the formation of new vessels involving endothelium of both human and rat origins, confirming the ability of the human CD133+ to differentiate in vivo in endothelial cells and to integrate in neovascularization processes. Similarly, Ma et al. [10] showed that intramyocardial injection of human purified CD133+ cells after cardiac cryo-injury was able to stimulate neoangiogenesis. Notably, BM-derived-CD133+ cells but not UCB-derived CD133+ cells were able to ameliorate myocardial contractility and prevent cardiomyocytes apoptosis. More recently, a rat model of AMI [48] confirmed the ability of intravenously infused human-derived CD133+ cells to infiltrate the infarcted area and to improve myocardial function. No difference was observed between expanded and nonexpanded CD133+ cells [48], suggesting that an extensive cell manipulation is not mandatory to achieve an adequate angiogenic potency. Furthermore, these cells have been detected into the heart up to 14 days after delivery, in the absence of adverse events.
To closely mimic the clinical scenario of ischemic cardiomyopathy, different works [35,47,49,50] induced in rats and pigs a chronic myocardial infarction (CMI) followed by both intravenous and intraventricular CD133+ cells injections 5–10 days after onset. As clearly demonstrated by Das et al. [47], the CD133+-group showed to be associated with the promotion of neovascularization into the ischemic heart tissue, the improvement of systolic function, and the overexpression of pro-angiogenic factors, such as VEGF and platelet-derived growth factor.
Cell biodistribution studies showed survival and nesting of transplanted cells into the ischemic heart. By microscopic examination, Leor et al. [35] demonstrated in a rodent model of CMI that UCB-derived CD133+ cells were able to migrate, colonize, and survive in the cardiac-infarcted tissue even 1 month after infusion. In pigs, magnetically labeled CD133+ cells were successfully tracked and visualized in the host myocardium with both, magnetic resonance imaging (MRI) and echocardiographic imaging, 2 months after transplantation [50 –52]. Noteworthy, LVEF and infarct volume of treated animals were considerably improved with respect to untreated animals [50].
In summary, experimental studies of acute and CMI showed scar size reduction and improvement of LV systolic function following CD133+ cells administration via indirect angiogenic and cytoprotective mechanisms.
Limb ischemia
Several hind limb ischemia (HLI) murine models investigating different routes of administration and cell dosing [12,53,54] have been tested. We were among the first to report that human UCB-derived CD34+-coexpressing CD133+ cells had the potential to differentiate into endothelial cells in vitro and to enhance in vivo the arteriole length density in a rat model of ischemic adductor muscles [53]. Yang et al. intravenously inoculated UCB-purified CD133+cells reporting a marked improvement of perfusion and limb salvage rate, superior to that obtained with not purified human umbilical vein endothelial cells [54]. Along with neoangiogenesis promotion, CD133+ cells demonstrated to accelerate wound healing in diabetic mice via higher wound capillarization and by reduction of apoptosis, thanks to a paracrine effect exerted by secretion of ILs, growth factors, and chemokines [23]. The paracrine hypothesis has been subsequently confirmed as the main angiogenic mechanism in several in vivo preclinical models of peripheral ischemia [12,13,23,54,55]. More controversial is the ability of CD133+ cells to trans-differentiate into new functional endothelial cells. In a dose escalating study [13], labeled CD133+ cells (1×105 cell dose) could not be detected in a model of murine HLI and in the group receiving 1×106 cell dose less than 1% of infused cells were localized into ischemic vessels. In summary, these studies demonstrated in vivo that only a small proportion of CD133+ cells have the capacity to integrate into the blood vessels of ischemic muscles and that the remaining cells act indirectly stimulating neovascularization through a paracrine mechanism.
To address the issue about the optimal delivery route, the direct intramuscular (i.m.) injection and the systemic intravenous delivery were evaluated in different studies demonstrating comparable proangiogenic effect and similar engraftment rate of transplanted cells within the target tissue (Table 3). In a rat hind limb model of ischemia [19], IM injections of human-derived CD133+ cells lead to vascular density increase compared with a control group. Further, the colocalization of human CD31+ endothelial marker within ischemic tissue at 2 weeks demonstrated both retention and differentiation into mature ECs of intramuscularly injected CD133+cells. Following intravenous administration, Yang et al. [54] was able to visualize labeled UCB-CD133+ cells into the limb ischemic area and the colocalization of human and mouse labeled cells 7 days after ischemia. No fluorescence positivity was found from other remote tissues. Interestingly, the sole report directly comparing the efficacy of the IM and intravenous administration routes concluded that both approaches lead to similar results in terms of blood flow recovery and capillary density [55].
Conclusions
In conclusion, irrespective of progenitor source, adequate evidence has been provided of beneficial effects ensued from both UCB and BM-derived CD133+ cells delivered in vivo under different ischemic conditions. In animal models of MI, it was invariably demonstrated that the injection of CD133+ cells improved LV function and reduced fibrotic areas, whereas HLI models showed a significant improvement in blood flow recovery and limb salvage.
Clinical Experience
The worldwide clinical experience with CD133+ cells in a setting of ischemia encompasses to date more than 250 patients enrolled in controlled phase I and II clinical studies to received cell therapy for acute or chronic myocardial ischemia through intracoronary (IC) or intramyocardial (IM) approaches and for chronic critical limb ischemia (CLI) through intramuscular (i.m.) approach (Table 4).
↑, increase; ↓, decrease; ↔, no change.
AE, adverse event; CABG, coronary artery bypass grafting; CCS, Canadian Cardiovascular Society, grading of angina pectoris; CLI, critical limb ischemia; IHD, ischemic heart disease; IHF, ischemic heart failure; i.m., intramuscular; IMendo, intramyocardial endocardial; IMepi, intramyocardial epicardial; MACE, major adverse cardiac events; MRI, magnetic resonance imaging; NR, nonrandomized; NYHA, New York Heart Association Functional Classification; PET, positron emission tomography; PSySR, peak systolic strain rate; R, randomized; RC, randomized controlled; RDB, randomized double-blinded; RPCDB, randomized placebo controlled, double-blind; RSB, randomized, single blind; SPECT, single photo emission computed tomography; ɛet, strain during ejection time; ɛmax, maximum strain during cardiac cycle.
Myocardial infarction
So far, the clinical experience with autologous CD133+ progenitor cells in a setting of MI is still limited. Table 4 summarizes the features and major findings of published trials. The first experience was reported in 2005 by Bartunek et al. [56] with a phase I/II, controlled nonrandomized trial, in which BM-derived CD133+ cells were IC delivered 10 days after ST-elevated myocardial infarction (STEMI) in patients with compromised LV function after successful coronary stenting. Authors reported a benefit in terms of LV function and perfusion at 4 months follow-up as assessed by echocardiography, single photon emission computed tomography (SPECT), and positron emission tomography (PET). However, in the treated group only, a modest increase of stent restenosis was reported. Colombo et al. [57] enrolled 15 patients to receive, within 14 days after STEMI, BM-derived CD133+ cells versus mobilized peripheral blood (mPB) CD133+ cells versus standard medical therapy. In the absence of safety concerns, only BM study group demonstrated myocardial blood flow improvement (+10%) measured with cardiac dynamic PET scans 12 months after treatment. A trend toward reduction of infarct size was observed in both mPB and BM cell groups. Despite the small number of patients included in this study, cell treatment was considered safe and feasible. More recently, the randomized, double-blind, placebo-controlled phase II COMPARE-AMI study [58,59] has published 1 year ongoing follow-up data [60]. This study is aimed to compare IC administration of BM-derived CD133+ cells with a placebo group in 40 patients with STEMI and LV dysfunction after successful PCI. The trial was designed to establish the safety profile of the procedure and efficacy in terms of improvement of cardiac function. To date, 20 patients completed 1-year follow-up [60] and the preliminary analysis revealed no major concerns about safety in terms of major cardiac events such as death, recurrent MI, malignant ventricular arrhythmias, or restenosis. As for LV function, available echocardiographic data showed a relevant improvement of the LVEF at 4 and 12 months after the procedure. Of course, more definitive conclusions on CD133+ cell efficacy will be drawn once this trial will be completed.
In summary, available studies of IC injection of CD133+ cells in STEMI have confirmed feasibility and safety, although larger trials are needed to establish the therapeutic potential. Two randomized controlled phase II studies powered to draw meaningful data about the functional benefit of CD133+ cells treatment after MI (SELECT-AMI, Identifier: NCT00529932 and ESTABOMA trial, Identifier: NCT01748383) are currently actively enrolling (Table 5).
EF, ejection fraction.
Refractory angina
Despite progressive improvements in revascularization procedures and pharmacological therapies, a nonnegligible population of patients suffers refractory “no option” angina [61]. Small pilot phase I trials have been designed to explore the hypothesis that the administration of CD133+ cells could relieve angina symptoms and improve cardiac performance and regional myocardial perfusion in territories with reversible ischemia (Table 4). Klein et al. [62] provided the first evidence that the stand-alone epicardial injection of CD133+ cells was feasible and safe and shows the potential to improve symptoms and cardiac function as assessed by cardiac MRI in 10 patients with refractory angina. In a nonrandomized pilot study, we [63] enrolled five patients with untreatable angina to receive direct intramyocardial injection of BM-derived CD133+ cells in areas of reversible ischemia identified by SPECT. At 6 months follow-up, the number of segments with stress-inducible ischemia per patient significantly decreased (from 5.6±2.8 to 2.4±2, P<0.01). Moreover, 6-months angina improvement was found at 1 year to be unchanged in four out of five patients. To date, the epicardial delivery route via minimally invasive surgical approaches has been the preferred strategy in this clinical context. Adler et al. [64] were the first to perform cell infusion via IC route in nine patients with class II–IV angina. They have tested safety of three different cell escalating-doses of autologous CD133+ cells (1×106, 2×106, or 3×106 respectively), which were all well tolerated without side effects. At 12 months postoperatively, authors reported that cell infusion modestly but significantly increased angina stability and reduced areas of reference ischemia by SPECT analysis.
Altogether, available data are still preliminary and suggest clinical improvements in the absence of relevant side effects. Notably, two phase I and two phase II randomized controlled trials are currently going on (Table 5). The phase I study coordinated by Woo Yi-Ping J. (
Chronic ischemic heart failure
More evidence toward the ones for STEMI and refractory angina is now available in patients dealing with chronic ischemic cardiomyopathy. Overall, 84 patients were included in phase I studies in which cells were infused using IC delivery as a stand-alone therapy. In one study only, cells were epicardially injected into the border zone of the infarcted myocardium in combination with coronary bypass grafting [65,66]. These trials confirmed feasibility and safety of the procedures in the absence of side effects such as ectopic tissue formation and cardiac arrhythmias as assessed by echocardiography and electrocardiogram monitoring. In three studies, patients received G-CSF mobilization of PB-derived CD133+ cells before harvesting [67 –69]. In this context, side effects reported such as myalgia and thrombocytopenia were primarily associated with BM stimulation rather than to cardiac cell therapy, which was always well tolerated.
To address the issue of local and remote bio-distribution of delivered cells, four small uncontrolled phase I trials have been conducted to track labeled CD133+ progenitor cells before injection with commercially clinical-grade radionuclides. The most consistent data have been recently published by Koutelou and coworkers [70], in which 13 patients with old anterior MI were included to receive IC infusion of stem cells labeled with Tc-99m-hexa-methyl-propylene-amine-oxime (HMPAO). The comparison between images obtained by gated-SPECT before and 1 h after IC infusion showed persistence of delivered cells in the infarcted area ranging from 56.4% to 97.2%. However, according to other published data [71,72], most cells appear to disappear within few days after injection [68,69].
As for preliminary efficacy, eight phase I and three phase II studies enrolling 175 patients cumulatively, suggested a partial or complete restoration of global LV function and improvements in myocardial perfusion (Table 4). Stamm and coworkers [66] prospectively enrolled 40 patients to be randomly assigned to CABG and CD133+ cells or CABG alone. After 6 months, LVEF of cell therapy group was significantly higher by 10% in relation to patients undergoing CABG alone. Interestingly, a subgroup analysis showed a relevant positive correlation between poorly depressed preoperative function (LVEF<35%) and the gain of LVEF after 6 months (mean of 15.3% improvement). The long-term safety follow-up (up to 9 years) [73] showed no side effects in terms of tissue changes, malignant or sustained ventricular arrhythmias. Notably, patients with depressed preoperative cardiac function confirmed to be the best responders to cell therapy even after 5 years. Similarly, 5-years results from the Ahmadi study group [74] showed a good safety profile of BM-CD133+ cells implantation after CABG and demonstrated improvement in cardiac and clinical performance as indicated by regional wall motion and New York Heart Association Functional Classification class. In a very recent phase II randomized trial (CARDIO133) [75], 60 patients with chronic ischemic heart disease were randomized 1:1 to undergo either CABG and injection of CD133+ in the infarcted border zone or CABG and placebo injection. Although some improvement in infarct size and myocardial perfusion were detected 6 months after treatment, the global LV function and clinical symptoms did not change in the CD133-group compared to placebo.
Using an IC approach, Manginas et al. [76] reported a controlled study of infusion of CD133+ cells in 24 patients with old nonviable anterior MI. Treated-group exhibited significant reduction in LV end-diastolic and end-systolic volumes compared with controls, and a mild but statistically significant increase in LVEF (2.5%).
Notably, chronic myocardial ischemia is the target condition in five actively enrolling trials (Table 5). Recently, a randomized, prospective, double-blind study investigating the implantation of autologous CD133+ stem cells in patients undergoing CABG (IMPACT-CABG,
Critical limb ischemia
The vast majority of clinical studies regarding cell therapy in patients dealing with peripheral ischemic disease reported BM-mononuclear cell (MNC) administration rather than specifically selected cell populations. The Therapeutic Angiogenesis using Cell Transplantation (TACT) study [78] was one of the first demonstrating the efficacy of i.m. administration of BM-MNCs in “no-option” patients with CLI. Interestingly, a post hoc subgroup analysis of this trial concluded that best CLI responders presented an increased number of circulating CD34+/CD133+ cells 1 month after cell transplantation [79]. In 2007, purified CD133+ cells delivery from mPB was described for the first time in a case report by Canizo et al. [80]. Afterward, Burt et al. [81] enrolled nine patients in which CD133+cells were positively selected from PB and intramuscularly injected in limb ischemic areas. There were no side effects or adverse events and lower extremity salvage was reported for seven out of nine treated patients. Given the modest clinical experience, further studies are obviously required to validate safety and feasibility of CD133+ cells delivery in CLI.
Four ongoing trials (three phase I and one phase II) are actively enrolling (Table 5). The SCRIPT-CLI trial (
Conclusions
Cumulatively, phase I (14 studies) and randomized phase II (5 studies) clinical trials have demonstrated safety and preliminary efficacy of CD133+ cells administration into the heart, and cell tracking analyses have shown the ability of these progenitors to home into the injured myocardium. The large majority of completed early-phase trials concur that CD133+ cells injection is safe in the early and long-term follow-up and yielded preliminary clinical and functional benefits, irrespective of the delivery strategy. The clinical experience in CLI is still limited, although no safety concerns have been raised. The validation of these data with adequately powered controlled trials is expected in the near future.
Considerations on CD133+ Cell Compliancy as an Advanced Therapy Medicinal Product
The translational pathway from basic research to the application of a clinical-grade cell product [according to the definition of Advance Therapy Medicinal Product (ATMP)] is strictly regulated by United States- and Europe-based principal regulatory agencies, such as EMA and FDA [82]. Manufacturing clinical-grade cells with appropriate quality standards requires a process of purification, characterization, minimal or extensive manipulation, transport, and delivery according to operative procedures belonging to the “Good Manufacturing Practices” (GMP) [83] regulation. In the cardiovascular field, different autologous and allogeneic cell products have been characterized as ATMPs, either with minimal or more extensive manipulation [84]. The largest experience has been reported with BM-derived MNCs in a context of acute and chronic myocardial ischemia [43]. Other BM-derived cell types, including mesenchymal or positively selected CD34+ and CD133+ cells, have been similarly tested upon adequate manufacturing standards [85]. In November 2011, the Committee for Advanced Therapies (CAT) of the European Medicines Agency (EMA) published two scientific recommendations concerning the classification of autologous BM-MNCs and autologous BM-derived CD133+ cells intended for the treatment of ischemic heart disease, post-AMI and in chronic ischemic heart disease as ATMPs [86,87].
Our group was one of the first to report the validation process required to translate in GMP-compliant conditions human BM-derived CD133+ cells as an autologous ATMP in the cardiovascular scenario [12]. In our opinion, the manufacturing process of CD133+ cells is appealing for different features, including the minimal manipulation required, a closed and standardized selection strategy and the relatively fast process from harvesting to inoculation (<24 h). In a perspective of a scalable therapy, a standardized cell manufacturing process with specific threshold values is mandatory. The standard operative procedures (SOPs) we have finalized for the clinical translation of the CD133+ cell product, such as quality controls including purity, microbiological safety, and viability tests, have been precisely set up on the basis of our preclinical and pilot clinical experiences [12,63]. The following threshold values for batch release have been defined: purity >70%, viability >80%, and cellularity between 1 and 12×106 cells. These standards will be applied for an ongoing registered clinical study of autologous CD133+ cell administration in patients with chronic ischemic refractory cardiomyopathy (RECARDIO trial,
Discussion
The whole body of evidence we have reported in this article indicate that the BM-derived CD133+ cell is a subpopulation with a high potential for therapeutic angiogenesis, and cardiovascular tissue restoration. The mechanisms implicated in CD133+ cell's ability to contribute to neovascularization processes have been attributed to both their ability to directly differentiate into newly forming vessels and to indirectly activate pro-angiogenic signaling by paracrine mechanisms. In addition, CD133+ cells contribute to cardiovascular protection upon ischemia by modulating inflammation and matrix remodeling.
This body of knowledge makes the CD133+ cell one of the most characterized cell-based anti-ischemic ATMPs. Available experimental data fully comply with the required regulatory level of evidence of a safe and reliable translation from cell biology to a therapeutic product. Of note, different animal models employed in an acute or chronic ischemia setting have invariably reported a safe systemic and local profile and a specific anti-ischemic effect. Furthermore, clinical data suggest a preliminary salutary effect either from a symptomatic or a functional standpoint in cardiac and peripheral severe pathologic conditions, such as refractory ischemic cardiomyopathy or critical chronic limb ischemia.
Other analogous BM-derived cell products, in particular mononuclear unselected or selected CD34+ cells, have shown a competitive profile in terms of manufacturing process and potency in similar clinical settings [93 –95]. At present, no conclusive evidence is available on cell type superiority. In particular, no consensus has been reached on the opportunity to select cell subpopulations to increase angiogenic potency [96]. The rationale behind positive BM-derived cell selection was the avoidance of the injection of a mixed blend of hematopoietic cells, which may give rise to an unwanted inflammatory response in the target ischemic area [97].
It is worth to note that, irrespective of the BM-derived cell type and despite the large body of experimental and clinical data, some features related to cell potency remain still not elucidated. In particular, the cell-dosing issue has been not yet comprehensively addressed. Such data are difficult to be drawn from clinical studies, given the fact that with closed cell selection strategies as for the CD133+ fraction, the cell number obtained and inoculated in each single patient is usually equivalent. There is probably at this stage a translation lack of dose-escalating studies in large animal models adequately powered to inform the clinical application. As for the CD133+ cell, in the absence of robust preclinical indications, we were the first to tentatively set up dose-finding using a historical cohort of patients.
A second issue is the postmanufacturing validation of potency data. Potency studies are in fact usually conducted in animals before the cell product has been released upon GMP-compliant SOPs. In our CD133+ cell validation protocol, a second round of experiments has been provided using GMP-released human cells to confirm that the angiogenic capacity was not modified by the manufacturing process [12]. To our knowledge, these validation standards have not been reported for other cell types, although required at a regulatory level.
In the last decade, much effort has been done in the search of a thorough explanation of the mechanisms of action of cell therapy [98]. In the cardiovascular arena, with particular regard to ischemia, cell ability to act as pro-angiogenic, antiapoptotic, and cytoprotective agents has been mainly related to the “paracrine hypothesis,” according to which transplanted cells are able, upon ischemic conditions, to produce and release in a feature of “mini-bio-pumps” key active factors, such as cytokines and chemokines [99,100]. In this regard, enough evidence has been provided by us and others that both in vitro and in vivo the CD133+ cell is particularly prone to induce angiogenesis under ischemia. Moreover, a recent randomized controlled study reported that the IC inoculation of CD133+ and CD34+ cells is able to increase the mobilization of BM-derived progenitor cell in the PB of patients with ischemic heart disease even after 6 and 12 months from infusion, suggesting a boost of the physiologic mechanism of tissue repair [101].
These insights are strictly related to the issue of cell biodistribution and trans-differentiation, given the fact that there is evidence provided by cell tracking studies in vivo that, once inoculated into the ischemic tissue such as the infarcted heart, most BM-derived cells disappear within few days after injection. The CD133+ cell is not an exception to this rule [68,69,102]. There is very limited evidence of a long-term persistence of transplanted CD133+ cells in an undifferentiated state or after differentiation into endothelial cells or cardiomyocytes. Of note, from a regulatory standpoint, this issue in our opinion has to be carefully weighted, since the lack of in vivo differentiation, along with the minimal manipulation process required for cell procurement and selection, may in future switch the regulatory CD133+ cell framework from ATMPs to cell transplant.
Clinical data available indicate that CD133+ cells have the potential to be introduced in the clinical arena as an anti-ischemic agent. If compared to the CD34+ cell lineage, the CD133+ cell appears to be positioned at an equivalent stage of clinical development. Both cell types have overlapping biological features and a solid preclinical background in terms of angiogenic effect [103,104]. It is worth to note that these cell products are currently object of investigation of large phase III actively enrolling trials (RENEW for CD34+ and PERFECT for CD133+), powered to obtain confirmative clinical data in a context of refractory cardiomyopathy [105,106]. It is conceivable that in few years new knowledge will be available in this regard. As for CLI, more data from confirmative controlled trials are probably required to advance the CD133+ cell toward a clinical development.
In conclusion, this work has provided a comprehensive body of evidence that the CD133+ cell may be considered as a therapeutic agent when designing cell therapy clinical studies aimed to treat severe ischemic conditions. The number of ongoing actively enrolling phase II and III trials will provide in the next future enough information about the potential of the CD133+ to be part of the clinical anti-ischemic armamentarium.
Footnotes
Author Disclosure Statement
No competing financial interests exist.