
Abstract
Intervertebral disc degeneration is associated with low-back pain. Mesenchymal stem cells (MSCs) have been used to “regenerate” the disc. The aim of this study was to perform a systematic review of comparative controlled studies that have assessed the safety and efficacy of using MSCs for disc regeneration. Literature databases were extensively searched. Trial design, subject-type, MSC sources, injection method, disc assessment, outcome intervals, and complication events were assessed. Validity of each study was performed. Twenty-four animal studies were included with 20.8% of the studies reporting randomization of groups. Trials in humans fulfilling inclusion criteria were not noted. The studies represented 862 discs that were injected with MSCs and 1,603 discs as controls. All three types of MSCs (ie, bone marrow, synovial, and adipose tissues) showed successful inhibition of disc degeneration. Bone-marrow-derived MSCs demonstrated superior quality of repair compared with other non-MSC treatments. A 2.7% overall complication rate was noted, whereby complications were noted only in rabbits. Overall, evidence suggested that MSCs increased disc space height in the majority of animal models. This is the first systematic review to assess the safety and efficacy of MSCs for the treatment of disc degeneration. Short-term MSC transplantation is safe and effective; however, additional, larger, and higher-quality studies are needed to assess the long-term safety and efficacy. Inconsistencies in methodological design and outcome parameters prevent any robust conclusions. Human-based clinical trials are needed. Recommendations are further made to improve efficacy, reduce potential complications, and standardize techniques for future studies.
Introduction
L
The intervertebral disc assumes the role of a shock absorber of the spine and accommodates compressive loading forces [15]. The disc consists of a central gelatinous-based nucleus pulposus (NP) and the peripheral annulus fibrosus (AF) [16]. Cells in the NP region reside in proteoglycan-rich extracellular matrix (ECM), which confers the gelatinous and hydrated properties of the collagen-rich matrix of NP. Therefore, this architecture arrangement provides the mechanical tensile strength toward the surrounding AF [17]. When harmonious, the disc facilitates spinal motion and affords protection of the neural elements. Disc degeneration is the progressive process of the loss of structural and functional integrity of the disc and is characterized by chemical changes in water and proteoglycan content [15,16,18 –21]. This sequential process is thought to be associated with a decreased cell number and a change in phenotype of disc cells, eventually leading to functional loss of the disc unit. As degeneration progresses, change in disc volume and shape is noted, together with overloading of adjacent structures (end plates, facet joints, and ligaments) [18,21]. Such degenerative changes may lead to altered spinal motion, potential disc herniation and compression of the nerve roots, and adjacent disc degeneration that may in time become symptomatic [22 –24].
Spinal fusion and disc arthroplasty are treatment options to address pain and disability from discogenic low-back pain [3,25]. However, these can be costly, they require invasive surgical treatment that may in itself present complications, and symptoms may not fully resolve [25 –27]. Additionally, in the case of spinal fusion, motion of the spine is not preserved, which may alter the natural kinematics of the spine. Early in the degeneration cascade, pain medication, local injections, and physiotherapy are of value to reduce symptoms, but a true treatment aiming at halting or even reversing the degenerative process and preserving the natural state of the disc is needed [3]. In an effort to “prevent” or “treat” discogenic low-back pain in a minimally invasive manner, and to maintain the normal kinematics of the spine, various motion-preservation technologies that attempt to prevent or to reverse the degeneration process of the disc have been addressed via the use of growth factors, chondrocyte transplantation, and gene therapy [28 –34]. Cell-based therapies for treating disc degeneration have gathered considerable attention over the past decade. This modality allows the injection of cells into the disc to repair lost cells and matrix, and to increase proteoglycan content. Mesenchymal stromal/stem cells (MSCs) are one of the available sources for cell-based repair of the disc currently under in-depth research [35 –37]. MSCs are a heterogeneous population of multipotent cells capable to differentiate along the chondrogenic, osteogenic, and adipogenic lineages but not the hematopoietic lineage. Various sources of MSCs have been identified and studied, including bone marrow (BM), synovial membrane, and adipose tissues [38 –40].
Of recent years, tremendous research efforts and funding have been devoted worldwide toward investigating the utility of MSCs to treat disc degeneration. An effective and safe MSC treatment should restore the biochemical and physical architecture of the intervertebral disc without complications. However, various complications (eg, tumor formation, undesirable bone formation, immune reaction, etc.) have been reported with the use of stem cells for other medical conditions, which has caused particular scepticism regarding their safety in the human body and in particular in a high-pressured region, such as the disc, where leakage of the implant may occur [41 –43]. Although the use of MSCs for the disc has gathered considerable attention throughout the past decade, no systematic review has been addressed to truly assess their safety and efficacy for disc regeneration to fully substantiate this modality as a potential treatment for disc degeneration. Therefore, the primary objective of this study was to systematically review, in a Cochrane fashion, comparative controlled studies of the existing peer-reviewed literature to assess the safety and efficacy of MSCs compared to no treatment/saline in animals and human subjects. Our second objective was to assess the quality of these published reports.
Materials and Methods
Literature search
A systematic review of the peer-reviewed literature was performed to identify comparative controlled experiments in animal models or humans. Online searches of PubMed, MEDLINE, EMBASE, and BIOSIS were performed on March 11, 2013. Search terms were generated, which included “mesenchymal stem cell transplantation,” “adipose stem cell,” “mesenchymal stem cell,” “synovial stem cell,” “intervertebral disc,” and “disc regeneration” with various Boolean operators. These terms were used without any restrictions concerning language or date of publication. Searches of the databases using these search terms were preformed independently by two individuals (Rita Lok-Hay Yim and Juliana Tsz-Yan Lee). The bibliographies of relevant articles were searched for further screening. All relevant studies were reviewed manually for eligibility.
Selection criteria
Studies were selected according to Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. Case reports, case series, prospective nonrandomized clinical trials, and all in vitro studies were excluded. Studies that used mammals were included irrespective of vertebral segment receiving implantation of cells. Both randomized and nonrandomized animal or human studies with control groups were eligible for inclusion. Valid control groups were defined as subjects with healthy nonintervened intervertebral discs or a degenerated disc receiving no intervention or sham procedure. Studies that compared MSCs against other types of differentiated cells or stem cells were also included. Included studies were required to provide a comprehensive description of disc degeneration induction and MSC injection protocol [44]. Studies without specification on dose and source of MSCs used for injection were excluded. In addition, studies focused on evaluating methodologies for follow-up analysis, and studies that had adopted only a single assessment were also excluded from this review.
Data extraction
Data extraction addressed outcomes of disc regeneration by multiple methods reported in any form, which included anatomical, radiographic, histological, biochemical, and/or molecular assessments. Since different animal models have different life cycle hence lifespan, intermediate and long-term outcomes were evaluated as defined by authors in each article. Events of complications stemming from MSC implantation in any form were recorded according to reports from each publication. Parameters including approaches for disc degeneration, types, dosages, and injection protocols of MSCs into each animal model were extracted. Assessment parameters pertinent for validity assessment and demographics of the animals studied were abstracted and tabulated (Table 1). Follow-up methodologies and final outcomes of their last follow-up were abstracted and summarized with the evaluation of sample randomization and grading of blindness according to the methodology of each study (Table 2). Only data from in vivo experiments were extracted from articles, whereas in vitro experiments were disregarded. Two individuals (Rita Lok-Hay Yim and Juliana Tsz-Yan Lee) independently extracted relevant data parameters and a consensus was reached in the event of initial disagreement.
AD, adipose; AF, annulus fibrosus; BCP, bilaminar coculture pellet; BM, bone marrow; cABC, chondroitinase ABC; CFDA, carboxyfluorescein diacetate; DAPI, 4′,6-diamidino-2-phenylindole; GFP, green fluorescent protein; MSC, mesenchymal stem cell; NP, nucleus pulposus; TGF, transforming growth factor.
ADSC, adipose-derived stem cells; FISH, fluorescent in situ hybridization; HSC, hematopoietic stem cell; ICC, immunocytochemistry; IDD, intervertebral disc degeneration; IHC, immunohistochemistry; MRI, magnetic resonance imaging; RT-PCR, reverse transcription polymerase chain reaction; RT-qPCR, quantitative reverse transcription polymerase chain reaction; RX, radiography.
Validity assessment
Internal validity was assessed by the following components adapted from Jadad et al. [45]. Briefly, a modified composite scoring system was generated based on nine parameters which points were awarded if the study fulfilled the criteria. Three parameters were directly related to the control of potential bias and included (i) description of animal drop-outs, (ii) randomization (defined as randomly allocating animals into different treatment or control groups), and (iii) blindness. The other six minor criteria were indirectly related to bias control, points were awarded equally if the study fulfilled such criteria. These criteria included were as follows: (i) if the study's objectives were clearly defined, (ii) if outcome measurements were clearly disclosed and explained, (iii) if criteria for inclusion and exclusion of animals were described, (iv) if sample size of the study was clearly calculated and justified, (v) if methodology of induction of disc degeneration and intradiscal injection was clearly disclosed, and (vi) if methods for measuring complications of treatment were clearly documented. A total of 14 points can be achieved utilizing the Jadad et al. [45] method. Studies were regarded excellent (score 11–14), good (score 8–10), fair (score 5–7), or poor (score 4 or less).
Statistical analyses
Due to the heterogeneity of the studies with relation to animal models used, time period of assessment, number and type of cells used, injection techniques, and postinjection assessment methods of the disc, it was found to be not sensible to pool studies to perform a meta-analysis addressing the effects of MSCs upon the disc. However, complication events based on animal rather than specific disc levels were accounted and a complication rate was tabulated from all MSC cases.
Results
Study characteristics
The literature search produced a total of 1,333 studies (Fig. 1). Seven hundred studies were further reviewed for eligibility after excluding 633 duplicated studies. Further, 639 studies and 34 in vitro and unrelated studies were excluded. Out of the 27 articles subjected to further review, 1 was excluded as the doses of MSCs injected were not specified, 1 was excluded since only one assessment method was adopted, and 1 was rejected as no quantitative data were generated for statistical analysis. This produced 24 articles published between 2003 and 2013, representing 862 discs that were injected with MSCs and 1,603 discs as controls. Approximately, MSCs were injected into the disc of 473 animals.
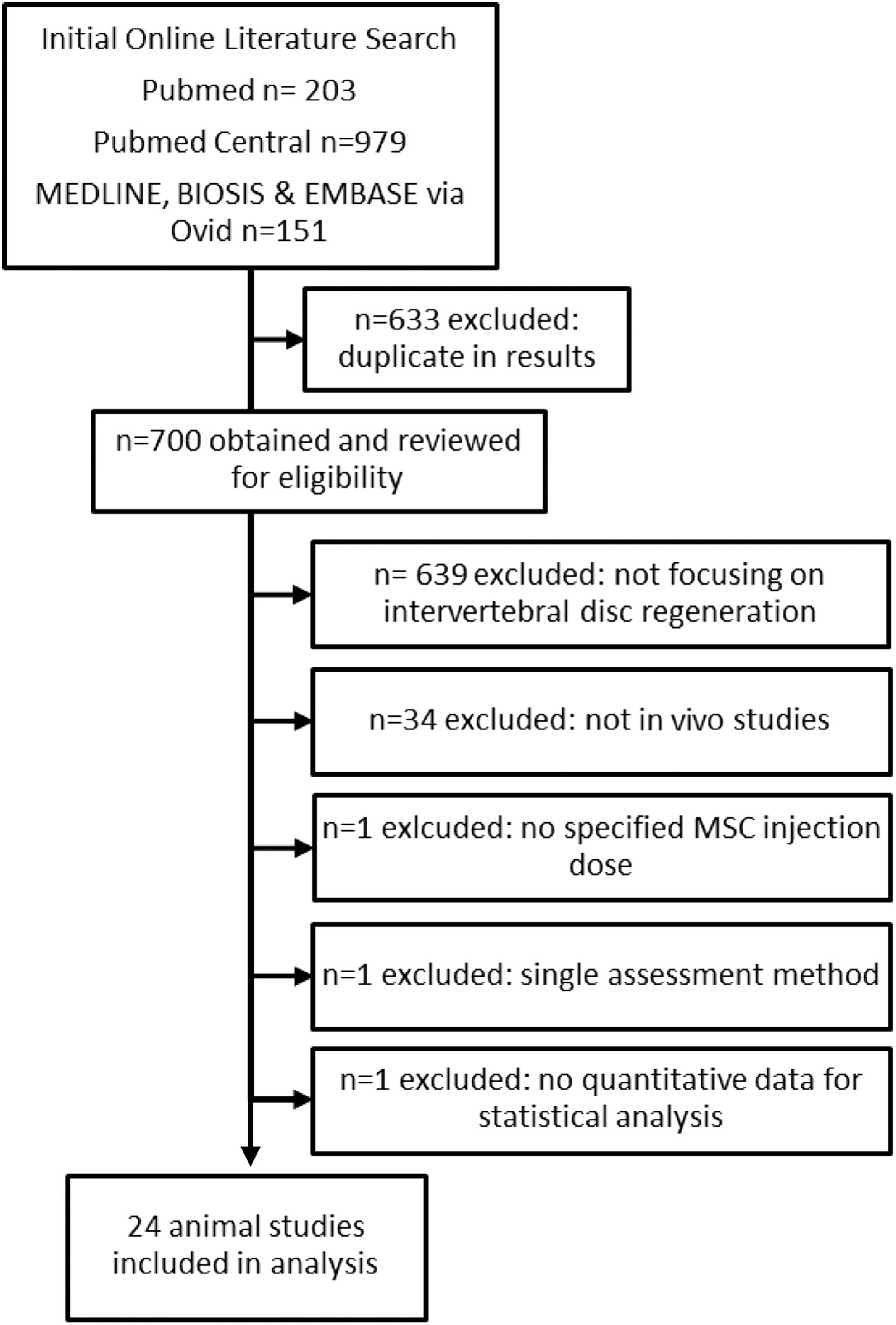
Flow diagram of literature search and included studies.
Of these 24 articles, 6 showed at least partial randomization of their studies. Relatively high-quality articles adopted strategies with minimal invasiveness and were reported in 13 studies; that is, only fine needle was used for induction of degeneration and MSC implantation instead of open surgery on the NP. Fine-needle microinjectors were used with needle sizes of 33G for mice and 30G for rats (or larger animals). At the time of the literature search, no randomized or quasi-randomized controlled clinical trials in humans were reported.
Small animals (ie, mouse, rat, and rabbit) and large animals (sheep, dog, and minipig) were used in different studies. Disc regeneration by injection of MSCs was assessed by measurement of disc height index (DHI) using radiography and by real-time PCR or similar biochemical approaches of postmortem spinal units. A restoration of DHI similar to healthy control groups along with increased expression of proteoglycan or ECM genes was considered as successful disc regeneration. Bone marrow was used as the source of MSCs in 21 studies, while 2 studies used adipose-tissue-derived MSCs (AD-MSCs), and synovial tissue-derived MSCs were used in only 1 study (Table 1). Fifteen studies tracked MSCs in vivo or in situ for regenerative ability by green fluorescent protein (GFP), 4′,6-diamidino-2-phenylindole (DAPI), or LacZ genes as reporter systems.
Histology and magnetic resonance imaging (MRI) were commonly used to monitor overall recovery of disc height and water content while anatomical analysis was used less frequently. Other techniques were supplemented for further molecular characterization, including immunostaining, quantitative reverse transcription polymerase chain reaction (RT-qPCR), and biochemical tests (Table 2). However, different combinations of assessment methods and nonstandardized parameters and genes studied made comparison at the molecular level across various animal species difficult. One of the nonstandardized parameters was the measurement of disc height by radiography. Although this was a common assessment method, not all publications disclosed disc height after treatment as normalized values to pretransplantation values, which required manual conversion of data in the analysis of potential bias of these publications during validity assessments.
Validity assessment
Quality assessments of all 24 articles were performed using a modified scoring system from Jadad et al. [45] (Table 3). All of the studies except one included at least a sham control or degenerative controls. Despite that these reports were are all controlled studies, only five studies (20.8%) declared some sort of randomization. Only one study, which was reported by Hee et al. [46], clearly disclosed sample size calculation, whereas all remaining studies did not explain or conduct sample size calculation or power analyses. However, justification of sample size was not a critical parameter that determined the validity of the publication, as all animal studies included control groups to minimize variability among individual animals. Histological assessments were made in all except two studies that used radiography with fluoroscopy or MRI for disc assessment [47,48]. Blindness could not be assessed in most studies as they were unclear whether histological outcomes and outcome assessments were conducted by a third party; as such, nonblinding was assumed. Overall, 4.2% (n=1) of the studies were regarded of excellent quality, 45.8% (n=11) as good, 29.2% (n=7) as fair, and 20.8% (n=5) as poor.
The higher the total score, the higher the study quality. Scores of 11–13, excellent; 8–10, good; 5–7, fair; 0–4, poor.
Outcome and quality of repair by bone marrow MSCs
Mouse
Disc regeneration using a low injection dose of MSCs was studied by Yang et al. [49] in mouse models. Without application of cell carrier, they demonstrated that regeneration was still observed when only 103 BM-MSCs were injected into each tail disc, evident by restoration of disc height and repopulation of cells in the NP region. By GFP immunostaining, the number of GFP-MSCs was found to decrease significantly from 4 to 24 weeks after injection. Dual staining of GFP with chondrocyte markers, like SOX9 and collagen type II, revealed that a portion of GFP+ cells acquired a chondrocyte-like morphology and phenotype as a result of successful in vivo differentiation. MSC differentiation was further evident by an increasing number of these GFP+ cells expressing both chondrocyte markers. Also, endogenous (GFP−) cells showed increased cell proliferation in response to injected BM-MSCs and contribute to disc regeneration.
Rat
In rats, human BM-MSC transplantation study was performed by Jeong et al. [50] without application of carrier or sealant, resulting in inhibition of disc degeneration starting from 2 weeks post-BM-MSC injection. BM-MSC-treated discs had a stabilized histological score compared with the degeneration controls (injected with saline) throughout the 8-week study period but the injected BM-MSC only survived for 2 weeks. Disc degeneration was induced by longitudinal hemisection by blade instead of standard disc nucleotomy as performed in other similar studies [48,51,52]. In a later study, the same authors focused on AD-MSC transplantation in rats [40]. In comparison with Allon et al. [51] who used 2.5×106 cells for transplantation, Crevensten et al. [48] transplanted BM-MSCs at a lower dose (5×105/disc) and found proliferation in vivo at 28 days postinjection with a marked decrease in injected cell number over the first 7 days. They therefore proposed that hyaluronan gel might not be an ideal carrier because of potential initial cytoxicity to BM-MSCs and failure to retain cells within the site of injection. To avoid the pitfall of cell leakage, Allon et al. [51] developed a pellet coculture system of BM-MSCs and NP cells in which cells were encapsulated within a spherical bilaminar scaffold. This entire 3D coculture system was subsequently grafted into denucleated tail discs by open surgery, and this system showed a better BM-MSC retention up to 80% and superior differentiation compared with controls.
Wei et al. [52] investigated human CD34+ hematopoietic stem cells (HSCs) and CD34− BM-MSCs in rat model of disc degeneration. They further investigated potential immune reactivity within NP during disc regeneration. The authors found superior cell survival of CD34− BM-MSCs until day 42 whereas CD34+ HSCs were no longer detected after 21 days postinjection. Despite the formation of clusters and streaks, these cells showed upregulation of collagen type II and SOX9 proteins, indicating stimulated chondrogenesis. In agreement with the avascular and immunoprivileged nature of the intervertebral disc (IVD), no macrophage infiltration was detected in both treatment groups but only CD34− BM-MSC-treated rats showed Fas-L upregulation in host NP cells. The authors therefore proposed that upregulated Fas-L phenotype protected the cells from an immune response.
Rabbit
Rabbit was by far the best studied small-animal model for disc regeneration using BM-MSCs. To reach the ultimate goal of disc regeneration by repopulating the disc with NP cells, Feng et al. [53] compared the healing effect of BM-MSCs with differentiated NP cells. Although they found no direct evidence for superiority of BM-MSCs over NP cells in terms of disc height recovery, water content, histological outcome, proteoglycan, and matrix gene expression, they suggested that BM-MSCs could serve as an alternative to NP cell injection. Three independent studies were published by Sakai et al. [54 –56], which all applied atelocollagen gel as carrier. The two studies in 2003 and 2006 by Sakai et al. [54,55] collectively demonstrated that autologous BM-MSCs survived up to 48 weeks and atelocollagen gel promoted in vivo cell proliferation, differentiation, and expression of proteoglycan genes and collagen II gene. However, in their 2003 study, the MSC-transplanted group showed no significant improvement on histological grading compared with the normal and degenerated control groups [16,57]. Restoration of disc height and water content detected by radiography and MRI was suggested to be the result of BM-MSC differentiation toward NP-like cells in their 2005 study [55]. This study also demonstrated that a cell injection dose of 2×104 cells per disc was capable to restore proteoglycan content and expression of related ECM genes to normal levels.
Sobajima et al. [58] found that grafted cells survived up to 24 weeks with injected cells homing into the transition zone between NP and inner AF region, although the cell suspension in saline was injected directly into the NP region with an ultrafine 30G needle. In line with Wei et al. [52], Sobajima et al. [58] found no evidence of immune cell infiltration. To further optimize the carrier system for BM-MSC injection, Yang et al. [59] described a carrier gel system supplemented with transforming growth factor (TGF)-β1 during BM-MSC expansion and injection into denucleated discs. They suggested that the deceleration of disc height reduction observed could be due to a reduced cell apoptosis of NP cells that produced more collagen II. However, Ho et al. [57] reported that the severity of disc degeneration was an influential factor determining the efficacy of cell-based treatment. After injection of BM-MSCs in rabbit discs with disc degeneration at 7 months after annular puncture, IVDs showed further reduction in disc height measured by radiography, but restored proteoglycan content and histological grades. On the other hand, in rabbits with early degeneration at 1 month after annular puncturing, injection of BM-MSCs partially succeeded in prevention of disc height reduction, yet the discs showed no significant improvements in proteoglycan content nor histological grades. Therefore the authors concluded that the therapeutic effect of injection of BM-MSCs was more optimal in later than in early stage of degeneration. In terms of methods in inducing disc degeneration in animal, most studies adopted NP-surgical-based techniques for induction of disc degeneration, yet Hee et al. [46] developed an external compressing device to induce disc degeneration with no surgical intervention of the NP region. In line with other studies, the authors showed that recipient rabbits, which were subsequently switched to mechanical disc distraction alongside with MSC injection, displayed superior regenerative effect of MSCs than those only receiving a mechanical disc compression leading to formation of degeneration.
Larger animals
Canine, porcine, and ovine models were studied by five different research groups but molecular characterization of collagen II upon BM-MSC injection was only conducted by Serigano et al. [60] using dog models, and Henriksson et al. [61] and Acosta et al. [62] using minipigs. Serigano et al. [60] further investigated the optimal BM-MSC injection dose for maintaining survival and localization of BM-MSCs within the central NP region. They found that the NP and inner AF structures were best maintained at a dose of 105 and 107 cells per disc but 106 cells per disc showed the least apoptosis with similar regenerative efficacy compared with a higher injection dose. On the other hand, Hiyama et al. [63] adopted another approach to study BM-MSC survival within the IVD by investigating Fas-L expression. They demonstrated that BM-MSCs survived for 8 weeks after injection and showed upregulation of Fas-L that contributed to the successful disc regeneration at 12 weeks after injection compared with controls, supporting the immunoprivilege of BM-MSCs in disc regeneration.
Henriksson et al. [61] showed in the minipig model that injected human BM-MSCs survived within the porcine disc with expression of chondrocyte markers SOX9 and collagen II accompanied by increased aggrecan expression at 6 months after injection. Similar to Sobajima et al. [58], they found localization of BM-MSCs in the transition zone between NP and inner AF and supported the hypothesis that application of a 3D-gel carrier system can promote MSC survival and differentiation. On the other hand, Bendtsen et al. [47] investigated the effect of BM-MSC injection on vertebral blood flow and demonstrated that successful IVD rehydration and disc height recovery was partially attributed to restoration of permeability of the endplate. They concluded that survival of BM-MSCs for more than 12 weeks in vivo was attributed by maintenance of blood flow and hence homeostasis of the IVD microenvironment.
In majority of studies, bone marrow aspirate was cultured to deplete nonadherent hematopoietic cells leading to variable differentiation stages of isolated BM-MSCs and potential cell contamination from mononuclear cells. Therefore a modified methodology for isolation of BM-MSCs was studied and introduced by Ghosh et al. [64], immunoselecting MSCs by STRO-3 expression using magnetic Dynabeads. Similar quality of repair was achieved at 6 weeks after MSC injection when adopting a lower dose (0.5×106 cells/disc) compared with the higher dose (4×106 cells/disc), but the lower dose showed a superior cell survival. This supports the finding of Serigano et al. [60] that the avascular IVD has a limited nutrient supply that may compromise MSC survival when excess cells are injected [58,60,64].
The regeneration efficiency of MSCs was compared with NP cells by Feng et al. [53] in rabbits, but the ischemic IVD microenvironment also supported the replacement of MSCs by articular chondrocytes in minipigs as described by Acosta et al. [62]. Twelve months after injection, excessive tissue scarring was reported in the MSC-treated group without remarkable proteoglycan regeneration compared with the groups transplanted with juvenile articular chondrocytes. Moreover, in situ tracking of injected male MSCs in female recipient minipigs by fluorescent in situ hybridization probing Y-chromosome only detected survival of articular chondrocytes but not of MSCs, indicating that MSCs were more prone to cell death in the ischemic IVD with limited nutrient supply, especially when cells are injected in excess [53,62].
Outcome and quality of repair by adipose MSCs and synovial MSCs
AD-MSC-based studies included only one with the rat [40] and with the dog [65] model. Jeong et al. [50] utilized a simple rat model to inject human AD-MSCs at a dose of 5×104 cells per disc, which was much lower than their study using BM-MSCs (106 cells/disc) as described earlier. Two weeks after AD-MSC injection, inhibition of further disc degeneration in the stem-cell-treated group was evidenced by restoration of MRI signal, nucleic acid staining, and collagen type II staining. In the dog model studied by Ganey et al. [65], hyaluronic acid was used as carrier for better AD-MSC delivery. After 6 and 12 months of recovery, disc explants from sacrificed dogs showed significant regeneration in terms of nucleus material, hydration, and disc height as detected by gross morphology, MRI, and radiography. RT-qPCR detected upregulation of collagen II and aggrecan genes but also of collagen I gene, indicating fibrosis in the disc. DAPI-labeled cells surrounded by abundant ECM were identified by fluorescent microscopy at both time points, indicating survival of the AD-MSCs.
Miyamoto et al. [66] described the only synovial MSC study in rabbits in which labeled allogenic rabbit AD-MSCs were grafted immediately after disc nucleotomy at a dose of 107 cells per disc. Despite MRI and radiography indicating a favorable outcome, histological staining of treated discs revealed fibrosis within the NP region, suggesting that further conditioning was required.
Safety of MSCs
Only 2 of 24 studies reported complications, assuming that there were no complications in the remaining 22 studies. Sobajima et al. [58] reported that, in one rabbit, ossification was found at 24 weeks postinjection but no details were provided. Vadalà et al. [42] reported that, 9 weeks after injection of MSCs, they detected no signs of restored NP area signal intensity using MRI but they detected the presence of GFP+ cell within the large osteophytes formed anterolaterally as a result of potential cell leakage. To address the issue, the potential reasons for complications were discussed, including cells were injected without a carrier to retain the cells at the site of injection, or no sealant was used to close the injection hole through the annulus to avoid cell leakage [42]. Overall, MSC-related complications were noted in 2.7% of all animal models. Since complications were noted in only rabbits, they represented 5% of complications within group.
Discussion
Based on reported animal studies, our systematic review has demonstrated that the use of MSCs for the treatment of disc degeneration is largely safe and effective. Complication rates based on all animals injected with MSCs was 2.7%, all occurring in rabbit models. With the exception of 2 reports out of 24 controlled trials, no further complications were noted. According to Sobajima et al. [58] and Vadalà et al. [42], findings in a rabbit model noted osteopyte formation anterolaterally to the disc space, which was attributed to leakage of the MSCs. Vadalà et al. [42] emphasized the significance of using a cell carrier and annulus sealing technique after injection to reduce the risk of uncontrolled differentiation of MSCs into osteoblasts. When comparing MSC treatment with other types of treatments, for example, articular chondrocytes [62] and mechanical distraction devices [46], MSC treatment seems to demonstrate a more persistent and consistent quality of regenerative effect. In a clinical setting, injection of MSCs has the advantage of minimizing invasiveness of secondary surgery in comparison with installation of mechanical device that also requires tertiary surgery to remove device after treatment.
Among all the sources of MSCs being studied in vivo, MSCs isolated from bone marrow were found to be the best studied source compared with MSCs isolated from adipose and synovial tissue. Although there is no clear recommendation concerning efficacy of different sources of MSCs in vivo, BM-MSCs currently offer the most information on therapeutic potential with the stem cell molecular mechanism and most importantly MSC survival in vivo being better studied compared with the other two MSC sources. Therefore from the clinical standpoint, adipose and synovial MSCs tend to be a viable option for autologous BM-MSCs whenever bone marrow is not suitable to be used (eg, patients with bone marrow abnormalities).
Outcome of most studies seems to be valid based on histological grading and MRI but outcome is more difficult to interpret by the other assessment methods, such as by RT-qPCR, due to lack of well-defined NP and chondrocyte markers. Emerging evidence supports that MSCs replicate and differentiate toward NP cells when injected into a degenerated site and they stimulate endogenous NP cells to proliferate and hence repopulate the intervertebral disc. Multiple studies also support the tendency that injected MSCs have a latency period before they can replicate and repair the affected disc and application of a gel carrier improves the repair efficiency. Further, the quality of repair by BM-MSCs seems to be dependent on severity of degeneration, but it is also suspected that MSCs will not differentiate into disc cells if MSCs cannot even survive for at least a short period of time upon injection. As reported by Ho et al. [57], proteoglycan content and restoration of disc height were more improved when the degree of disc degeneration was higher. Despite there also reported a gentle decrease in surviving MSCs in smaller animal models in long term, large-animal studies supported the hypothesis that MSC proliferation in vivo is not critically dependent on local blood circulation. This is based on the observation that MSCs still survived considerably within the central NP region of minipigs despite NP had a lower oxygen supply compared with the annular region due to the larger disc size compared with smaller animals, like rabbits, mice, and rats. All these combined evidences support the application of BM-MSCs for regeneration of intervertebral disc and that long-term survival of injected cells in the hypoxic disc environment is feasible. In addition to MSC long-term survival in vivo, immediate and trophic effects are of great importance in supporting MSC differentiation into disc cells, contributing to immediate disc repairing. Therefore, future studies can also focus on methods that support MSC differentiation as adjuvants. It should also be noted that trophic effects from MSCs injected into the intervertebral disc could potentially contribute to activate endogenous disc or stem cells to enhance the regenerative efficiency, as is noted, for example, when MSCs are transplanted into an overactive bladder [67]. This further highlights the long-term therapeutic effect of MSCs mediated by the paracrine system. From a clinical perspective, when efficacy of regeneration is shown to be dependent on the degree of degeneration, detailed clinical staging of patients with disc degeneration is required to screen for appropriate patients to receive MSC transplantation.
In general, there is a lack of collective evidence to support that injected BM-MSCs only differentiate into NP cells as molecular analyses also detected upregulation of common biomarkers for large vacuolated NP cells and small-sized articular chondrocytes [68]. It has to be highlighted that during development and aging, large vacuolated notochordal cells are gradually replaced by chondrocyte-like cells and these cells are distinct from each other for their proteoglycan and matrix production. There are publications further suggesting that disappearance of notochordal cells along with aging could account partially for disc degeneration [69,70]. This limitation shall be addressed by devising definite markers that differentiate NP cells from chondrocytes and other cell subpopulations that reside in the intervertebral disc. The selection of animal models shall also resemble human spine, especially disc size, proteoglycan content, cell population, and distribution across the intervertebral disc.
Once the animal model is selected, the approach in generating disc degeneration should be less invasive and spontaneous to mimic human disc degeneration. For example, a chondrodystrophic dog can be bred until 1-year old to develop spontaneous disc degeneration whose gross pathology and histology is found similar to human [71]. It is also recommended to perform these studies on lumbar discs (instead of tail disc, etc.) as these structures receive major mechanical loading from the body weight of the animal, hence, being similar to the human spine. When designing these experiments, randomization of disc-level injections should be performed to ensure that successful regeneration is not a result of less mechanical loading compared with sham/degenerate controls. The follow-up methods should include not only gross anatomy, DHI, but also include molecular studies that detect notochordal cells when a well-defined marker panel is devised to differentiate notochordal cells from chondrocytes.
For the overall quality of all the 24 publications, a modified Jadad scoring scale is devised and applied in this study. This scoring system does not only consider randomization and blinding similar to clinical trials but also evaluates the quality based on other criteria that are not applicable in human. One of the major factors that require consideration is disclosure of the methodology used that to induce degeneration, since an invasive open surgery may predispose the disc to cell leakage and hinder disc regeneration after MSC implantation. Similarly, a clear explanation as to the manner MSCs implanted is desired as implantation of a large-volume solid implant could hinder the recovery of the injured disc and it also would require a larger cavity for implantation that may also press against peripheral tissues. From the information collected, description of the disc degeneration and MSC implantation approaches can be improved based on the collective outcomes of individual articles. Based on the modified Jadad scoring system, our systematic review noted that 50% of the studies were of good-to-excellent quality, whereas 29.2% and 20.8% are of fair and poor quality, respectively.
There were only two reported human clinical trials found during the literature search, dated in 2010 and 2011, respectively. Since both studies were not blinded study and did not include control groups, we classified both studies as Phase IV studies that had poor level of evidence. In a study by Yoshikawa et al. [36], two female patients diagnosed with intervertebral disc degeneration were treated with autologous BM-MSCs. Patient selection criteria were based on MRI, radiography, myleography, and development of spontaneous back pain confirming intervertebral disc degeneration and instability. Similar to the animal trials using hydrogel carrier, about 20 collagen porous sponges were soaked with the MSC suspension and were grafted into central region of the intervertebral disc guided by fluoroscopy. The surgical hole was sealed with an acellular collagen sponge. Although no significant improvement was seen using T1-weighted MRI 2 years postinjection, T2-weighted MRI showed increased signal intensities in both patients, indicating restoration of water content in treated intervertebral discs. In Orozco et al. [35] case series study in 2011, a total of 10 patients were recruited in their pilot Phase 1 clinical study using autologous BM-MSCs. Guided by fluoroscopy, cells were injected into the NP region without a carrier or annulus sealant. The post-transplant observation period lasted for 12 months adopting standard clinical analytical procedures that showed that pain was relieved. However, T2-weighted MRI showed no significant improvement in water content and disc height.
Animal studies have provided preclinical knowledge of MSC-based regeneration but not all methods used in animal studies can be directly translated into human randomized controlled trials or final clinical application. For example, molecular assessments by reverse transcription polymerase chain reaction used in many animal studies require tissue sampling and surgical sampling from treated patients that is not ethical and practical due to the invasiveness of the procedure. Analysis of gene expression as an outcome measure can therefore not be applied in a clinical setting. MRI remains the best option for monitoring the quality of disc repair. Finally, long-term significance of MSC-based treatment remains relatively unknown since the lifespan of animals in trials is largely not prolonged to assess outcomes.
Conclusions
This is the first study to address, in a systematic fashion, the safety and efficacy of MSCs for the treatment of disc degeneration. Our study noted that MSCs in animals present a low incidence rate of complications (∼2.7%) and are effective in halting the progression of disc degeneration or increasing disc height. MSCs offer a treatment option to disc degeneration, whereby published clinical trials and pilot studies demonstrate the ability of MSCs to inhibit disc degeneration. However, randomized clinical trials in humans have not been reported and are needed. Future clinical trials for MSC use should aim to have proper subject selection and identify the appropriate phenotype of disc degeneration to ensure optimal effectiveness, define a series of standards to calculate the minimal effective dosage of stem cell use, utilization of a carrier or annular sealant to prevent cell leakage, and adopt a delivery method to prevent further disc breakdown while optimizing cell efficacy. Proper randomization should be taken into consideration to ensure that high level of evidence can be produced.
Footnotes
Acknowledgments
This work was supported by grants from the Hong Kong Area of Excellence (AoE/M-04/04) and the Theme-Based Research (T12-708/12N) schemes.
Author Disclosure Statement
No competing financial interests exist.