
Abstract
Autologous bone marrow stem cell (ABMSC) transplantation has been utilized in clinical practice to treat patients with liver failure, but the therapeutic effect remains to be defined. A meta-analysis is essential to assess clinical advantages of ABMSC transplantation in patients with liver failure. A systematic search of published works [eg, PubMed, Medline, Embase, Chin J Clinicians (Electronic edition), and Science Citation Index] was conducted to compare clinical outcomes of ABMSC transplantation in patients with liver failure. Meta-analytic results were tested by fixed-effects model or random-effects model, dependent on the characteristics of variables. A total of 534 patients from seven studies were included in final meta-analysis. Subsequent to ABMSC transplantation, there was no significant improvement in general symptom and signs such as loss of appetite, fatigue, and ascites. Activities of serum ALT were not significantly decreased with weighted mean difference (WMD) of −19.36 and 95% confidence interval (CI) −57.53 to 18.80 (P=0.32). Postoperative level of albumin (ALB) was expectedly enhanced by stem cell transplantation (WMD 2.97, 95% CI 0.52 to 5.43, P<0.05, I 2=84%). Coagulation function was improved as demonstrated by a short prothrombin time (PT) (WMD −1.18, 95% CI −2.32 to −0.03, P<0.05, I 2=6%), but was not reflected by prothrombin activity (PTA) (P=0.39). Total bilirubin (TBIL) was drastically diminished after ABMSC therapy (WMD −14.85, 95% CI −20.39 to −9.32, P<0.01, I 2=73%). Model for end-stage liver disease (MELD) scores were dramatically reduced (WMD −2.27, 95% CI −3.53 to −1.02, P<0.01, I 2=0%). The advantage of ABMSC transplantation could be maintained more than 24 weeks as displayed by time-courses of ALB, TBIL, and MELD score. ABMSC transplantation does provide beneficial effects for patients with liver failure. Therapeutic effects can last for 6 months. However, long-term effects need to be determined.
Introduction
L
The liver failure is commonly caused by viral infection (HBV and HCV), alcoholism, drug overdose, cholestasis, poison (wild mushrooms and herbal medications), autoimmunity (PBC and PSC), inherited factor (hemochromatosis), or unknown origin. Causative factors induce liver injury via distinctive modes of cell death, including necrosis, necroptosis, autophagy, and apoptosis [3]. The pre-existing genetic condition modifies susceptibility to various types of the causative factors and perpetuates the destruction of liver tissue [4]. These diverse modes of cell death consist in a dynamic spectrum during liver injury. The mode of liver cell death is doubtlessly determined by the duration and magnitude of etiological factors. When the extent of hepatocyte death is less than the capacity of liver regeneration, liver function can be compensated. Otherwise, liver failure occurs. The hepatocyte death contains two major types or apoptosis and necrosis [5]. Apoptosis as a temperate response is less severe than necrosis, but both modes of cell death often coexist in liver disease, dependent on the severity of the insult. ATP as energy molecule is necessary for the execution of apoptosis, whereas ATP is depleted in necrotic tissue. Apoptosis is associated with little secondary impairment as compared with necrosis. The necrotic process recruits inflammatory cells (eg, neutrophils) into liver parenchyma. Liver injury is further aggravated by inflammatory response, which leads to dramatically different outcome from apoptotic cell death in regard to progression of liver disease [6]. When the hepatic parenchyma is seriously damaged and poor function is unable to meet metabolic requirements of the body, a devastating syndrome of ALF develops. The crucial outcome is reflected by a series of clinical complications, such as coagulopathy, encephalopathy, hemodynamic changes, and electrolyte disturbance. There is a complicated relationship between liver injury and the syndrome of ALF. Current knowledge on ALF pathophysiology is limited due to the lack of an adequate animal model of the disease. Recent data indicate that necrosis is associated with poor outcome of ALF. The detection of necrosis can therefore become useful to identify ALF patients for liver transplantation. The liver failure can be diagnosed through a detailed history, sign and symptom, blood test, imaging test, and liver biopsy. Early recognition of the ALF and an aggressive treatment can improve clinical outcome. Despite significant advance in medical care, however, the mortality remains extremely high.
Treatment of liver failure depends on information that clinicians promptly collect. For instance, an early detection of ALF caused by an overdose of acetaminophen may decrease death rate. Likewise, if the liver failure is caused by viral infection, medical treatment and supportive care can alleviate symptoms of virus-induced liver injury, inhibit virus replication, and restore liver function. Intervention of liver failure includes (1) Medications to treat poisoning. Adequate medications can reverse effects of the toxins and relieve ALF induced by acetaminophen overdose or mushroom poisoning; (2) Treatment for complications. A positive treatment of complications can interrupt the deterioration of liver function and gives the liver healing time. Improving symptoms and signs that patient is experiencing can impede disease progression, such as (a) relieving brain edema, (b) treating the infection, and (c) preventing severe bleeding; (3) Stem cell transplantation. For liver failure resulting from chronic liver disease, the guideline of initial treatment is to save still functioning part of the liver and to stimulate the regenerative capacity of the liver. A challenge is how to get enough hepatocytes for the recovery of liver function [7]. In recent years, a series of cytotherapeutics have been carried out, such as autologous bone marrow mesenchymal stem cell transplantation, in vitro proliferation of bone marrow stem cells and transplantation, umbilical cord stem cell transplantation, and hepatocyte transplantation [8 –11]. These therapies provide the best evidence for cell engraftment that promotes generation of functional liver parenchyma. In addition, autologous bone marrow stem cell (ABMSC) mobilized by an injection of granulocyte colony-stimulating factor (GCSF) can also be included in the field of stem cell therapy [12]; (4) Orthotopic liver transplantation. In many cases, ALF is hard to be reversed. A liver transplant becomes necessary in clinical treatment. In fact, liver transplantation is the most effective treatment for liver failure [13]. Sometimes, a liver transplant is the only cure for ALF. Fortunately, liver transplantation as a common procedure is often successful. Unfortunately, liver transplantation is limited by rejection, adverse effects of immunosuppressive drugs, and especially a shortage of donor organ.
Animal experiments and clinical trials have shown beneficial effects of stem cell therapy [14,15]. The intravenous injection of hematopoietic stem cells into mouse model of tyrosinemia type I could correct the metabolic defect and rescue the animal with disease. Another study also demonstrated that purified hematopoietic stem cells could differentiate into hepatocytes and stimulate the hepatic regeneration in vivo. Based on a set of animal data, some clinical studies are performed in patients with liver disease. Many prospective trials have evaluated the efficacy and safety of ABMSC transplantation. The ABMSC transplantation includes different cell types such as CD34, CD133, or unsorted cell mixture. Transfusion of cells can be via intrahepatic, intrasplenic, or peripheral veins. The mechanism for transplantation of ABMSC to improve the situation of liver failure remains unknown. Potential therapeutic mechanisms involve regeneration, antiapoptosis, inhibition of inflammation, and regulation of immunity. Therapeutic effects of ABMSC transplantation can be estimated by the improvement of symptoms and signs, serum enzyme activities, biochemical markers (eg, albumin, bilirubin, glucose, and cholesterol), coagulation function, comprehensive MELD and Child–Pugh scores, mortality, survival rate, and so on.
A significant advancement has been obtained as patients with liver failure were treated through the ABMSC transplantation [14 –17]. However, the clinical outcomes are inconsistent. Moreover, an optimal method of the ABMSC transplantation for liver failure is still unknown. From laboratory and clinical perspective, the treatment of liver failure by the ABMSC transplantation is beneficial. Unfortunately, there is heterogeneity in published studies. Some studies are based on small sample sizes with low statistical power, which cannot predict the result of a single large study. We therefore conducted a meta-analysis of ABMSC transplantation according to the standard of the Cochrane Collaboration. A meta-analysis based on systematic review of the literature can assess not only the effect and advantage of ABMSC transplantation in patients undergoing liver failure, but also the strength of the evidence supporting such a favorable result. Results demonstrate the ABMSC transplantation can improve liver function in short term, but long-term effects need to be observed.
Methods
Systematical search of published work
We systematically screened PubMed, Medline, Embase, Chin J Clinicians (Electronic edition), and Science Citation Index until April 2014. References were identified using the following keywords: “bone marrow stem cell” and “human liver disease.” The search of published work was not restricted by types of clinical studies. The relevant literature was further scrutinized by the completeness of data.
Study selection
Trials eligible for inclusion were based on quality of evidence, included Grade I randomized controlled trials, Grade II-1 controlled trials without randomization, and GradeII-2 cohort or case–control analytic studies [18]. We excluded studies with umbilicus cord stem cells and stem cells out of peripheral blood subsequent to a GCSF injection. Also, the exclusion covered studies that provided insufficient data relating to the prespecified outcome variables. The included studies only contained patients with the transplantation of ABMSCs. Data extraction was accomplished by two investigators independently. Disagreement was resolved by third opinion.
Data collection and outcome measures
We extracted general data on characteristics of participants (source of reference, country, study design, age, and sex composition of patients), intervention, and outcome measures in different studies. A primary comparison was performed among basic data out of ABMSC transplantation and control groups. We analyzed common symptoms and signs, levels of ALT, ALB, TBIL, PT/PTA/INR, MELD score, Child–Pugh score, morbidity, and mortality. Morbidity was calculated by number of patients with at least one complication after ABMSC transplantation and mortality by in-hospital or at home death due to any cause. We subsequently excluded studies in which not enough data were reported. Meta-analysis was further performed including symptoms and signs, quantitative data of ALT, ALB, TBIL, PT/PTA, and MELD score.
Study quality assessment
Bias in primary studies can lead to misleading summary estimates of accuracy. Quality assessment guides the interpretation of results in terms of potential for bias and sources of heterogeneity. The methodological quality of included studies was evaluated by random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, and selective reporting. Priori criteria of high quality study include (1) Randomized trials; (2) Prospective cohort study; (3) Consecutive patient enrollment; (4) Adequately reported methodology of measurement.
Statistical analysis
Review Manager (RevMan version 5.2, 2012; The Cochrane Collaboration, Oxford, United Kingdom) was used to pool data and meta-analysis. For categorical variable, treatment effect was expressed as odds ratio (OR) with corresponding 95% confidence intervals (CI). Results were compared through a random-effects model. For continuous variable, treatment effect was expressed as weighted mean difference (WMD) with corresponding 95% CI. Chi-square (Chi2 or χ 2) and I 2 statistics estimate the appropriateness of pooling individual study. Heterogeneity was evaluated by χ 2-test with significance set at P value 0.10. Heterogeneity was measured by I 2 more than 50% as statistical significance. Forest plots were constructed with P values of less than 0.05 as significant difference.
Results
Quality assessment of the included studies
A total of 1,366 references were identified through the electronic search. After original full texts had been reviewed, seven studies involving a total of 534 patients were included in present meta-analysis, which were from different countries including Egypt, Brazil, Japan, and China (Fig. 1) [8,19 –24]. Resultant data were compared between stem cell transplantation (n=291) with control (n=243) groups. The risk of bias in the included studies was moderate (Fig. 2). The distribution of sample size and effect size could be outlined with a funnel plot. Owing to the small number of included studies, the funnel plot asymmetry was not investigated [25].
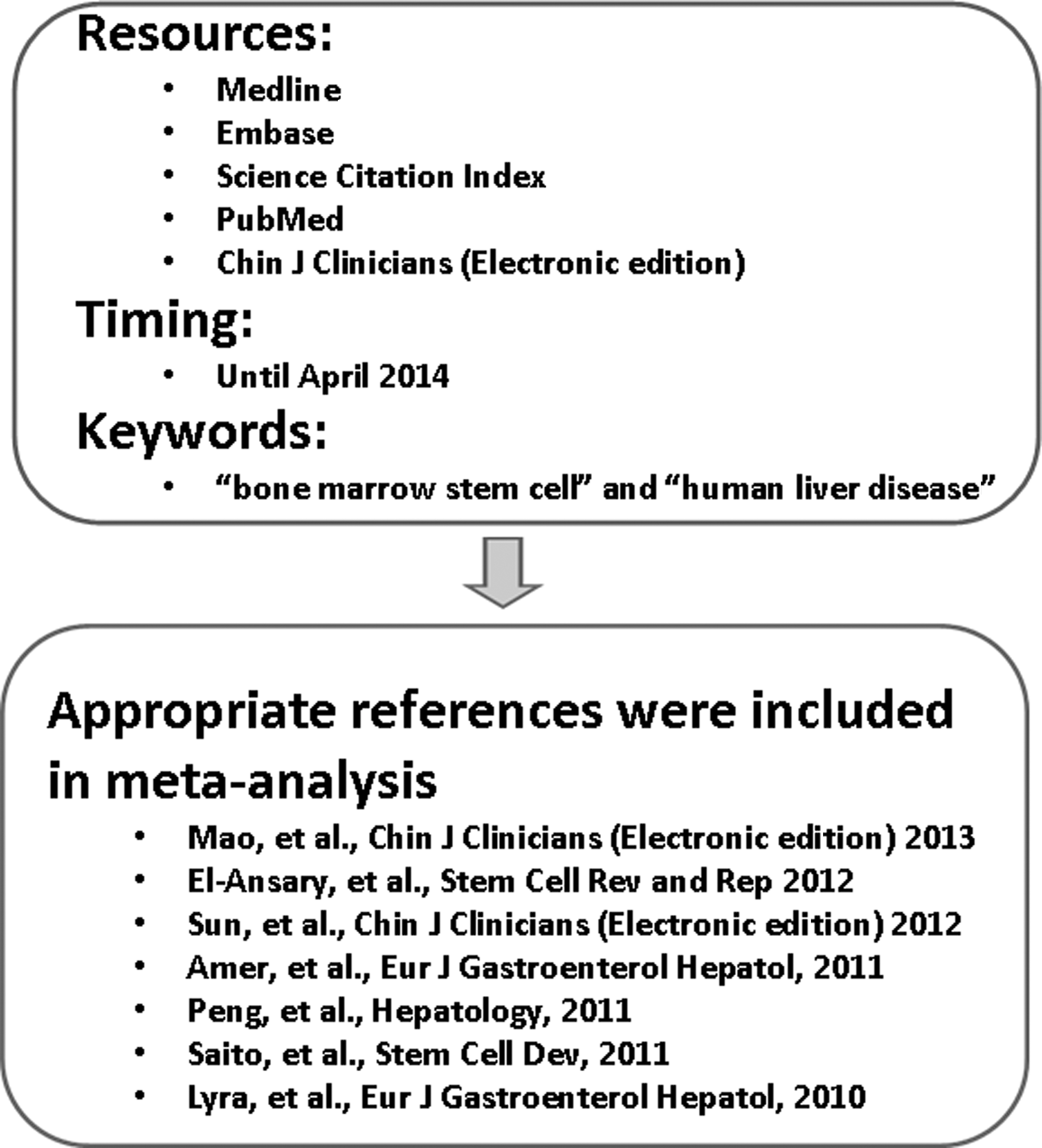
Flow chart of references that were identified and included respectively.
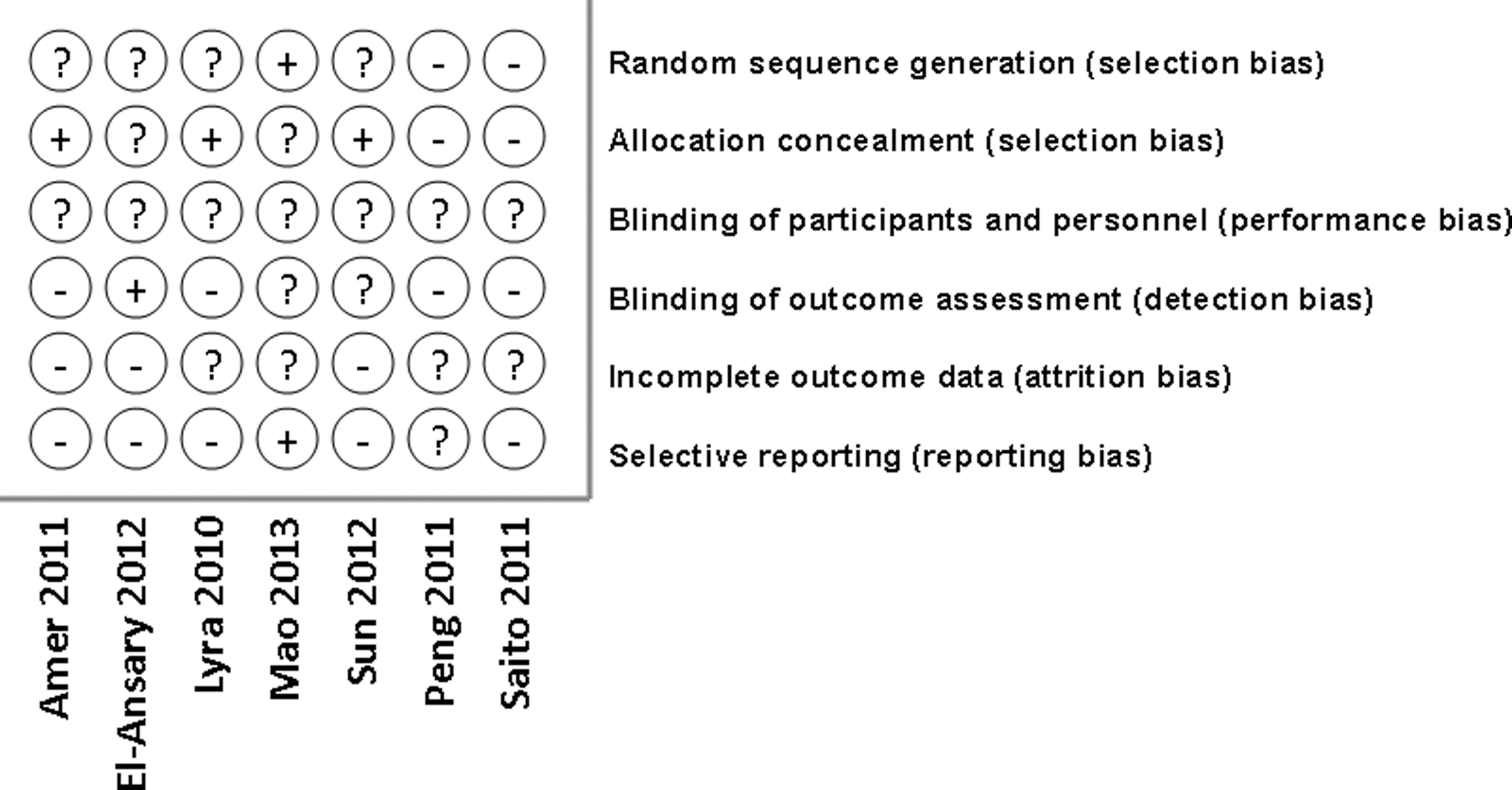
Summary of potential bias in the identified trials.
Description of the included studies
A systematic review that covered stem cell treatment for human liver disease in recent years was summarized (Table 1). Following stem cell treatment, the liver function was improved at certain degrees as demonstrated in the different types of liver disease [8,19 –24,26]. Here, types of stem cells include ABMSC, in vitro proliferation of ABMSC, umbilical cord stem cells, and GCSF-mobilized stem cells. Other parameters of stem cells were also compared, containing characteristics of stem cells, pattern of intervention, and clinical improvement subsequent to transplantation. Only studies using bone marrow ABMSC transplantation were chosen for further meta-analysis. General characteristics of the included studies were reflected by source of data, study design, number of patients, ratio of male/female, and age (Table 2). Of note, Peng study also randomized cirrhotic patients into stem cell transplantation group (73.58%) and control group (73.33%) (P=0.973).
AIH, autoimmune hepatitis; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALB, albumin; TBIL, total bilirubin; PT, prothrombin time; PTA, prothrombin activity; BM, bone marrow; MSC, mesenchymal stem cell; CP, Child–Pugh score; MELD, model for end- stage liver disease; PBC, primary biliary cirrhosis; PB, peripheral blood; G-CSF, granulocyte colony-stimulating factor; INR, international normalized ratio; MNCs, mononuclear cells; ICG-R15, indocyanine green R15.
Grade I: randomized controlled trials; Grade II-1: controlled trials without randomization.
N/A, not available.
Improvement of clinical symptoms and signs
Short-term therapeutic effects or outcomes subsequent to stem cell transplantation could be reflected by an improvement of clinical symptom and sign such as pain, nausea, loss of appetite, fatigue, dizziness, jaundice, edema, abdominal distension, ascites, pruritis, tremor, complications (bleeding, erythema, and encephalopathy), and so on. According to an availability of data, only loss of appetite, fatigue, and ascites were selected to represent patient's changes in clinical symptom and sign. Studies by El-Ansary, Lyra, and Saito did not provide information on appetite and fatigue. Amer study gave a mean fatigue impact scale. Therefore, they were excluded in meta-analysis. A random-effect model was used to investigate the therapeutic effect of ABMSC transplantation when I 2≥50%. There was no significant difference in loss of appetite between the stem cell transplantation and control groups (I 2=50%, OR, 1.66; 95% CI, 0.90–3.07; P=0.11) (Fig. 3a). Information on the number of patients in fatigue symptom was available for three studies relating to 429 patients (Fig. 3b). No improvement in fatigue symptom was found (I 2=93%, OR, 2.62; 95% CI, 0.48–14.30; P=0.27). Although individualized studies by El-Ansary and Sun showed ascites was significantly improved after stem cell infusion, there was no statistical difference in meta-analysis of ascites between ABMSC transplantation and control groups (I 2=82%, OR, 2.09; 95% CI, 0.64–6.79; P=0.22) (Fig. 3c).
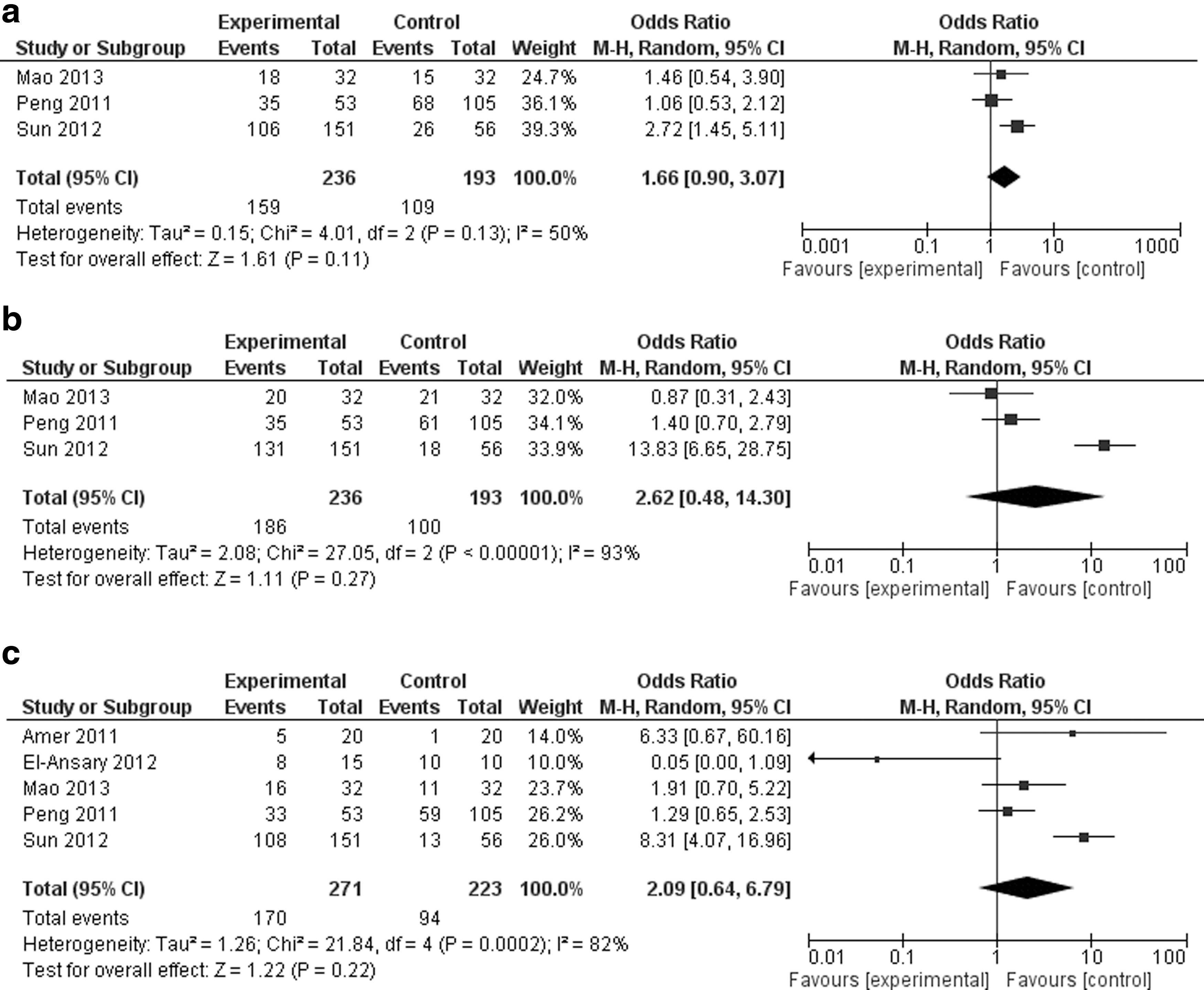
Forest plots illustrate outcomes of clinical symptom and sign in patients undergoing stem cell transplantation.
Improvement of liver function by levels of ALT, ALB, TBIL, and PT/PTA/INR
Serum ALT activity is a basic marker to estimate liver injury (Table 3). Studies by Mao et al., Sun et al., and Peng et al. provided primary data on ALT activity. El-Ansary study reported enzyme activities of ALT, ALP, GGT, and AST as median (range). Studies by Lyra, Saito, and Amer did not give any information on ALT activities. Meta-analysis of ALT activities indicated that the postoperative ALT level was not significantly altered between the transplantation and control groups (WMD, −19.36; 95% CI, −57.53 to 18.80; P=0.32; I 2=99%) (Fig. 4a). Time-course of ALT activity was provided by Peng et al. from postoperative week 1 to 48. The ALT levels showed significant decrease in the ABMSC transplantation group compared with the control group during 36 weeks. Albumin is an essential part of liver function panel (Table 4). Amer study presented serum albumin as figure. Lyra study showed albumin change in percentage and El-Ansary study provided albumin data as median (range). So they were not eligible for meta-analysis. Postoperative level of albumin was higher in the stem cell group than the control group (WMD, 2.97; 95% CI, 0.52–5.43; P<0.05; I 2=84%) (Fig. 4b). Time-course of ALB by Peng et al. showed that ALB was quickly enhanced subsequent to ABMSC transplantation during 3–24 weeks. However, no significant difference was found after 48 weeks between ABMSC and control groups. For TBIL measurement, El-Ansary study reported TBIL level as median (range), Lyra study as figure, and Amer/Saito studies as a narrative description or “there was no difference between patients and control groups regarding serum bilirubin.” Other three trials provided available data on postoperative levels of bilirubin. Meta-analysis of the bilirubin showed a significant difference in the ABMSC transplantation group compared with control group (WMD, −14.85; 95% CI, −20.39 to −9.32; P<0.01; I 2=73%) (Fig. 4c). Time-course of TBIL by Peng et al. revealed that serum TBIL were significantly decreased from postoperative week 4 to 12, but no difference after 36 weeks between transplantation and control groups. The improvement of TBIL in stem cell group was markedly superior to those in control group during 4–12 week after ABMSC transplantation. Moreover, biochemical levels ALB, TBIL, and ALT in Mao study were analyzed under Child–Pugh A&B and Child–Pugh C grades, respectively. Stem cell transplantation significantly improved biochemical levels in patients with Child–Pugh C grade. Coagulation function could be determined by PT, PTA, or INR values. PT and PTA data were unavailable in Amer study, but a description indicated no INR difference between stem cell therapy and control groups. Lyra study reported the coagulation function as INR not PT/PTA. Meta-analysis of PT showed an improvement in stem cell group (WMD, −1.18; 95% CI, −2.32 to −0.03; P<0.05; I 2=6%), but PTA levels were unchanged between two groups (P=0.39) (Fig. 4d, e). After stem cell transplantation, the improvement in PT scores of ABMSC group was significantly superior to those of control group during 4–12 week as demonstrated by Peng study.
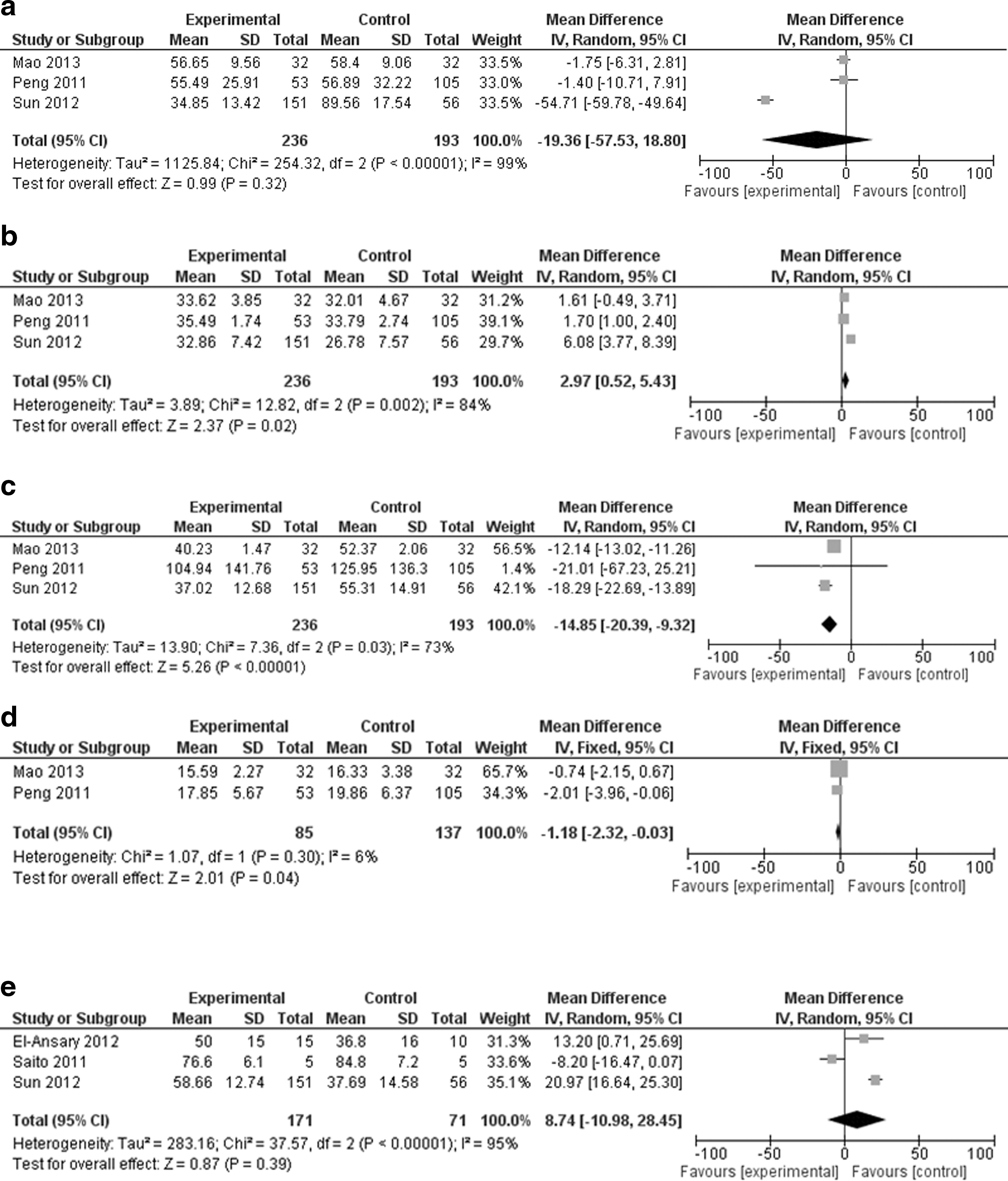
Forest plots show an improvement of liver function as reflected by
ABMSC, autologous bone marrow stem cell; ALT, alanine aminotransferase; N.S., not significant; N/A, not available.
ALB, albumin; N.S., not significant; N/A, not available.
Improvement of liver function can be indirectly reflected by changes of kidney function, glucose, total cholesterol, hemogram, and tumorigenic AFP expression
Postoperative kidney function was monitored by levels of urine volume, creatinine, and BUN in Sun study and the concentration of creatinine in El-Ansary study as median (range). However, not enough information from other studies was reported. Thus, it was unable to perform meta-analysis of kidney function. Although levels of glucose and total cholesterol could also be affected by liver disease relevant data were not available to run meta-analysis. Hemoglobin, leukocyte, and platelet counts were presented in El-Ansary study as median (range). No hemogram information from other studies was provided. AFP, a tumorigenic marker of hepatocellular carcinoma (HCC), was measured only in El-Ansary study following stem cell transplantation. In Peng study, one case in stem cell group suffered from HCC at the 20th week after transplantation and nine cases in control group developed HCC throughout the 48-week follow-up (P=0.107). Furthermore, there was no difference in incidence of HCC during 192 weeks of follow-up. The included studies did not provide enough information to do meta-analysis of carcinogenesis.
Therapeutic effects of ABMSC transplantation were evaluated by comprehensive MELD score, Child–Pugh score, liver volume, mortality, and morbidity
Single marker can estimate one aspect of liver function. Therapeutic effects of ABMSC transplantation need to be evaluated by comprehensive markers such as MELD score, Child–Pugh score, liver volume, mortality, and morbidity. A meta-analysis of Amer and Peng studies disclosed a significant improvement of MELD score following ABMSC transplantation (WMD, −2.27; 95% CI, −3.53 to −1.02; P<0.01; I 2=0%) (Fig. 5). In Peng study, the improvement of MELD score in ABMSC group was prominently superior to that of control group during 3–36 weeks after transplantation. Child–Pugh scores were provided in El-Ansary study (in percentage). A time-course of Child–Pugh scores in Amer study showed a significant improvement during 6 month after stem cell transplantation. These results revealed that there were significantly low MELD and Child–Pugh scores subsequent to the stem cell transplantation. In Saito study, the functional liver volume in cm3 was obtained using single photon emission CT with a radiolabeled Tc-GSA and calculated by the outline extraction method. The functional index was improved during 2 weeks in four of the five patients who received stem cell therapy. In Sun study, one patient died in control group and one patient died in stem cell group respectively. In Peng study, no death number was available, but it reported no dramatic difference in mortality during 192 weeks of follow-up. Additionally, survival rate was plotted as figure in Peng study. No significant difference in survival rate was found between two groups. The meta-analysis of complications or morbidity in the included studies also demonstrated no statistical difference between stem cell transplantation and control groups.

Meta-analysis of MELD score in patients with the ABMSC transplantation. ABMSC, autologous bone marrow stem cell; MELD, model for end-stage liver disease.
Discussion
Major finding
The ABMSC transplantation has been utilized in clinical practice for the treatment of liver failure. A meta-analysis including all available data can provide a weighted average of effect size. Meta-analysis results of included studies demonstrate that the ABMSC transplantation does not alleviate the common symptom and sign as reflected by loss of appetite, fatigue, and ascites. Serum levels of ALT activities were not significantly improved by ABMSC therapy. However, the ABMSC transplantation is truly beneficial to patients with liver failure in the improvement of coagulation function (PT), albumin (ALB), bilirubin metabolism (TBIL), and severity of liver disease (MELD). These favorable effects can last at least 6 months, but long-term effects remain to be determined.
Mechanisms of therapeutic ABMSC transplantation
The improvement of liver function is found following ABMSC transplantation in short term. This finding supports the hypothesis that stem cells may be directly involved in the regeneration and repair of liver tissue. The exact mechanisms of stem cell therapy are unknown. Liver-protective effect of ABMSC transplantation may be via several aspects: (1) to stimulate liver regeneration. The regenerative response of liver injury mostly depends upon mature parenchymal cells. When native regenerative abilities of parenchymal cells have been exhausted, a foreign stimulation or supplementation becomes a necessity. Only rigorously purified hematopoietic stem cells can promote hepatocyte proliferation [14,16,26]; (2) to differentiate directly into parenchymal hepatocytes to compensate for the cell loss; (3) to secrete protective factors that prevent progressive apoptosis of functional cells and stimulate replication of host cells; (4) to regulate immunologic response of host liver; (5) preventing the liver fibrogenesis via a variety of cytokines, such as HGF, interleukin-6, and −10; (6) angiogenesis; and (7) to dissolve fibrosis directly through the production of matrix metalloproteinase [27 –35]. Moreover, the ABMSC transplantation promotes cell fusion with parenchymal cells for liver regeneration [14,16,34,36]. The cell fusion causes concern for safety due to theoretically possible contribution to tumor formation. Notably, stem cells have profibrogenic potential and may contribute to scar-forming myofibroblasts in liver [37,38]. Transplanted MSCs can migrate into liver parenchyma to stimulate cell differentiation, particularly under conditions of chronic injury. Previous studies revealed that hepatocyte-like cells were limited to a low number; by contrast, myofibroblast-like cells were observed in a significant number. Thus, profibrogenic potential of MSCs has to be noticed. Because of multiple functions of ABMSC, it is no surprise that the ABMSC transplantation can improve the prognosis of liver disease. Meta-analysis of available studies demonstrated that there was significant improvement of relevant biomarkers subsequent to ABMSC transplantation, which again confirms the mechanism and advantage of stem cell therapy in the recovery phase of liver injury.
Clinical significance
The stem cell therapy provides new strategy for the treatment of both primary and secondary liver injury. The ABMSC transplantation has much beneficial role in the improvement of liver failure [8,19,21]. Therefore, its clinical application becomes popular in recent years. The following observations are noticed: (1) Stem cell transplantation could be through different routes such as intrasplenic, intrahepatic, and peripheral vein. In the included studies, only one intrasplenic research was performed by Amer team. No statistical difference was observed between intrahepatic and intrasplenic groups. Both hepatic and splenic groups had a consistent outcome as regards jaundice, edema, serum albumin, serum bilirubin, liver enzymes, hemoglobin, total leucocytic count, or platelet; (2) Intrahepatic route was again subdivided into hepatic artery and portal vein pathways. Sun study demonstrated that transplantation of stem cells via either hepatic artery (87 patients) or portal vein (64 patients) resulted in a similar improvement in levels of ALT, ALB, TBIL, PTA, urine volume, BUN, and creatinine. An injection through portal vein was better than via hepatic artery because of relatively low percentage in adverse response and complications (eg, fever, fatigue, nausea, dizziness, bleeding, hepatalgia, hematoma, low leucocytic count, and thrombosis) via portal vein transplantation. Indeed, in contrast to control group, the liver failure can be ameliorated with appropriate stem cell therapy. Remarkably, the benefit of ABMSC transplantation is based on the small number of included studies and mainly time-course data from Peng study. The additional evidence is thus needed to support the anticipated conclusion. Advantages of ABMSC transplantation can be reflected by the improvement of clinical symptoms and signs, biochemical levels of liver function, MELD score, Child–Pugh score, morbidity, and mortality [8,19,20]. Other medical therapies such as antivirus, the treatment of complications and supportive therapeutics, can be combined with ABMSC transplantation against liver failure. An increased possibility of tumorigenesis in stem cell-treated patients further highlights the need for a regular evaluation of cancerous risk [39,40]. Potential mechanisms that lead to tumorigenesis subsequent to stem cell treatment implicate transdifferentiation of bone marrow stem cells and cell fusion between premalignant cell and bone marrow stem cell. Comprehensively, the mechanisms of tumorigenesis are complicated and beyond the scope of this review.
Study limitations
This study has a few limitations. The number of patients included in this meta-analysis is small and the published work search may not have covered all relevant references. In the present meta-analysis, it was impossible to adjust or stratify for potential confounders. Age, an important confounding factor for liver failure, is associated with severity of clinical complications and functional activity of stem cells [41 –43]. Although the included studies enrolled different ages of patients, we were unable to determine the effect of age on the strength of the association. Moreover, presence and extent of liver cirrhosis have an adverse impact on short-term prognosis of patients with liver failure. A meta-analysis has inherent weaknesses because of combining heterogeneous data sets. Current meta-analysis includes studies that they were of variable quality and provided insufficient information on potential sources of bias. Obvious heterogeneity had been observed among studies, because it was hard to match patient characteristics in all studies. A random-effects model was applied to examine variation between studies, but this might not rule out the effect of heterogeneity between studies. Furthermore, almost no information on therapeutic medications or supportive treatment was provided in the included studies. The potential impact of liver-protective therapy rather than stem cell transplantation could not be evaluated in this meta-analysis.
Perspective
At present, some small sample studies have shown beneficial roles of ABMSC transplantation in improvement of liver failure, whereas conflicting results have been reported in other studies as well [44 –46]. After having pooled data of available studies, we are able to re-explore the association between ABMSC transplantation and improvement of liver failure. The estimated ORs and WMDs for these variables may be less robust than those of established individual study. However, these biomarkers are very common and are well known for their roles in liver function. Future challenges include (1) long-term, large sample size, and randomized controlled study. Several critical issues deserve immediate attention, such as the optimal type of transfused stem cells, the most effective number of stem cells, the best route of administration, and the optimal therapeutic timing. It needs a long time to get answers to these issues. Clinical safety and long-term advantages of stem cell therapy should be also reinforced by a large-sized randomized controlled trial; (2) Liver-protective mechanisms of stem cell transplantation. It is important to track the fate of the transfused stem cells in vivo. The transfused stem cells can stimulate liver regeneration and improve liver function. However, stem cells are profibrogenic as well. The relationship between transfused stem cells and the hepatic inflammatory/fibrotic microenvironments is still to be determined [47,48]; (3) to test different types of stem cells, for example, umbilicus stem cells and adipose-derived stem cells; and (4) reinfusion to improve long-term benefits [20]. The reinfusion of adipose-derived adult stem cells has been utilized to treat complex perianal fistulas [49,50]. As a novel idea, the reinfusion of stem cells at regular intervals may be suitable for liver disease. If these challenges can be figured out, the clinical application of stem cell-based therapy will be warranted for the treatment of patients with liver disease.
Summary
Meta-analysis shows significant advantages of the ABMSC transplantation as demonstrated by the improvement of ALB, PT, TBIL, and MELD score. Further evidence from animal experiments and controlled clinical trials is still needed to estimate the beneficial and adverse effects. Future prospective study should be designed to assess the optimal technique of stem cell therapy, to investigate long-term therapeutic effects, and to clarify the underlying mechanisms. In conclusion, the liver function is significantly improved by ABMSC transplantation in patients with liver failure for short term. This finding strengthens the hypothesis that stem cells play essential roles in the recovery phase of liver disease. The long-term effect of stem cell therapy is still to be determined.
Footnotes
Acknowledgment
We appreciate Li Zhang's help during data extraction and preparation of this article.
Author Disclosure Statement
There are no commercial relationships or conflicts of interest in connection with this article.