
Abstract
MRL/lpr mice spontaneously develop high titers of anti-dsDNA antibodies and symptoms such as glomerular nephritis and organ weight gain. They also develop spontaneous skin inflammation similar to the cutaneous lesions common in human lupus erythematosus. This study aimed to compare the effects of long-term serial administration of human adipose tissue-derived mesenchymal stem cells (ASCs), CTLA4Ig-overexpressing ASCs, and cyclophosphamide treatment in MRL/lpr mice. MRL/lpr mice were divided into saline (C), cyclophosphamide (Y), ASC early (E), ASC late (L), and CTLA4Ig-overexpressing ASC (CT) treatment groups. Background-matched control MRL/MPJ mice treated with saline (N) were also compared. The treatment period was 5–23 weeks, except for the L group (15–23 weeks). Blood and tissue samples were collected when the mice were 24 weeks old. Organ weight, anti-dsDNA antibodies, urine protein, skin and kidney histologic abnormalities, and trabecular bone volume were evaluated. The Y group showed the greatest decrease in anti-dsDNA antibodies, organ weight, degree of kidney inflammation and glomerular infiltration of C3, and incidence rate of severe proteinuria; the E, L, and CT treatment groups showed better results than the C group. ASC transplantation reduced anti-dsDNA antibody levels significantly. Mice treated with ASCs or CTLA4Ig-ASCs starting from the early disease stage did not show dermatitis upon gross examination; they demonstrated significant improvement in hyperkeratosis, acanthosis, and inflammatory cell infiltration scores in histopathology. Micro-CT analysis revealed that cyclophosphamide treatment significantly decreased bone volume and increased bone spacing in the trabecular bone. Thus, we found that ASC and CTLA4-ASC treatments prevent lupus dermatitis development in MRL/lpr mice without adverse effects.
Introduction
S
Our previous study using the F1 hybrids of New Zealand Black and New Zealand White ([NZB×NZW] F1) female mice, which develop SLE, revealed that long-term serial human adipose tissue-derived mesenchymal stem cell (ASC) transplantation at an early stage of disease ameliorated the histological and serological abnormalities, immunological functions, and increased survival significantly [9]. In contrast, single or short-term allogeneic bone marrow-derived mesenchymal stem cell (MSC) transplantation at an advanced disease stage had no effect on these variables [10,11].
MRL/MpJ-Faslpr
/J (MRL/lpr) mice are other important models of human SLE. These mice spontaneously develop high titers of anti-dsDNA antibodies and symptoms, including organ malfunction, proteinuria, organ weight gain (including splenomegaly and lymphadenopathy), immune complex glomerulonephritis, dermatitis, and increased mortality, which resembles human SLE [12,13]. According to the Jackson Laboratory, the average life span of female MRL/lpr mice is 17 weeks and the levels of circulating immune complexes start to rise markedly at about 3 months of age (
Skin is the second most commonly affected organ in human SLE [14]. Skin and mucous membranes are symptomatically involved in over 80% of SLE patients [15]. MRL/lpr mice are important disease models, because they have the unique characteristic of spontaneous skin inflammation that occurs at a high frequency. Furthermore, the skin lesion in MRL/lpr mice is the best-characterized LE-like skin model and is considered relevant to cutaneous LE.
Conventional immunosuppressive therapies induce global immunosuppression in the body. In contrast, MSCs are selective immunomodulators because their suppressive effects occur only in the presence of an inflammatory environment [16]. Recent studies on successful MSC treatment in autoimmune diseases have been reported. Furthermore, in our previous studies on autoimmune thyroiditis and rheumatoid arthritis, CTLA4Ig-ASCs showed stronger suppression in the T-cell proliferation against autoantigens and were more effective in reducing serum levels of autoantibodies than nontransduced ASCs were [17 –19].
The purpose of this study was to evaluate the effect of long-term serial ASC (early and late treatments) and CTLA4Ig-overexpressing ASC transplantations in the MRL/lpr SLE mouse model. Parameters investigated included anti-dsDNA antibodies, proteinuria, organ weight, glomerulonephritis, and dermatitis.
Materials and Methods
Human ASC preparation
Human ASCs (hASCs) were prepared from surplus, frozen banked stem cells (K-STEMCELL, Seoul, Korea) as described previously [17]. Anonymized ASCs were used in this study under an institutional review board (IRB)-approved exemption (Samsung Medical Center IRB).
The preparation and validation of CTLA4Ig-ASCs
We constructed a therapeutic gene comprising the extracellular domain of mouse CTLA-4 (GenBank accession number NM_009843, nt 258–629) and the CH2–CH3 domains of the mouse immunoglobulin gamma 1 constant (IGHGC) region (GenBank accession number AB097849.1, nt 772–1452). The human oncostatin M signal sequence (GenBank accession number NM_020530.3, nt 53–127) was cloned along with the therapeutic gene to enable the secretion of this protein into body fluid. Therapeutic gene transduction into hASCs was conducted with ViraPower™ Lentiviral Expression Systems (Invitrogen, Carlsbad, CA) and CTLA4Ig-ASCs were selected by blasticidin as previously described [17]. The preparation and assessment of CTLA4Ig-hASCs also were performed as previously described [7,17].
Experimental animals
The breeding pairs of MRL/MpJ-Faslpr /J (MRL/lpr) and background-matched control MRL/MPJ mice were purchased from the Jackson Laboratory (Bar Harbor, ME). This study was reviewed and approved by the Institutional Animal Care and Use Committee of the Samsung Biomedical Research Institute (SBRI). SBRI is accredited by the Association for the Assessment and Accreditation of Laboratory Animal Care International and abides by the guidelines of the Institute of Laboratory Animal Resources.
Experimental groups and treatment protocol
For the in vivo study, the experimental groups consisted of a control group (C group, MRL/lpr, n=15), a cyclophosphamide-treated group (Y group, MRL/lpr, n=15), ASC-treated groups (E and L groups, MRL/lpr, n=15 per group), the CTLA4Ig-ASC-treated group (CT group, MRL/lpr, n=15), and the normal group (N group, MRL/MPJ, n=15). All mice used in this experiment were females.
Each mouse in the C and N groups was infused with 150 μL of saline every 2 weeks from 5 weeks of age until 23 weeks. Each mouse in the E and CT groups was intravenously (via the lateral tail vein) administered 106 ASCs and CTLA4Ig-ASCs/150 μL of saline every 2 weeks from the age of 5 weeks until 23 weeks (a total of 10 times), respectively. Each mouse in the L group was intravenously administered 106 ASCs/150 μL of saline every 2 weeks from the age of 15 weeks until 23 weeks (a total of five times). The Y group was injected intraperitoneally with 20 mg/kg of cyclophosphamide per week from 5 weeks of age until 23 weeks.
Determination of proteinuria
Fresh urine was collected by performing an abdominal massage. Urine protein was measured using the Coomassie Brilliant Blue method as previously described [9]. Urine creatinine was measured using a DRI-CHEM 3000 Colorimetric analyzer (Fujifilm, Tokyo, Japan) by diluting the urine in deionized water at a ratio of 1:100.
Determination of blood urea nitrogen, serum creatinine, and anti-dsDNA antibodies
Blood urea nitrogen (BUN) and serum creatinine were determined with a DRI-CHEM 3000 Colorimetric analyzer. Anti-dsDNA antibodies were measured in sera collected at 4, 12, 18, and 24 weeks of age, as previously described [9].
ELISA of multiple cytokine levels in sera and skin extract samples
Serum samples from all mice were assayed using a MILLIPLEX® MAP mouse cytokine/chemokine kit for GM-CSF, TNF-α, IFN-γ, IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-10, IL-12p70, IL-15, and IL-17 (Millipore, Bedford, MA). Skin samples were weighed and then transferred into 12.5 μL dPBS, which contained antiprotease Complete™ cocktail (Boehringer, Mannheim, Germany), per milligram of wet weight tissue. The samples were homogenized twice using a freeze-crushing cell homogenizer, Automill TK-AM5 (W280×D 390×H 290 mm; Tokken, Inc., Chiba, Japan), at 1,400 rpm for 90 s and centrifuged at 16,000 g for 15 min at 4°C. The supernatant was collected and stored at −70°C. Skin extract samples from mice (n=6/group) were assayed using a MILLIPLEX® MAP mouse cytokine/chemokine kit for TNF-α, IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-10, IL-12p70, IL-15, IL-17, KC, MCP-1, MIP-2, and RANTES (Millipore).
Determination of the proportion of T regulatory cells and CD138 cells by flow cytometry
Spleen cells were analyzed for T regulatory cell markers using antibodies against CD4, CD25, and Foxp3 (FITC rat anti-mouse CD4, APC rat anti-mouse CD25, and PE rat anti-mouse Foxp3; BD Biosciences, San Jose, CA). The proportion of CD138-positive cells was also determined (PE rat anti-mouse CD138; BD Biosciences).
Histological analysis
Hematoxylin and eosin (H&E), periodic acid-Schiff, and Masson's trichrome staining of the kidney were conducted as previously described [9]. The degree of inflammatory cell infiltration was scored from 1 to 4: 1 (infiltration area <10%), 2 (infiltration area 10%–19%), 3 (infiltration area 20%–30%), and 4 (infiltration area >30%). H&E staining of skin was also conducted and the degree of hyperkeratosis, acanthosis, and inflammatory cell infiltration was graded as 0 (none), 1+ (mild), 2+ (moderate), 3+ (moderate to severe), or 4+ (severe).
Immunofluorescence
Fresh kidney and skin tissue were embedded in optimum cutting temperature compound and frozen in 2-methylbutane slush. Slides were incubated with FITC-conjugated goat anti-mouse IgG (Millipore) or FITC-conjugated goat anti-mouse C3 (Cappel, West Chester, PA), as previously described [9]. The slides were then mounted with mounting medium containing DAPI (Vector laboratories, Southfield, MI) and examined with a laser scanning confocal microscope (LSM 700; Carl Zeiss, Jena, Germany).
Confocal microscopy examination of CM-DiI-labeled human MSCs
Three mice from the E, L, and CT groups were administered ASCs or CTLA4Ig-ASCs that were labeled with a conjugated red fluorophore, Cell Tracker CM-DiI, to permit identification in histopathological sections. The presence of CM-DiI-labeled cells was determined in various tissues, such as the spleen, lymph node, kidney, liver, lung, heart, brain, and skin (by counterstaining with mounting medium containing DAPI), with a laser scanning confocal microscope (LSM 700; Carl Zeiss).
Statistical analyses
All results are expressed as the mean±standard error of the mean. The results from experiments using the anti-dsDNA antibodies, as well as cytokine analysis, and micro-CT of the distal femoral metaphysis, were compared using the Kruskal–Wallis test followed by the Mann–Whitney U test. Other data were analyzed and different groups were compared using one-way analysis of variance, followed by post hoc Tukey's multiple comparison tests. Differences with a confidence level of 95% or higher were considered statistically significant (P<0.05). *Significant (P<0.05) differences from the control (C group) are marked by an asterisk. All statistical analyses were conducted using SPSS version 21.0 (SPSS, Inc., Chicago, IL).
Results
Organ weight
The mean weights of the spleen weight, kidney weight, liver, and individual organ/body weight ratio were lower in all treatment groups than the C group, and there was a significant difference between the Y and N groups compared with the C group (data not shown).
Anti-dsDNA antibodies
The levels of anti-dsDNA antibodies in sera were significantly lower in the N group compared with the C group at all observed ages. Anti-dsDNA antibodies in the Y group were significantly lower than those in the C group in sera collected from mice at 12, 18, and 24 weeks of age. In sera from mice at 18 weeks of age, the levels of anti-dsDNA antibodies in the E group were significantly lower than in the C group (Mann–Whitney U test, at each time point, Fig. 1a). The levels of anti-dsDNA antibodies in the CT group were similar to those in the E group, but there were no significant differences compared with the C group.

Anti-double-stranded DNA antibody and flow cytometry data in MRL/MpJ-Faslpr
/J (MRL/lpr) mice and background-matched control MRL/MPJ mice after treatments.
P<0.05), followed by the Mann–Whitney U test (*).
Urine protein and serum chemistry
The urine protein/creatinine ratios (UP/C) and the percentage of mice with UP/C <1 for the C, Y, E, L, CT, and N groups at 20 weeks of age are presented in Table 1. The incidence of severe proteinuria (>300 mg/dL) of those groups at 22 weeks of age is also presented in Table 1. The concentration of BUN, serum creatinine, and albumin was not significantly different among the groups.
N, normal group (MRL/MPJ); C, control group (MRL/lpr), saline; Y, cyclophosphamide; E, ASC early; L, ASC late; CT, CTLA4Ig-ASC treatment group; ASC, adipose tissue-derived mesenchymal stem cell; UP/C, urine protein/creatinine ratios.
The proportions of T regulatory and CD138 cells, as determined by flow cytometry
Spleen cells were analyzed to estimate the proportion of Treg cells (n=5 per group). The proportion of CD4+CD25+FoxP3+ cells in the N group was significantly higher than that in the C group; those of other treatment groups also showed an increase, although these differences failed to reach statistical significance (Fig. 1b). The proportions of CD138 cells were significantly lower in the Y and N groups than in the C group (n=5–7 per group, Fig. 1c).
Dermatitis and immunofluorescence of skin
Skin lesions in MRL/lpr mice were characterized by scabs and hair loss in the dorsum of the neck. Upon gross examination of the skin, 5 of 13 mice (38.5%) in the C group showed severe dermatitis and 2 of 14 mice (14.3%) in the L group showed mild dermatitis on the neck. No mice in the Y, E, CT, and N groups developed dermatitis (Fig. 2a). Representative histological staining images of skin lesions are presented (Fig. 2b). Skin lesions in the C group were more severe and were significantly different compared with those from other groups. The Y and CT groups showed significant improvement in hyperkeratosis, acanthosis, and inflammatory cell infiltrate scores compared with the C group (Fig. 2d). The E and L groups had statistically different scores for hyperkeratosis and inflammatory cell infiltration compared with the C group (Fig. 2d). The fluorescence intensity of IgG deposition in the dermal–epidermal junction was significantly lower in the CT and N groups than in the C group (Fig. 2c, d).
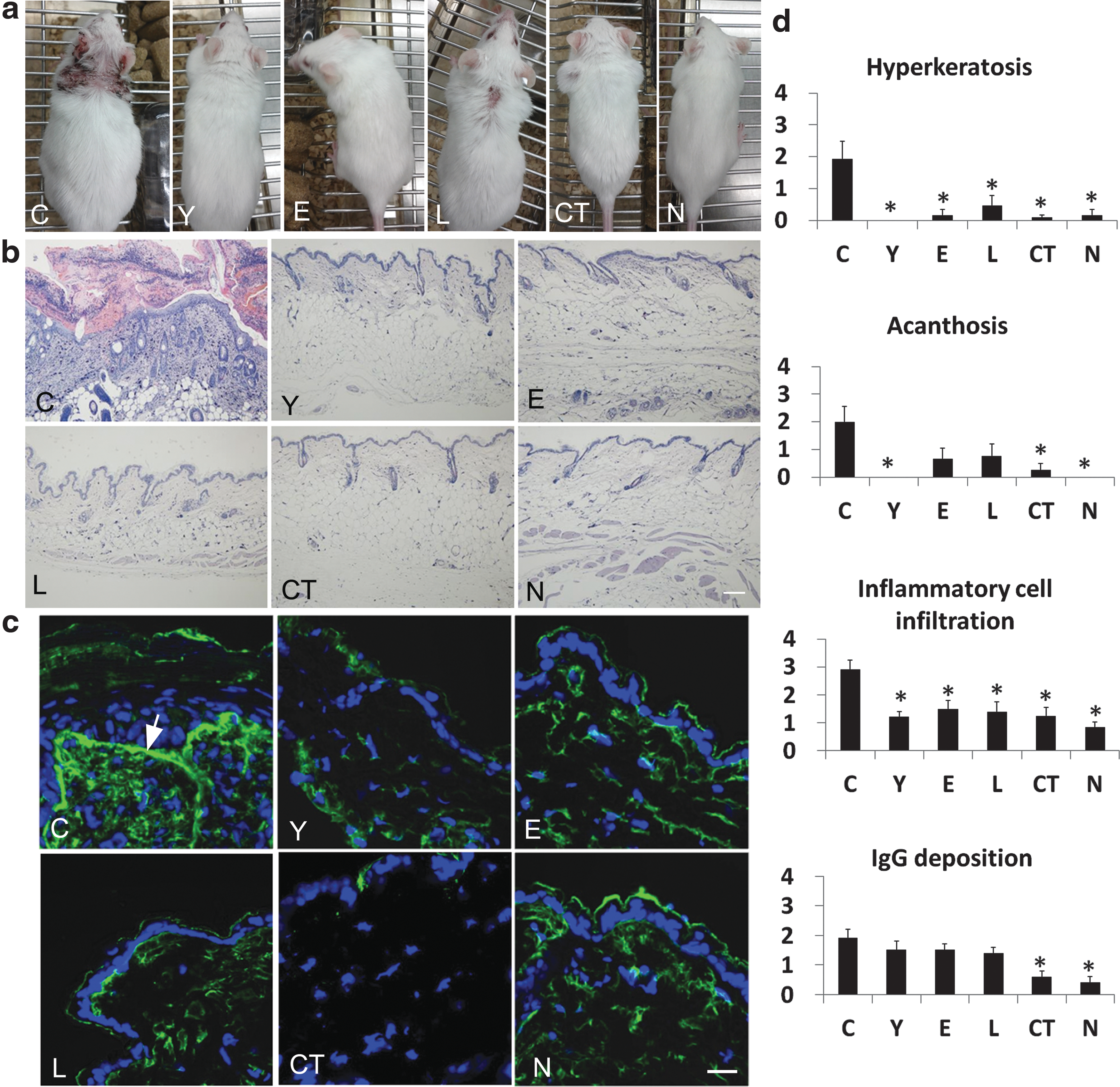
Morphological changes in skin samples from treated mice.
Kidney inflammation and immunofluorescence
Inflammatory cell infiltration in the kidney of the C, Y, E, L, CT, and N groups was evaluated (Fig. 3a). The score and percentage of inflammatory cell infiltration in the Y and N groups were significantly lower compared with those in the C group (Fig. 3b). The fluorescence intensity of IgG and C3 deposition in all treatment groups was significantly lower than that in the C group (Fig. 3c, d).
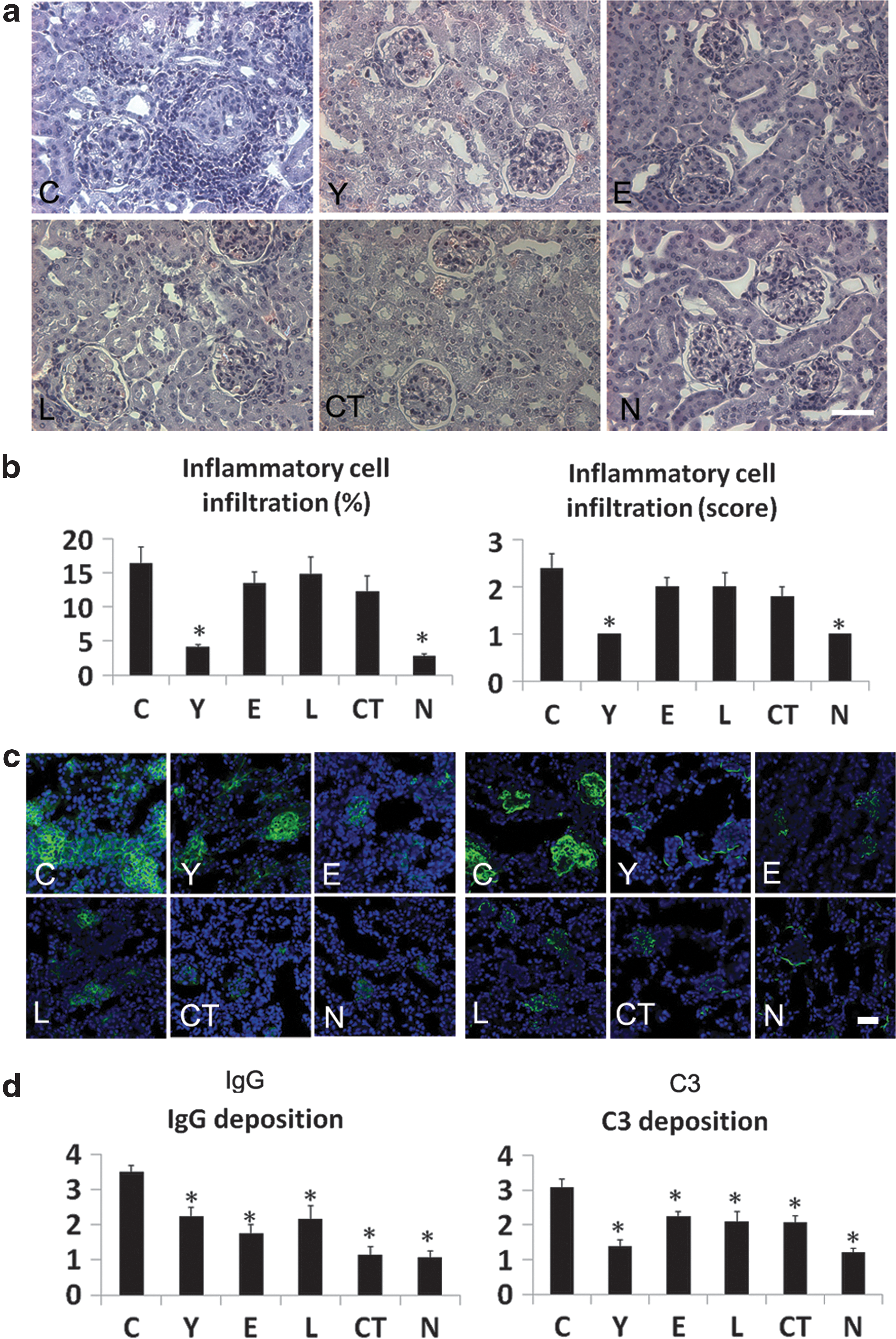
Histological staining and immunofluorescence of kidney samples.
Serum cytokines
The levels of IL-17 and IL-4 in sera from all treatment groups were significantly lower than those in the C group, collected at 24 weeks of age (Table 2). Levels of IFN-γ, IL-10, IL-1α, IL-1β, IL-2, IL-6, and TNF-α were statistically different between the groups, and the C group had the highest levels of cytokines. The levels of IL-6 and TNF-α in the Y and N groups were significantly lower than those in the C group, and other groups also had lower levels of cytokines than those in the C group, although these were not significantly different. IFN-γ/IL-4 (Th1/Th2) of the C, Y, E, L, CT, and N groups were 9.54±6.79, 0.63±0.18, 1.23±0.37, 5.98±3.13, 2.83±1.53, and 0.15±0.10, respectively. The ratio of Th1/Th2 cytokines was lower in the treatment groups compared with the control.
Data obtained from each group were compared using the Kruskal–Wallis test (
 P<0.05), followed by the Mann–Whitney U test (*).
P<0.05), followed by the Mann–Whitney U test (*).
*Significant (P<0.05) differences compared with the control (C group) are marked by an asterisk.
Skin extract cytokines
The skin extract levels of IL-4, IL-6, MIP-2, and TNF-α in the Y, E, CT, and N groups were significantly lower than those in the C group, and the skin extract levels of IL-1β in the E and CT groups were significantly lower than those in the C group (Table 2). The CT group showed the lowest average levels of IL-17 and IL-6 in skin extracts among the groups.
Micro-CT of the distal femoral metaphysis
Femurs (the distal femoral metaphysis) were removed from five mice from each group and were examined by micro-CT. The bone volume/total volume and trabecular number in the Y group were significantly lower than in the N group, and the trabecular spacing in the Y group was significantly greater than in the N group (Fig. 4). The trabecular number in the CT group was significantly higher than in the N group. There were no significant differences in these parameters between all other groups and the N group. Thus, cyclophosphamide treatment had a negative effect on trabecular bone integrity.

Micro-CT images from the distal femoral metaphysis. Representative micro-CT images of the distal femoral metaphysis and the bone volume/total volume and trabecular spacing scores from
Biodistribution
ASCs labeled with the CM-DiI red fluorescent tracker dye were present in the spleen, lymph node, kidney, liver, and skin. However, little evidence of cell fluorescence was found in the lung, heart, and brain (Fig. 5).

Biodistribution of transplanted ASCs. Three mice from the E, L, and CT groups were administered ASCs or CTLA4Ig-ASCs fluorescently labeled with conjugated red fluorophore Cell Tracker CM-DiI to allow identification in histopathological sections. The presence of CM-DiI-labeled cells was examined in various tissues, such as the spleen, lymph node, kidney, liver, lung, heart, brain, and skin (by counterstaining with mounting medium containing DAPI), with a laser scanning confocal microscope. Representative figures from each group are presented. Bar=50 μm.
Discussion
MRL/lpr mice develop a severe autoimmune disease, which resembles most clinical signs of human lupus. We evaluated the therapeutic effect of ASCs and CTLA4Ig-ASCs in MRL/lpr mice in comparison with cyclophosphamide treatment. According to a study on the long-term preservation of renal function in 111 patients with SLE and active glomerulonephritis (lupus nephritis), patients randomized to receive cyclophosphamide showed significantly better preservation of renal function than did patients who were randomized to receive prednisone only. The authors concluded that cyclophosphamide appears to provide a long-term benefit in the delay or prevention of end-stage renal disease in patients with lupus nephritis [20]. Many SLE studies using MRL/lpr mice also used cyclophosphamide as a positive control drug [21 –23]. Thus, we used cyclophosphamide as a positive control treatment drug because MRL/lpr mice develop a rapid and severe autoimmune syndrome characterized by excessive proliferation of autoreactive T lymphocytes.
B-cell over-reactivity leading to the overproduction of pathogenic autoantibodies is a fundamental event in the pathogenesis of SLE [1,24,25]. The cyclophosphamide treatment group had more favorable profiles with respect to serum anti-dsDNA antibodies and the proportion of CD138. Furthermore, ASC transplantation decreased the level of circulating anti-dsDNA antibodies. CD138 is expressed on B-cell precursors and plasma cells, and plasma cells generated during autoimmune responses are responsible for autoantibody production [26,27]. Thus, a reduction of CD138 cells may result in the suppression of anti-dsDNA antibody production.
Mice in the cyclophosphamide treatment group had the lowest level of kidney inflammation and glomerular infiltration of C3 (glomerulonephritis) and the lowest incidence rate of severe proteinuria. All other treatment groups had favorable levels in those parameters compared with the saline-treated control group.
MRL/lpr mice develop unique spontaneous skin inflammation, characterized by the liquefaction changes in basal keratinocytes, dermal T-cell infiltration, and IgG depositions at the epidermal–dermal junction (lupus band); these are similar to the cutaneous lesions of human lupus erythematosus [28]. Mice treated with ASCs or CTLA4Ig-ASCs starting from the early disease stage did not show dermatitis upon gross examination. ASC or CTLA4Ig-ASC transplantation led to a significant improvement in hyperkeratosis and inflammatory cell infiltration scores in histopathological sections. Furthermore, CTLA4Ig-ASC transplantation led to a significant decrease in acanthosis and IgG deposition in skin. The skin extract levels of IL-1β, IL-4, IL-6, MIP-2, and TNF-α in ASC and CTLA4Ig-ASC groups were also significantly lower than those in the control group. Thus, ASC or CTLA4Ig-ASC treatment prevented the development of spontaneous skin inflammation in MRL/lpr mice.
It remains controversial whether Th1 or Th2 cytokines contribute the most to the pathogenesis of skin lesions in SLE [29,30]. However, Th1-type IgG deposition was reported in human SLE [31]. It was also reported that a predominant Th1 cytokine response is related to the pathogenesis of lupus in both mice and humans [32]. In MRL/lpr mice, IgG2a and IgG3 are important subclasses involved in glomerulonephritis and are promoted by IFN-γ [33], whereas IgG1 is the major isotype involved in the pathogenesis of lupus dermatoses [34]. IL-4 induces B lymphocytes to switch from IgM to IgG1 production [35]. In this study, the pattern of cytokines in the skin of the saline-treated control group showed a Th2 shift with a 77-fold increase in IL-4 and only a 4-fold increase of IFN-γ compared with the background-matched normal group. IFN-γ and IL-17 play important roles in the initiation and development of lupus in MRL/lpr mice [36]. In our study, MRL/lpr mice treated with ASCs or CTLA4Ig-ASCs had a significant reduction in serum levels of IL-17 and IL-4, as well as a reduction in the level of IFN-γ and the ratio of Th1/Th2 (IFN-γ/IL-4) compared with the saline-treated control group. Therefore, systemic immune modulation following ASC transplantation might contribute to the improvement of disease in MRL/lpr mice, which is a commonly used SLE model. MSCs are considered an attractive alternative source for the treatment of tissue injury and immune-mediated diseases because of their differentiation capacity and production of various useful soluble factors, including trophic, chemoattractant, antiscarring, and immunomodulatory factors, such as prostaglandin E2 (PGE2), transforming growth factor-β (tumor growth factor-β, TGF-β), hemoxygenase-1 (HO-1), hepatocyte growth factor (HGF), 2, 3-dioxygenase (IDO), IL-10, human leukocyte antigen G (HLA-G), and leukemia inhibitory factor (LIF). These molecules exert antiproliferative effects on T cells or natural killer cells; HO-1 and LIF induce the generation of regulatory T cells, and PGE2 modulates the secretory profile of dendritic cells and macrophages [37,38]. Thus, the therapeutic effects of ASC transplantation on LE dermatitis might be due to the paracrine effects and immunomodulatory properties of ASCs.
In our previous study, we used another well-known SLE model, (NZB×NZW). In F1 female mice, serial ASC transplantation (from the early stage of disease) increased survival rates and decreased proteinuria [9]. We found increased serum levels of IL-4 and IL-10, and an increase in the proportion of CD4+Foxp3+ cells in the spleen. However, (NZB×NZW) F1 mice do not develop lupus dermatitis lesions like MRL/lpr, and the changing pattern of cytokine expression following ASC transplantation varies between the two strains. In MRL/lpr mice, the improvement of skin lesions after ASC or CTLA4Ig-ASC transplantation was remarkable, but the improvement of proteinuria, kidney lesions, or survival was relatively weak. ASC or CTLA4Ig-ASC transplanted mice had an increased proportion of Treg cells; however, this did not reach statistical significance. Functional defects in Treg, effector T, and antigen-presenting cells, as well as low expression of CTLA4 and CD80/86 molecules in MRL/lpr mice were reported [39]. Compared with ASCs, CTLA4Ig-ASCs showed significant synergistic therapeutic effects in improvement in the pathological score of dermatitis and IgG depositions in the skin and kidney and a decrease in skin IL-6 levels. Serial ASC transplantation started at an early stage of disease progression led to greater improvement of clinical symptoms than when started later in disease progression.
Cyclophosphamide treatment showed stronger therapeutic effects than ASC transplantation in MRL/lpr mice. However, using micro-CT analysis, we found that treatment with cyclophosphamide led to a significant reduction in bone volume and an increase in bone spacing in the trabecular bone. We confirmed that the use of cyclophosphamide reduced bone volume, even in background-matched control mice, MRL/MPJ (Fig. 4). Human SLE patients are also at increased risk of developing osteoporosis (
According to our recent case report, a dog patient with severe pruritus and anorexia was diagnosed as having pemphigus foliaceus based on its history, physical examination, and histopathology results of a skin biopsy. Treatment with prednisolone (2.2 mg/kg, PO, BID) and combination therapy of other immunosuppressive drugs (cyclosporine [5 mg/kg, PO, SID] and azathioprine [2 mg/kg, PO, SID]) had failed. Thus, the administration of canine CTLA4Ig-overexpressing allogeneic ASCs and/or ASCs was performed with the consent of the owner (21 times over a period of 20 months with an interval of 2–8 weeks). Prednisolone was gradually tapered concurrently and no relapse of the clinical signs was observed. After the termination of treatment, the skin lesions had improved and could be managed with a low dose of prednisolone (0.25 mg/kg, PO, SID) until recently. The body weight increased, and the abnormal clinical pathologic data (leukocytosis, anemia, and increased liver enzyme) and body condition were greatly improved [42].
Taken together, patients with immunosuppressant-resistant SLE or those who develop severe side effects to treatment, such as osteoporosis, may consider the use of ASCs as an alternative treatment option. These results also suggest the possibility of the use of ASCs for treatment of lupus dermatitis (patients with discoid lupus erythematosus).
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (NRF-2012R1A1A2006701) to E.W.C. Further support was provided by a grant from the Samsung Biomedical Research Institute (SMX1140141) to E.W.C.
Author Disclosure Statement
No competing financial interests exist.